

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
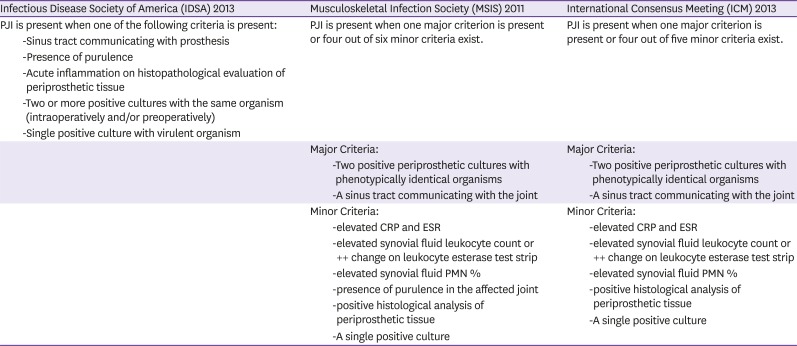
Total joint arthroplasty is a highly successful treatment modality that improves joint function, relieves pain, and increases the overall quality of life [1]. Prosthetic joint infection (PJI) is one of the most dreaded complications of arthroplasties, reported in 2–3% of patients undergoing primary total knee and hip arthroplasties in Korea [2]. With a projected increase in the number of primary or revision arthroplasties [34], more patients with PJI are anticipated in the future. PJIs are caused by organisms that grow on the surface of foreign bodies in biofilms and, in some cases, persist intracellularly in cells surrounding the implants. The majority of PJIs are initiated through inadvertent introduction of normal microbial flora at the time of surgery. Early PJI (i.e., within three months after arthroplasty) mainly results from infection with virulent organisms [5], whereas delayed (i.e., 3–12 months after arthroplasty) or late (>12 months after arthroplasty) PJIs tend to be associated with low-virulence bacteria, such as Staphylococcus epidermidis [6]. Biofilm-related infections are difficult to diagnose, as traditional microbiological tests are optimized to detect free-floating but not sessile bacteria. Diagnosis relies on a combination of clinical suspicion, clinical assessment, synovial fluid biomarker analysis, appropriately performed cell cultures, histology, and, in some cases, additional testing. Various definitions of PJI have been used between studies evaluating diagnostic tests for PJI, potentially affecting comparability of results. In an effort to standardize the definition of PJI, multiple medical societies and working groups have proposed definitions. In 2011, the Musculoskeletal Infectious Society (MSIS) proposed a set of criteria for the diagnosis of PJI that was later revised at the International Consensus Meeting (ICM) on PJI [78] (Table 1). In 2013, the Infectious Disease Society of America (IDSA) published a set of criteria for the definition of PJI [9]. However, these definitions are slightly different between each other. [6]. In recent years, extensive research efforts into biomarker identification have been performed [1011], and new definitions of periprosthetic hip and knee joint infection have been suggested or are in formulation [12].
Table 1
Proposed definitions of prosthetic joint infection
Diagnosis of PJI remains a challenge to the orthopedic community, at least in some cases. According to a publication from the Korea knee research group, diagnosis of PJI is based on clinical suspicion in one-third of cases, without joint fluid and histological analysis [13]. Recently, diagnosis of PJI has been greatly improved, due to application of molecular techniques. In this article, we review PJI diagnostic strategies with methods available in Korea using the ICM PJI definition.
Diagnosis
1. Clinical suspicion
Clinical presentations of PJI are diverse depending on the time of onset following prosthesis placement, mechanism of infection, virulence of the pathogen, and host immune response. Chronic PJI has an indolent course characterized by persistent joint pain, with or without early implant failure [9]. Joint pain is also the most common symptom in aseptic failure. Therefore, clinical suspicion based on a patient's constellation of clinical symptoms and risk factors for infection is important to decide upon the most appropriate diagnostic testing strategy. When patients have postoperative wound healing complications, such as prolonged wound drainage, wound dehiscence, wound hematoma, or lack of resolution of joint pain after primary surgery, the possibility of PJI increases [14]. Joint erythema, tenderness, and systemic findings, such as chills and fever, are highly specific for infection but are rarely observed except in hematogenous PJI or early infections [15]. A sinus tract that communicates with prosthesis is considered by most investigators to be specific, definitive evidence of PJI, and has been considered diagnostic in all three definitions (Table 1). Thorough history and physical examination improve the accuracy of diagnostic tests, but are dependent on the expertise of the evaluating clinician.
