

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although atherosclerotic cardiovascular disease (ASCVD) risk prediction algorithms currently play an important role in identifying high-risk patients who may benefit from preventive intervention, a large proportion of cardiovascular events occur in women whose 10-year estimated ASCVD risk is <7.5%.1)2) Therefore, additional strategies beyond the measurement of traditional risk factors are needed to identify women who might benefit from medical therapy based on unexpected higher risk.
Breast arterial calcification (BAC) is a type of medial calcification easily detected on standard mammography. Evidence over the past several decades suggests that BAC correlates with the risk of cardiovascular disease (CVD). In addition, there has been interest in whether the presence of BAC can improve cardiovascular risk assessments. Given that millions of women undergo mammography, a significant relationship between BAC and CVD would provide an opportunity to improve risk stratification without additional cost and radiation exposure.3)
In this review, we summarized existing evidence that shows a correlation of the presence of BAC on mammography with several traditional CVD risk factors and with prevalent and incident CVD. In addition, we briefly introduced the new data that investigated whether BAC can predict subclinical coronary artery disease (CAD) on coronary computed tomography angiography (CCTA) and that evaluated the potential utility of BAC for refining risk assessment in asymptomatic Korean women based on the 10-year ASCVD risk.
EVALUATION OF BAC
The Korean guidelines for breast cancer screening recommends biennial screening mammography in asymptomatic women aged 40 to 69 years (grade B recommendation), and it also recommends selective screening mammography in women aged 70 years or older according to individual risk and preference (grade C recommendation).4)
BAC on mammography is recognized by its typical tram-track appearance (two parallel linear calcifications), which is distinct from ductal calcification. Most BAC findings have been omitted in formal reporting because BAC is not related to breast cancer.
Normal mammography with BAC would be categorized in the Breast Imaging Reporting and Data System (BI-RADS) as category 1 (negative) or 2 (benign finding).5) To calculate a BAC score, the number, length, and density of BAC are evaluated. The number of calcified vessels in both breasts is recorded; if more than six calcified vessels are detected, the radiologist counts them as six. A vessel is counted as one if it is visible in both cranial-caudal and mediolateral-oblique views. The longest length of calcified vessel is scored using a 4-step scale (0, none; 1, less than 1/3; 2, between 1/3 and 2/3; and 3, more than 2/3). The calcification density of the vessel in the densest segment is scored using 4-step scale (0, none; 1, vessel wall calcification with clear visualization of the lumen and/or single wall calcination; 2, vessel wall calcification with clouding of the lumen; and 3, dense vessel wall calcification without visualization of the lumen) (Figure 1). To evaluate the severity of BAC, radiologists sum these three scores for each woman, and these BAC severity scores are categorized into three groups (0, 1 to 6, and 7 to 12).
Figure 1
Scoring system of breast arterial calcification (BAC) density. The calcification density of the vessel in the densest segment is scored using 4-step scale. White arrow indicates calcification segment. (A) 0, none, (B) 1, vessel wall calcification with clear visualization of the lumen and/or single wall calcination, (C) 2, vessel wall calcification with clouding of the lumen, (D) 3, dense vessel wall calcification without visualization of the lumen.

In the recent report, there was good agreement between readers for the BAC score (intraclass coefficient = 0.71, 95% confidence interval [CI]: 0.60–0.79) and substantial agreement for the presence of BAC (κ = 0.76, p < 0.001).3)
PREVALENCE AND RISK FACTORS OF BAC
BAC prevalence varies widely depending on the heterogeneity of the studied population and variations in the sensitivity of mammography equipment; ranging from 10% to 12% in healthier population-based cohort studies to 60% to 70% among women aged >70 years or with chronic kidney disease.6)
The systematic review and meta-analysis by Hendriks et al.7), showed BAC prevalence around 12.7% among women in breast cancer screening programs. Increasing age (pooled odds ratio [OR]: 2.98, 95% CI: 2.31–3.85 for every 10 years), diabetes (pooled OR: 1.88, 95% CI: 1.36–2.59), and parity as opposed to nulliparity (pooled OR: 3.43, 95% CI: 2.23–5.27) are associated with higher BAC prevalence. Smoking is associated with lower BAC prevalence (pooled OR: 0.48, 95% CI: 0.39–0.60). No associations were found with hypertension, obesity or dyslipidemia.
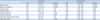
In the registry that enrolled 2,100 asymptomatic Korean women aged older than 40 years, BAC prevalence was reported as 9.5%.3) The risk factors of BAC were revealed as age, number of parities, diabetes mellitus, and body mass index in the univariable analysis and were in accordance with previous studies. However, only age and number of parities remained statistically significant after multivariable analysis (Table 1).
