

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Coffee and green tea are among the most widely consumed beverages worldwide. These beverages contain more than 1,000 chemicals, and many observational studies and randomized control trials (RCTs) have evaluated the association between their intake and various health outcomes.1 Coffee and green tea contain antioxidants such as polyphenols, which reportedly reduce the risk of cancer and cardiovascular diseases.23 However, some studies have shown that tea and coffee, which contain compounds such as caffeine, can increase the risk of diabetes or osteoporosis.45
The ingredients in coffee affects the absorption of nutrients from the gut.6 Morck et al.7 reported that iron absorption following a meal decreased by an average of 39% after consuming coffee. Following this initial report, this observation has been confirmed in numerous randomized intervention studies in both humans and animals.891011
Tea also has a strong inhibitory effect on the absorption of non-heme iron, which accounts for 70–90% of dietary iron.1213 The absorption rate of non-heme iron is lower than that of heme iron, but it constitutes one-third of all of the iron stored in the body.14 Inhibition of iron absorption can ultimately lead to iron deficiency, the most common micronutrient deficiency in adults.15 According to the Korean National Health and Nutrition Examination Survey (KNHANES), 2.0% of males and 22.4% of females in Korea do not meet the recommended daily allowance of iron.16 Thus, in Koreans with habitually low iron intake, the health effects of inhibiting iron absorption by drinking coffee or tea may be greater than in populations with adequate dietary iron intake. However, studies on the effects of coffee and tea intake on iron absorption are limited in the Korean population. Therefore, this study aimed to evaluate the effect of intake of coffee and green tea intake on serum iron status, as indexed by serum ferritin levels in Korean adults.
MATERIALS AND METHODS
1. Study design and population
Data was obtained from the Korean National Health and Nutrition Examination Survey (IV and V; 2007–2012). The KNHANES is a nationally representative survey of the non-institutionalized Korean civilian population conducted by the Korea Centers for Disease Control and Prevention.17 In the KNHANES IV and V, lifestyle, medication use, food frequency questionnaire (FFQ), 24-hour dietary recall, and past medical history data were collected by a trained investigator. Of the 38,005 subjects aged 19 years and over, FFQ or 24-hour dietary was surveyed among 34,308 subjects. In final analysis, 27,071 of the subjects were included, with 7,237 being excluded due to missing data.
2. Coffee and green tea consumption
In this study, we used data on the frequency of coffee and green tea consumption, as surveyed by the FFQ. In the FFQ of KNHANES IV and V (2007–2011), there are 10 consumption frequency categories-never or rarely, 6–11 times a year, once a month, 2–3 times a month, once or twice a week, 2–3 times a week, 4–6 times a week, once a day, twice a day, and 3 times a day. In the FFQ of KNHANES V (2012), there are nine consumption frequency categories-never or rarely, once a month, 2–3 times a month, once a week, 2–4 times a week, 5–6 times a week, once a day, twice a day, and 3 times a day. Coffee and green tea intake was reclassified into four categories-less than once a day, once a day, twice a day, and 3 times a day.
3. Measurement of serum ferritin
Serum ferritin level was measured by an immunoradiometric assay using a 1470 Wizard Gamma Counter (PerkinElmer, Turku, Finland).18
4. Covariates
Information on covariates, such as alcohol consumption, smoking status, physical activity, education level, comorbidities and daily iron intake, was obtained in interviews with the study subjects. Subjects' weight and height were measured in light clothing and without shoes. Alcohol intake was classified as-consumption of ≥1 standard drink per week and <1 standard drink per week. Smoking status was classified as current smoker or non-smoker. Physical activity was classified as moderate physical activity for ≥30 minutes at least 5 days per week, or less than that. Education level was coded as middle school or below, high school, or college or above. Comorbidity status, including of hypertension and diabetes was classified according to whether a diagnosis had ever been made by a doctor or not. Daily iron intake was calculated based on 24-hour dietary recall data and the Food Composition Table developed by the National Rural Resources Development Institute.
5. Statistical analysis
A multivariate linear regression was performed to evaluate the relationship between coffee and green tea consumption and serum ferritin levels. Log transformation of serum ferritin levels was necessary because of the highly skewed distribution. Dietary iron intake were calorie-adjusted using the residual method.19 A multiple linear regression model was fitted with log-transformed serum ferritin level as the dependent variable, and with the following covariates included: age, body mass index (BMI), education level, smoking status, alcohol consumption, physical activity, hypertension, diabetes mellitus, and calorie-adjusted daily iron intake. All analyses were conducted using Stata software (ver. 14.0; Stata Corp, College Station, Texas, USA).