2. Biomarkers in the serum: erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), procalcitonin, interleukin (IL)-6
Several preoperative tests are available to assist in the assessment of PJI. ESR and CRP are the most frequently used inflammatory markers and are determined through inexpensive, widely available, noninvasive tests with rapid turnaround time in most laboratories that have now been incorporated in the routine evaluation of PJI (Table 1). Values greater than 30 mm/h for ESR and greater than 10 mg/L for CRP have been proposed for PJI diagnosis [8]. Infections with low-virulence organisms, prior antimicrobial use, and immunosuppression may be associated with normal inflammatory markers [16]. CRP and ESR can be elevated during the post-operative period and in renal disease, malignancy, advanced age, and chronic inflammatory conditions such as rheumatoid arthritis and metallosis [17]. Serum procalcitonin levels have been useful for other infections but have been investigated in only a small number of patients for PJI diagnosis. One study involving 78 patients found that serum procalcitonin was specific (98%), but not sensitive enough (33%) [18]. Therefore, procalcitonin is not currently recommended for PJI diagnosis. IL-6 is a cytokine produced by monocytes and macrophages that has been shown to be useful in the diagnosis of PJI. In a meta-analysis, IL-6 was shown to have a higher diagnostic odds ratio (314.7) when compared with ESR and CRP [19].
3. Synovial fluid studies - cell count and differential, IL-6, α-defensin
If clinical signs and symptoms, and blood tests suggest the possibility of PJI, the next step is fluid aspiration from the joint. Synovial fluid can be obtained through preoperative or intraoperative aspiration. Synovial fluid aspiration of a knee arthroplasty is easily performed in the office, but aspiration of a hip arthroplasty may require fluoroscopic guidance. The amount of synovial fluid obtained during aspiration does not correlate with the presence or absence of infection. Synovial fluid should be submitted for determination of nucleated cell counts and percentages of neutrophils and for bacterial aerobic and anaerobic cultures. Specific cutoffs for synovial fluid leukocyte counts have been recommended for diagnosis of PJI, which are lower than those reported for native septic arthritis. The cutoff value for a positive test varies across joint-types and time of onset of PJI, and is also affected by the presence of underlying inflammatory arthritis. Leukocyte counts >1,100/mm3 provided a sensitivity and specificity of 90.7% and 88.1%, respectively, in one study of 429 patients with knee arthroplasties (including 161 PJIs) [20]. A smaller study by Trampuz et al. of 133 patients (34 with PJI) with knee arthroplasties found that a leukocyte count >1,700 cells/ mm3 showed sensitivity and specificity of 94% and 88%, respectively [21]. The optimal cutoff values for synovial fluid leukocyte counts and neutrophil percentages appear to be higher in hip than in knee arthroplasties. A study of 201 hip arthroplasties (including 55 PJIs) found that a leukocyte count >4,200 cells/ mm3 provided a sensitivity and specificity of 84 and 93%, respectively [22]. A more recent study of 810 patients with knee or hip arthroplasties (including 146 PJIs) found that a count of >3,450 leukocytes/mm3 was 91% sensitive and 93% specific, and that a neutrophil percentage >78% was 95% sensitive and 87% specific [23]. According to the MSIS PJI definition, a synovial fluid leukocyte counts of >3,000/mm3 and a neutrophil percentage of >80% indicate hip or knee arthroplasty infection. Notably, IDSA diagnostic criteria do not include specific values for synovial fluid leukocyte counts or leukocyte differential. Because synovial cell counts may be elevated in periprosthetic fractures, inflammatory arthritis, and allergies to metals, interpretation must be careful. By combining results of synovial fluid cell count and differential, with those of culture, ESR, and CRP, the sensitivity of PJI detection can be improved up to 99.7% [16].