Table 1
Univariable and multivariable analyses to determine the factors associated with breast arterial calcifications in the BBC registry
ASSOCIATION OF BAC AND CORONARY ATHEROSCLEROSIS
Table 2 summarizes current evidence of the association between BAC and coronary atherosclerosis.3)8)9)10)11)12)13)14)15)16)17)18)19)20)21)22)23)24)25) Initially, several studies examined the relationship of BAC with coronary atherosclerosis based on a coronary angiography diagnosis. The results were inconsistent across the studies and a 5-study meta-analysis by Abi Rafeh et al.26), including nearly 1000 women, demonstrated that patients with BAC had a 1.59-fold increased risk of CAD by angiography. However, it should be noted that, since these studies were performed in women who received clinically-indicated invasive coronary angiography, the study populations were limited to patients with suspected CAD, and were very small in size
Table 2
Association of breast arterial calcification with coronary atherosclerosis

| Author, year | n | Age | Modality | Conclusion |
|---|---|---|---|---|
| Moshyedi, 19958) | 182 | 39–92 | CA | BAC in women aged less than 59 years may indicate an additional risk factor for CAD, particularly in diabetic patients. |
| Henkin, 20039) | 319 | 50–70 | CA | The presence of BAC does not differentiate between patients with angiographic evidence of CAD and those with angiographically normal coronary arteries. |
| Topal, 200710) | 123 | > 40 | CA | There was a significant increase in the frequency of BAC among subjects with more than two vessels with stenosis. |
| Fiuza Ferreira, 200711) | 131 | 42–81 | CA | A strong association exists between intramammary arterial calcifications and CAD (adjusted OR: 4.6). |
| Penugonda, 201012) | 94 | 66.7 (mean) | CA | BAC was not positively associated with cardiovascular risk factors, documented CAD, or acute cardiovascular events, suggesting that BAC is not a useful predictor of CAD in intermediate-to high-risk patients. |
| Zgheib, 201013) | 172 | 64.3 (mean) | CA | The authors did not observe a correlation between BAC and coronary angiography-detected CHD, even when CHD severity was considered. |
| Hekimoğlu, 201214) | 55 | > 40 | CA | A significant relationship between intramammarian arterial calcifications and CAD was indicated (OR: 10.8, 95% CI: 3.02–38.59). |
| Ružičić, 201815) | 102 | > 45 | CA | In women > 45 years, there was a significant correlation between the severity of CAD as evaluated by the SYNTAX score and BAC as evaluated by the Likert scale. |
| Pecchi, 200316) | 74 | < 65 | MSCT | Positive association with CAC |
| Linear correlation between BAC severity and coronary calcium content | ||||
| Maas, 200717) | 499 | 49–70 | MSCT | Positive association with CAC |
| Matsumura, 201318) | 202 | 30–90 | MSCT | Positive association with high-risk CAC score (CAC > 400) |
| Moradi, 201419) | 150 | > 40 | CCTA | No significant correlation of presence and severity of BAC with CAC score |
| Newallo, 201520) | 195 | 46–59 | CCTA | Positive association with increased probability of coronary calcification, atherosclerosis, and CAD on CCTA |
| Mostafavi, 201521) | 100 | 34–86 | CCTA | The presence of BAC on mammography appears to correlate with CAD as determined by CCTA. |
| The inclusion of BAC as a feature in CAD prediction significantly increased classification results. | ||||
| Chadashvili, 201622) | 145 | 56–61 | CCTA | Prediction of coronary artery calcium score of > 11 |
| Significant correlation between BAC and cardiac risk factors, namely diabetes and chronic renal disease | ||||
| Margolies, 201623) | 292 | 39–92 | MSCT | Strong quantitative association with CAC |
| Equivalent to both the FRS and PCE for the identification of high-risk women and additive when women with established CAD are included. | ||||
| Yoon, 20183) | 2,100 | > 40 | CCTA | Association of the presence and severity of BAC with the risk of subclinical CAD in asymptomatic women |
| Independent and incremental value over conventional risk algorithms | ||||
| Kelly, 201824) | 104 | 50–65 | CCTA | BAC diagnosed on 2 yearly screening mammography predicts CAD-RADS ≥ 3 disease in symptomatic patients. |
| Fathala, 201725) | 435 | 58 (mean) | MPS | The presence and severity of BAC on screening or diagnostic mammography do not predict myocardial ischemia on stress MPS. |
BAC: breast arterial calcification, CAG: coronary angiography, CAC: coronary artery calcification, CAD: coronary artery disease, CAD-RAD: coronary artery disease-reporting and data system, CCTA: coronary computed tomography angiography, CHD: coronary heart disease, CI: confidence interval, FRS: Framingham risk score, MPS: myocardial perfusion single-photon emission computed tomography, MSCT: multi-slice computed tomography, OR: odds ratio, PCE: pooled cohort equation.