RESULTS
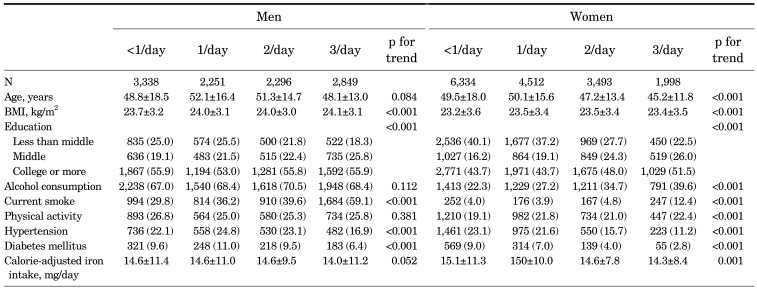
The general characteristics of the participants according to coffee intake are summarized in Table 1. Subjects of both sexes with higher coffee intakes had a higher BMI, higher education level, and higher smoking rate, together with a lower prevalence of hypertension and diabetes mellitus. The women with higher coffee intake were also younger, and had higher alcohol intake, and had higher levels of physical activity.
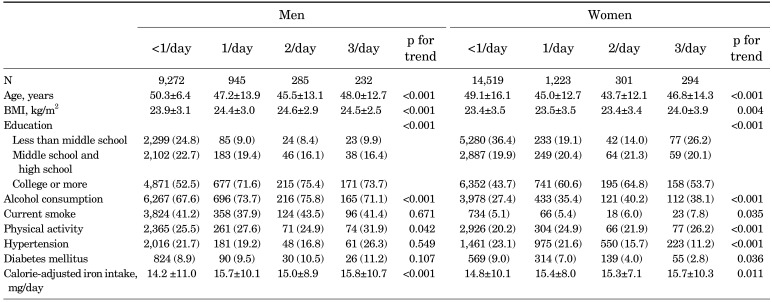
The general characteristics of the participants according to green tea intake are summarized in Table 2. Subjects of both sexes with higher green tea intake were younger, and had a higher BMI, higher education level and physical activity levels, and higher alcohol intake, and higher calorie-adjusted daily iron intakes. Subjects with higher green tea intake had a higher smoking rate and, in women, a lower prevalence of hypertension and diabetes.
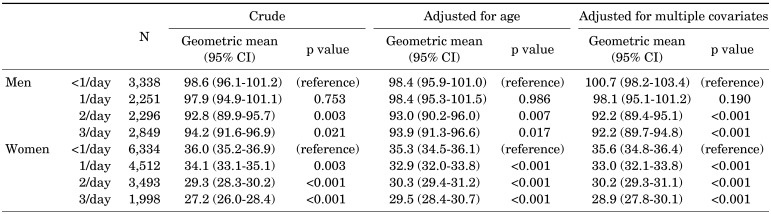
The geometric mean concentration of serum ferritin decreased with increasing coffee intake (Table 3). After adjusting for potential confounders, the serum ferritin level increased with coffee intake in males but decreased in females. In men, the geometric mean serum ferritin level was 100.7 ng/mL (95% confidence interval [CI]: 98.2–103.4) with <1 coffee /day, 98.1 ng/day (95% CI: 95.1–101.2) with 1 coffee/day, 92.2 ng/mL (95% CI: 89.4–95.1) with 2 coffees/day and 92.2 ng/mL (95% CI: 89.7–94.8) with ≥3 coffees/day. In women, the equivalent values were 35.6 ng/mL (95% CI: 34.8–36.4), 33.0 ng/mL (95% CI: 32.1–33.8), 30.2 ng/mL (95% CI: 29.3–31.1), and 28.9 ng/mL (95% CI: 27.8–30.1).
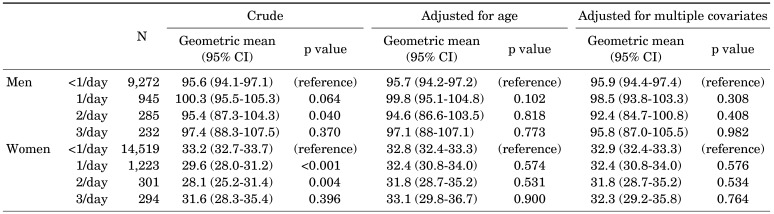
The geometric mean concentration of serum ferritin did not differ with green tea intake in either sex (Table 4), with or without adjustment for potential confounders.