Some biomarkers can be elevated in various inflammatory conditions. In theory, synovial fluid biomarkers, which are obtained directly from the affected joint, may be more accurate for PJI diagnosis than serum biomarkers. A relatively recent development includes synovial fluid analysis for identification of novel biomarkers, such as α-defensin and IL-6 [11]. One study that evaluated the sensitivity, specificity, and accuracy of 24 synovial fluid biomarkers in patients with PJI versus aseptic failure reported that synovial fluid IL-6 had excellent diagnostic performance, with an accuracy over 0.9 for the diagnosis of hip and knee PJI [7]. This finding corresponds well with the results of a recent study reporting that synovial fluid IL-6 had an accuracy of 0.89, with very high sensitivity, thus leading to strong diagnostic strength [24]. Synovial fluid IL-6 as a predictor of shoulder PJI had 87% sensitivity and 90% specificity with an area under the curve of 0.891 and an ideal cutoff value of 359.3 pg/mL [25]. Defensins are endogenous peptides of the host-defense innate immune system that are released mainly from polymorphonuclear cells in response to pathogens. Several studies have considered the role of α-defensin in the evaluation of painful hip and knee replacements with a sensitivity and specificity approaching 100% [2627]. These results have not been replicated for shoulder replacements, with sensitivity dropping to 63% [28]. A recent study showed that α-defensin can be falsely positive in conjunction with an underlying non-infectious inflammatory disease, mainly in cases with crystal deposition [29]. The detection of synovial fluid α-defensin with enzyme-linked immunosorbent assay (ELISA) is commercially available under the name SynovasureTM (Zimmer, Warsaw, IN, USA) PJI test, but not yet available in Korea. At least 1.0 mL of synovial fluid is required for analysis and the stability of α-defensin in synovial fluid is 48 h at room temperature [26]. The test has been validated for the detection of PJI with a cutoff value of 5.2 µg/mL, providing a signal-to-cutoff ratio of 1.0.
4. Intraoperative periprosthetic purulence and histology
IDSA and MSIS guidelines consider intraoperative purulence as a diagnostic criterion for PJI. However, with concerns regarding the subjective interpretation of purulence and the possibility that noninfectious causes of arthroplasty failure, such as reactions to metal debris and crystal-induced arthritis, can induce a purulent-like fluid response, the ICM omitted purulence from their diagnostic criteria.
Histopathology is highly specific in predicting culture-positive PJI and therefore confirming the presence of infection [30]. Histopathological evaluation of PJI involves tissue sampling from the areas adjacent to the prosthesis that appear to be infected upon intraoperative inspection. Different thresholds for acute inflammation have been proposed, but the presence of at least 5 neutrophils per high power field (×400 magnification) in at least 5 microscopic fields is one of the most common definitions used. Intraoperative frozen section evaluations can provide useful information to surgeons at the time of revision surgery, with the caveat that, as with assessment of purulence, non-infectious conditions, such as inflammatory arthritis or periprosthetic fracture, may provide false-positive results [31]. In addition, histology may be false-negative when infection is due to a low-virulence microorganism, such as a coagulase negative Staphylococcus species or Cutibacterium acnes [32].
5. Culture of synovial fluid, periprosthetic tissue and sonicate fluid
Aspirated synovial fluid can be inoculated into blood culture bottles at the time of collection or first transported to the microbiology laboratory and inoculated into blood culture bottles; alternatively, synovial fluid may be inoculated into solid and/or into liquid media. Recent studies recommended that synovial fluid should be inoculated into paired aerobic and anaerobic blood culture bottles for ideal diagnosis of PJI [3334].
Multiple periprosthetic tissue samples should be collected and submitted for aerobic and anaerobic culture at the time of operation. Single-tissue specimens for culture should be avoided because of low sensitivity and difficulty in interpreting potential contamination with low-virulence microorganisms [35]. The number of cultures required for optimal detection of pathogens has recently been re-defined. The IDSA guidelines recommended that at least three and optimally five or six periprosthetic intraoperatively-collected tissue samples should be submitted for aerobic and anaerobic cultures [9]. A single positive culture may be important, especially when a virulent organism such as S. aureus, a beta-hemolytic Streptococcus species, or an aerobic gram negative bacillus is isolated, or when the same organism is found in the synovial fluid and the sonicate fluid. The specific media and incubation time for periprosthetic tissue culture have been examined to a limited extent [36]. Previous microbiological techniques for periprosthetic tissue culture have used aerobic and anaerobic blood agar plates, alongside broths, such as thioglycolate broth. One recent large study involving 178 patients compared the sensitivities and specificities of four different culture media to a gold standard for the detection of acute inflammation in periprosthetic tissue. Cultures using cooked meat broth (83%) or blood culture bottles (87%) were more sensitive than cultures using fastidious anaerobic broth (57%) or solid-agar plates (39%) [37]. Newly published studies have shown that culture of periprosthetic tissue specimens in blood culture bottles improved diagnosis; additionally, it required fewer specimens (three specimens) than cultures using conventional plates and broths, for accurate PJI diagnosis; culture in blood culture bottles is also labor- and cost-saving [38394041]. In the majority of studies, the incubation period was in the order of 5 days for aerobic cultures and 14 days for anaerobic cultures. Schafer and Butler-Wu recommended an incubation period of 14 days based on late recovery of Cutibacterium/Propionibacterium species [4243].