The general utility of coronary artery calcification scoring (CACS) has been risk prognostication by directly visualizing coronary artery calcification (CAC) as a marker of subclinical heart disease.27)28) As demonstrated in the previous study, higher CACS is associated with higher risk of coronary heart disease (CHD) events.29)30)31) The presence of CAC has also been used to justify a more aggressive CAD risk-factor modification treatment, including aspirin, statins, and lifestyle modifications.32)33)
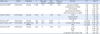
The association of BAC with CAC in several studies is also summarized in Table 3.34)35)36)37)38) With the exception of the study by Moradi et al.19), published studies point to a significant relationship of BAC with CAC. However, these data have limitations and should be interpreted with caution because of the small sample sizes and possible selection bias, since most studies recruited women who had already been referred for computed tomography (CT).33) In addition, there were differences in the methods for measuring CAC and CAC scoring thresholds across the studies.
Table 3
Longitudinal studies that examined the association between BAC and cardiovascular disease
| Author, year | Nation | Population | n | Mean age (years) | BAC prevalence | Follow-up (years) | Outcome | HR | 95% CI |
|---|---|---|---|---|---|---|---|---|---|
| Kemmeren,199834) | Netherlands | General | 12,239 | 57.5 | 9.1% | 16.8 | All-cause mortality | 1.29 | 1.06–1.58 |
| Cardiovascular mortality | 1.29 | 1.01–1.66 | |||||||
| CHD mortality | 1.44 | 1.02–2.05 | |||||||
| Cerebrovascular mortality | 0.88 | 0.49–1.61 | |||||||
| Other cardiovascular mortality | 1.38 | 0.89–2.16 | |||||||
| Iribarren, 200435) | United States | General | 12,761 | 56 | 3.0% | 24.8 | CHD | 1.32 | 1.08–1.60 |
| Ischemic stroke | 1.41 | 1.11–1.78 | |||||||
| Heart failure | 1.52 | 1.18–1.98 | |||||||
| Schnatz, 201136) | United States | General | 1,454 | 56.3 | 16.3% | 5 | CHD | 3.54 (OR) | 2.28–5.50 |
| Abou-Hassan, 201537) | United States | End stage renal disease | 202 | 58.3 | 58.4% | 4.1 | Coronary artery disease | 1.06 (OR) | 0.48–2.38 |
| PAD | 4.56 (OR) | 1.20–17.3 | |||||||
| Hendriks, 201538) | Netherlands | General | 1,540 | 57 | 8.6% | 13.2 | CHD | 1.44 | 1.02–2.01 |
| Stroke | 1.39 | 0.92–2.08 | |||||||
| PAD | 1.37 | 0.74–2.52 | |||||||
| Composite of CHD, stroke, PAD | 1.39 | 1.00–1.93 |
Margolies et al.23) studied 292 women who had mammography with a non-gated chest CT within a year and determined CAC in a semi-quantitative way. BAC demonstrated a quantitative association with CAC and was superior to standard cardiovascular risk factors for the prediction of CAC. However, the investigators failed to demonstrate a statistically significant incremental value of BAC to the conventional risk stratification algorithm.
A recent investigation by Yoon et al.3) was the first and largest study to evaluate the association between BAC and subclinical CAD, including both CAC and coronary atherosclerotic plaque (CAP), as evidenced by CCTA. The Women Health Cohort for Breast, Bone and Coronary Artery Disease (the BBC cohort) included 2,100 asymptomatic women aged older than 40 years who participated in general health check-ups (ClinicalTrials.gov Identifier: NCT03235622).The presence and severity of BAC was associated with the presence of CAC and CAP after adjusting for traditional cardiovascular risk factors. In addition, the evaluation of BAC provided an independent and incremental value over conventional risk algorithms. For the prediction of CAC and CAP, the addition of BAC presence to the ASCVD risk prediction algorithm significantly increased the areas under the curve (0.71 to 0.72, p = 0.016; and 0.66 to 0.68, p = 0.010, respectively) and resulted in net reclassification index improvements (0.304, p < 0.001; and 0.245, p < 0.001, respectively). Further studies regarding relationship between BAC and CAP composition or long-term follow up results according to the presence or severity of BAC will shed light on the causal relationship between BAC and CHD.
BAC AND LONGITUDINAL CARDIOVASCULAR OUTCOMES
Longitudinal studies that have examined the relationship between BAC and cardiovascular outcomes have been scarce and are summarized in Table 3.34)35)36)37)38)
Kemmeren et al.34) reported the relationship between BAC and cardiovascular mortality in a cohort of 12,239 women aged 50 to 68 years who participated in a population-based breast cancer screening project (DOM Project) in Utrecht, the Netherlands, during the period 1975-1977. Mortality data from 16-19 years of follow-up were available. The hazard ratio for overall mortality, mortality from CVD, and death from CHD were 1.29 (95% CI: 1.06–1.58), 1.29 (95% CI: 1.01–1.66) and 1.44 (95% CI: 1.02–2.05) in women with BAC detected on screening mammograms compared to women without BAC after correction for cardiovascular risk factors including age, diabetes mellitus, hypertension, parity, Quetelet index, and smoking.