DISCUSSION
This is the first nationwide study to assess the relationship between coffee intake and serum ferritin levels in the adult Korean population. Compared to participants who drank coffee less than once a day, those who drank it three times a day exhibited low serum ferritin levels, of 8.5 ng/mL (8.4%) in men and 6.7 ng/mL (18.9%) in women. These inverse relationships remained statistically significant after adjustment for confounders and calorie-adjusted daily iron intake.
In our study, the higher coffee intake was correlated with a higher BMI and a lower prevalence of hypertension and diabetes. When adjusted for age, education level, smoking history, and alcohol intake, the relationship of coffee intake with BMI and diabetes was still significant. Interestingly, a significant relationship was observed between hypertension and coffee intake, but only in women. The relationship between coffee intake and BMI as well as diabetes was similar to that observed in previous studies. In a meta-analysis of prospective cohort studies, Carlstrom and Larsson20 reported that the risk of diabetes decreased by 6% when coffee consumption increased by one beverage a day. In the Copenhagen General Population Study (CGPS) and the Copenhagen City Heart Study (CCHS), a linear relationship between BMI and coffee intake in cross-sectional analyses was reported, although coffee intake was not associated with BMI in a Mendelian randomization study.21 The association between coffee consumption and hypertension has been inconsistent among RCTs and cohort studies.22
Previous studies evaluating the correlation between blood markers associated with iron metabolism and coffee and tea intake are also inconsistent. Coffee intake was negatively associated with serum ferritin level in the Framingham Heart Study.23 However, in an RCT aiming at an intervention for discontinuing coffee intake, Dewey et al.11 reported no difference in plasma hemoglobin, iron or ferritin levels between the intervention and control groups. When iron supplements were administered to subjects with iron deficiency, the increase in plasma ferritin was greater in the group that stopped drinking coffee.11 In NHANES II, Mehta et al.24 assessed the relationship between coffee and tea intake and anemia. Coffee and tea consumption were negatively associated with anemia. The odd ratios with five cups of coffee or tea was 0.975 (95% CI: 0.975–0.976).24 The mechanism by which coffee consumption affects iron metabolism can be explained as follows. First, polyphenols contained in coffee bind iron and form insoluble complexes that inhibit iron absorption.25 This occurs only in non-heme iron, while heme iron is not affected.1012 In our study, serum ferritin was reduced by 8.4% in males, and by 18.8% in females, in to subjects drinking ≥3 coffee a day compared to those drinking <1 coffee a day. In a previous study reporting that one third of the total iron store is non-heme iron, coffee intake reduced the absorption of non-heme iron by 40%.7 Since the bioavailability of non-heme iron is low, increased coffee intake has a relatively modest reducing effect on serum ferritin levels in our study, somewhat in line with previous studies. Second, drinking beverages with meals reduces the bioavailability, and thus also the absorption, of iron.26
In this study, coffee, but not green tea, intake was associated with serum ferritin levels. The results of previous studies evaluating the relationship between green tea intake and serum ferritin have not been consistent. Mennen et al.9 reported no significant association between green tea intake and serum ferritin levels in a study involving French adults, but in a study on Japanese males conducted by Imai and Nakachi27, there was a significant relationship between serum ferritin and green tea intake. However, in a cross-sectional study of Chinese females, Root et al.28 reported that tea intake was not associated with plasma ferritin. The heterogeneous results may be due to difference in types of tea and participant dietary habits among studies. Production and brewing methods, and the foods consumed with these beverages, may all affect the iron absorption;29 further studies are required to fully assess the impact of these variables on serum ferritin levels.
The aim of this study was to assess the effect of coffee and green tea on iron absorption, after adjusting for the calorie-adjusted iron intake, using a large-scale data representative of the adult Korean population. Although limited by our incomplete understanding of the causal relationships between the variables in this cross-sectional study, the results are still significant. Another factor to consider when designing future studies is that serum ferritin levels in women are influenced by menstruation30 although this was not included as a confounder.
In conclusion, we found that an increase in coffee intake was associated with a decrease in serum ferritin levels. Our results suggest that regular coffee consumption may be associated with iron deficiency anemia in Korean adults.
 XML Download
XML Download