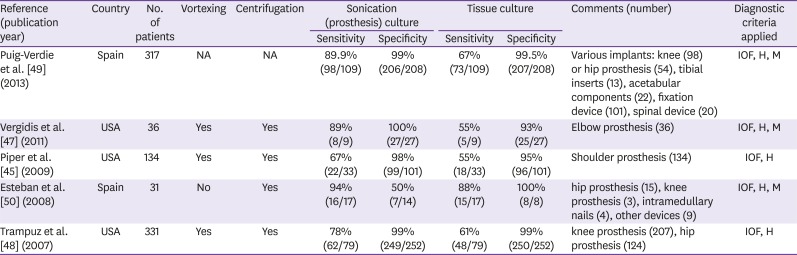
Sonication fluid culture has emerged as a practical and effective method to dislodge biofilms and the associated bacteria from the surface of implants [44]. Sonicate culture should be accompanied by the use of solid rather than liquid media, to enable semi-quantitative analysis, which is not possible when a broth medium is used. A recommended protocol for sonication of explanted joint prostheses is shown in Figure 1. Plating onto aerobic and anaerobic sheep blood agar plates, the microorganisms are enumerated and identified by routine microbiological techniques. According to Mayo Clinic guidelines, sonication fluid cultures are positive when at least 20 colony-forming units are grown per plate (0.1 mL inoculum equals 10 mL of original sonicated sample) [4546]. Sonication has been studied on hip, knee, shoulder, and elbow prostheses, with a range of observed diagnostic accuracies reported (Table 2) [4547484950]. A recent meta-analysis of clinical trials showed that sonication fluid culture is of greater value for PJI diagnosis than traditional tissue culture [5152]. A recent study demonstrated that periprosthetic tissue culture sensitivity in blood culture bottles was similar to that of sonication fluid culture; however, the two tests combined had the highest sensitivity without compromising specificity [39].
Figure 1
Prosthesis sonication protocol used in the Mayo Clinic Clinical Microbiology Laboratory (Courtesy of David Lynch, reproduced with permission).
The implant is collected in a sterile container and 400 mL Ringer's solution is added followed by rigorous mixing (vortex). Vortex of the sample for 30 s before sonication increases the yield of positive cultures. Following vortex, the container was sonicated (40 kHz) in an ultrasound bath for 5 min. After sonication, sonicate fluid is vortexed for 30 s again, followed by centrifugation; for example, 50 mL aliquots are centrifuged at 3,150 g for 5 min, and the whole supernatant, but the bottom 0.5 mL, is discarded. As shown in Figure 1, after the concentration step, the supernatant is aspirated and 0.1 mL of the precipitate is plated onto aerobic and anaerobic sheep blood agar plates, which are incubated at 37°C in 5% CO2 aerobically and anaerobically for 5 and 14 days, respectively.
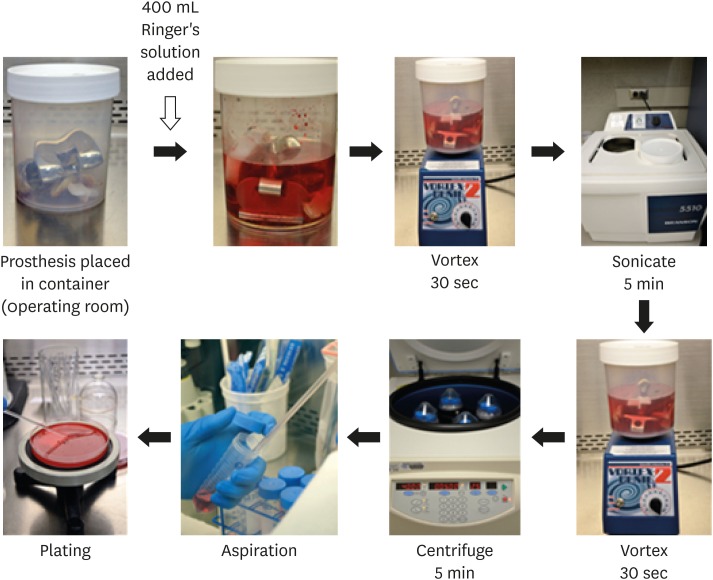
Table 2
Comparative studies of sonication culture with tissue culture and yield of positive cultures in patients with orthopedic implant-associated infection
| Reference (publication year) | Country | No. of patients | Vortexing | Centrifugation | Sonication (prosthesis) culture | Tissue culture | Comments (number) | Diagnostic criteria applied | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Sensitivity | Specificity | |||||||
| Puig-Verdie et al. [49] (2013) | Spain | 317 | NA | NA | 89.9% (98/109) | 99% (206/208) | 67% (73/109) | 99.5% (207/208) | Various implants: knee (98) or hip prosthesis (54), tibial inserts (13), acetabular components (22), fixation device (101), spinal device (20) | IOF, H, M |
| Vergidis et al. [47] (2011) | USA | 36 | Yes | Yes | 89% (8/9) | 100% (27/27) | 55% (5/9) | 93% (25/27) | Elbow prosthesis (36) | IOF, H, M |
| Piper et al. [45] (2009) | USA | 134 | Yes | Yes | 67% (22/33) | 98% (99/101) | 55% (18/33) | 95% (96/101) | Shoulder prosthesis (134) | IOF, H |
| Esteban et al. [50] (2008) | Spain | 31 | No | Yes | 94% (16/17) | 50% (7/14) | 88% (15/17) | 100% (8/8) | hip prosthesis (15), knee prosthesis (3), intramedullary nails (4), other devices (9) | IOF, H, M |
| Trampuz et al. [48] (2007) | USA | 331 | Yes | Yes | 78% (62/79) | 99% (249/252) | 61% (48/79) | 99% (250/252) | knee prosthesis (207), hip prosthesis (124) | IOF, H |