Iribarren et al.35) used either hospital admission data or municipal death records to examine the association of BAC and CVD events. The authors reported hazard ratios of 1.32 (95% CI: 1.08–1.60) for incident CHD, 1.44 (95% CI: 1.02–2.05) for CHD mortality, 1.29 (95% CI: 1.01–1.66) for CVD mortality, and 1.52 (95% CI: 1.18–1.98) for heart failure after adjusting for age, race, education level, body mass index, total serum cholesterol, cigarette smoking, alcohol consumption, hypertension, diabetes, family history of myocardial infarction, number of live births, early menarche, and hormone replacement therapy.
Schnatz et al.36) found that women who were BAC positive had a 3.5-fold increased risk for CHD (OR: 3.54, 95% CI: 2.28–5.50, p = 0.001) when they evaluated the development of any CHD after 5 years among those who were CHD negative at baseline and controlling for age.
Contrary to other studies that analyzed women who participated in a breast cancer screening program, Abou-Hassan et al.37) reported the clinical implication of BAC in patients with end-stage renal disease (ESRD). In this study, BAC was found in 58% of the study participants and was significantly associated with age, diabetes, and ESRD duration. Both coronary artery (27% vs. 15%) and peripheral arterial disease (PAD) (19% vs. 4%) were more likely in patients with BAC compared to those without BAC, but only PAD persisted after accounting for other factors (OR: 4.6, 95% CI: 1.2–1.5).
Recently, Hendriks et al.38) reported a series of case–cohort studies nested within the larger Prospect-EPIC (European Prospective Investigation into Cancer and Nutrition) cohort study. The presence of BAC was significantly associated with CHD (HR: 1.44, 95% CI: 1.02–2.01) and combined CVD including CHD, stroke, and PAD (HR: 1.39; 95% CI: 1.00–1.93), during 13.2 years (median) of follow-up after adjusting conventional cardiovascular risk factors such as age, body mass index, physical activity, high density lipoprotein/ total cholesterol ratio, smoking and pulse pressure. Larger effect sizes were found for severe BAC, with HRs of 3.37 (95% CI: 1.80 to 6.31) for combined CVD and 3.40 (95% CI: 1.76 to 6.57) for CHD compared with women without BACs.
BAC appear to be associated with an increased risk of CVD events, while only being associated with some of the known cardiovascular risk factors, illustrating that medial arterial calcification might contribute to CVD through a pathway distinct from the intimal atherosclerotic process.39) Medial calcification may lead to CVD through increased arterial stiffness because BAC could be a marker of a more generalized tendency to develop medial calcification in other vascular beds.37)38) The lack of distensibility may lead to higher peak pressures in distal vessels, resulting in damage and remodeling and exacerbation of ischemia produced by co-existing atherosclerosis. Stiffening of the large arteries may also promote atherosclerosis by altering flow characteristics.40)
Despite existing evidence that suggests BAC is a risk factor for subclinical and clinical CVD, it is important to note that most of prior studies have relied on conventional film mammography. Therefore, further research is needed to examine the association of BAC with CVD risk factors and CVD events using digital mammographic techniques that have a much greater sensitivity level.40) The Multiethnic Study of Breast Arterial Calcium Gradation and Cardiovascular Risk (MINERVA) cohort study will yield novel insights into ethnic differences in BAC presence and gradation, and factors associated with BAC. In addition, no study to date has quantified BAC mass and its relationship with CVD risk factors and events, MINERVA may elucidate the role of BAC mass in the prediction of CVD and determine whether adding BAC mass to prediction model based on traditional risk factors improves the classification of risk for total CVD and its components.40)41)
LIMITATIONS AND FUTURE INVESTIGATIONS
First, there remains uncertainty regarding the exact causality and pathophysiologic mechanism of BAC, although previous studies have suggested a correlation of BAC with cardiovascular risk factors or with increased arterial stiffness.
Second, there are currently no guidelines regarding the reporting of BAC, therefore, it is often omitted. BAC should instead be treated as any other clinically relevant incidental finding, and be mentioned in the conclusion of the mammogram report to help clinicians assess cardiovascular risk.6)
Third, before BAC can be used to facilitate personalized decision-making for aggressive prevention, randomized controlled trials of an integrated screening and targeted prevention strategy are required.
CONCLUSION
BAC is associated with prevalent or incident CVD and subclinical coronary atherosclerosis. It could provide an independent and incremental predictive value over conventional risk factors. Further studies are warranted to evaluate whether the evaluation of BAC in asymptomatic women translates into long-term clinical benefits.
 XML Download
XML Download