Absence of bacterial growth has been reported in up to 14% of patients with clinical evidence of PJI [6]. In general, PJI caused by mycobacteria and fungi is rare, and routine use of mycobacterial and fungal cultures is not cost-effective in Western countries [53]. In a literature review, Million and colleagues reported that, out of 301 cases of culture-negative PJI, 46% were due to fungi, 43% due to mycobacteria, and 11% due to bacteria [54]. In Korea, the prevalence of Mycobacterium
tuberculosis infection is not low [55] and routine mycobacterial culture may be useful. If fungal or mycobacterial infection is suspected, proper specimen transport and isolation media should be used. Adequate numbers of samples, strict withholding of antimicrobials prior to surgery and improvements in microbiological techniques may decrease the number of culture-negative infections. Antimicrobial agents should be held until cultures are collected, if the patient is not systemically ill.
6. Future diagnostics: Molecular methods
Culture-negative PJIs are challenging in terms of management, so new laboratory methods that improve the microbiological diagnosis of PJI are required. The use of polymerase chain reaction (PCR) technology has the theoretical advantage of a rapid turnaround time and ability to detect culture-negative cases. In the context of PJI diagnosis, two main categories of PCR assays exist, specific PCR and broad-range PCR assays [5657]. Specific PCR assays target single bacterial species (e.g., S. aureus) or a group of closely related species (e.g., Staphylococcus species) or multiple specific genes combined with detection of common resistance genes such as mecA for MRSA, or vanA, vanB, or bla
KPC. Specific PCR assays have been used with commercial or laboratory-designed PCR primers [46585960]; recently, these are typically real-time PCR assays. A rapid panel PCR showed better performance in an evaluation using sonication fluid [46] but not using periprosthetic tissue or synovial fluid [5861]. However, panel PCR may show limited sensitivity with relation to multiplex PCR design, which can only detect pathogens included in the primer setup [62]. Broad-range bacterial 16S rRNA PCR targets regions of the bacterial rRNA gene conserved across species [63]. The specific identity of the source bacteria in broad–range assays is determined by analyzing the sequence of the amplified DNA. Mixed sequence data, resulting from mixed infection, may be resolved by several strategies, including cloning of the PCR amplicon and sequencing of a limited number of clones or with next generation sequencing. The main limitations of broad-range bacterial PCR relate to inherent sensitivity issues. The use of next-generation sequencing techniques allows for the generation of thousands of individual sequences from a single broad-range PCR reaction and this approach may provide detailed information on the bacterial population present in prosthetic joint samples [6465].
Conclusions
Joint arthroplasties are life-enhancing and the number of arthroplasties is increasing. Accordingly, more infectious complications are expected, but, clinical data or research regarding PJI is lacking in Korea. Major contributions in the advancements of PJI diagnosis have been made in the recent years. All current diagnostic tests have inherent limitations that require the combination of different testing modalities for ideal clinical care. Laboratorians, orthopedic surgeons, and infectious disease specialists should cooperate to accomplish accurate diagnosis of PJI. Improved diagnostics for PJI is anticipated over the following years. While waiting for the advent of new technologies, clinicians should make an effort to follow strategies that can be used to enhance the yield of culture techniques.
 XML Download
XML Download