

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although the incidence of gastric cancer is slightly decreasing, it is still one of the most common malignancies and a major cause of cancer-related death in Korea [12]. However, biannual cancer screening programs have identified a large proportion of early-stage gastric cancer patients and increased their overall survival rate. With the increase in survival rates, many surgeons and patients are more focused on the early postoperative recovery and quality of life. Therefore, there has been an increase in the incidence of laparoscopic gastrectomy (LG) than open gastrectomy (OG) [34].
End-stage renal disease (ESRD) can be cured with renal transplantation. Through the development of dialysis techniques and kidney transplantation, the total survival rate of ESRD patients has increased. However, some patients with ESRD develop gastric cancer. ESRD patients were once regarded as high-risk patients for any operative procedure [5678910]. If the advantages of a laparoscopic approach can be adopted for gastric cancer patients with ESRD, surgical results can be improved. However, the intra-abdominal CO2 gas insufflation and long duration of high pneumoperitoneum pressure might affect the hemodynamic status and postoperative course of ESRD patients who cannot continuously modulate their volume status. In addition, their tissue status and wound healing processes may be weakened. No study currently addresses the role of laparoscopic radical gastrectomy in ESRD patients. Therefore, this study aimed to evaluate both the short- and long-term surgical outcomes of ESRD patients undergoing LG and OG.
MATERIALS AND METHODS
Patients
From January 2004 to November 2014, 38 ESRD patients in 7 hospitals affiliated with the Catholic Medical Center in South Korea underwent radical gastrectomy due to gastric adenocarcinoma. They were divided into the LG and OG groups, and the surgical approaches were selected based on each surgeon's preference. The surgeries were performed by 7 different surgeons. Each surgeon performed >300 OG and LG cases during the study period.
A patient with oliguria or anuria receiving regular dialysis (hemodialysis [HD] and peritoneal dialysis [PD]) or with a glomerular filtration rate (GFR) of <15 mL/min/1.73 m2 based on the most recent laboratory analysis prior to surgery was defined as having ESRD. Patients who underwent palliative or non-curative resection or had a neoplasm in other organs were excluded. The clinicopathological results and early surgical and long-term survival outcomes were compared between the 2 groups. We adopted the Charlson Comorbidity Index (CCMI) to compare various comorbidities of ESRD patients [11]. In 1987, M.E. Charlson developed CCMI, which was the most cited comorbidity index in the literature, and has been validated in a number of studies [1213]. Ethical approval was obtained from the Institutional Review Board of the Catholic University of Korea College of Medicine (XC17REDE0072).
Operative methods and postoperative evaluations
Gastric resections included total and distal gastrectomies, with D1+ to D2 lymph node dissection (LND) performed according to the third Japanese gastric cancer treatment guidelines [14]. The type of approach and method of reconstruction were selected based on the surgeon's preference and patient's condition. The extent of resection and LND followed the Japanese treatment guidelines. Closed drains were placed in the Morrison's pouch in all patients following surgery. Moreover, surgical outcomes including the clinicopathological characteristics, number of retrieved lymph nodes (LNs), operation time, estimated blood loss volume, morbidity and mortality rates within 30 days postoperatively, time to first oral intake, and length of postoperative hospital stay were assessed based on a prospectively collected database. Postoperative morbidity was classified according to the Clavien-Dindo (CD) classification [15], and the Comprehensive Complication Index (CCI) [16] was calculated to compare the severity of each patient's multiple postoperative complications.
Statistical methods
The statistical analyses were performed using the SPSS 18.0 software (SPSS Inc., Chicago, IL, USA). The collected data are expressed as median values and interquartile ranges (25–75th percentile) for non-parametric continuous variables, means±standard deviations for parametric continuous variables, and frequencies with percentages for nominal variables. The χ2 or Fisher's exact test was used for nominal variables. Additionally, the Mann-Whitney U test was used for non-parametric variables, and the Student's t-test was used for parametric continuous variables. A 2-tailed P-value of 0.05 was considered statistically significant. Survival curves were estimated using the Kaplan-Meier method and compared using the log-rank test.
RESULTS
A total of 38 patients (OG: 21 patients, LG: 17 patients) were included in this study. They constituted 0.37% of all patients who underwent curative radical gastrectomy from January 2004 to November 2014. No significant differences were noted on the sex, age, body mass index, cause of renal failure, and type of dialysis between the 2 groups. Diabetes was the most common cause of renal failure in both groups (OG: 47.6%, LG: 47.1%). In the OG group, 16 patients (76.2%) underwent HD and 4 patients (19.0%) had PD. Meanwhile, in the LG group, HD and PD were performed in 13 (76.5%) and 3 (17.6%) patients, respectively. No significant difference was observed in the CCMI between the 2 groups (Table 1).
Table 1
Patients' characteristics between the 2 groups

Based on the surgical outcomes, there were no differences in the extent of resection, reconstruction type, LND, or number of retrieved LN (Table 2). In the LG group, 7 patients underwent laparoscopy-assisted subtotal gastrectomy, 8 underwent totally laparoscopic subtotal gastrectomy, and 2 underwent totally laparoscopic total gastrectomy. LG patients had less estimated blood loss volume (OG vs. LG: 275 vs. 94 mL, P=0.005). The operation time (OG vs. LG: 200 vs. 190 minutes, P=0.340) and duration of hospital stay (OG vs. LG: 12 vs. 11 days, P=0.617) were similar for both groups. Of the 38 patients, 29 patients (76.3%) were on HD, 7 patients (18.4%) were on PD, and the remaining 2 patients started HD in the early postoperative period. The PD patients required longer operation time compared to the HD patients, although this was insignificant (PD vs. HD: 232.1 vs. 210.4 minutes, P=0.415). No significant differences were noted in the postoperative complications of PD and HD patients (PD vs. HD: 42.9% vs. 37.9%, P=1.000).
Table 2
Operative outcomes between the 2 groups

7 patients (OG vs. LG: 33.3% vs. 41.2%, P=0.873) from each group developed postoperative complications (Table 3). Complications were observed in 4 patients (19.0%) in the OG group and 5 patients (29.4%) in the LG group, which were classified as CD grade IIIa or higher. With the exception of a mortality case, there were 2 cases of morbidity in the OG group: duodenal stump leakage and bacteremia caused by methicillin-resistant Staphylococcus aureus (MRSA). In the LG group, 1 patient each developed anastomosis leakage and bleeding, pleural effusion, and chylous ascites. Wound infection was observed in 19.0% (n=4) of the OG group and 11.8% (n=2) of the LG group. Of these patients, wound infection of 1 patient in the OG group was classified as CD grade IIIa, and complications of the remaining 5 patients were CD grade II. The CCI for each group was similar (OG vs. LG: 9.5±17.1 vs. 11.7±16.8, P=0.711). Postoperative mortality was noted in 2 cases in the OG group and 1 case in the LG group. In 2 OG patients, the causes of death were postoperative recurrent intra-abdominal bleeding due to candida infection and multi-organ failure caused by MRSA infection. 1 patient in the LG group expired because of septic shock during duodenal stump leakage.
Table 3
Morbidities and mortalities following gastrectomy in 2 modalities
Survival result
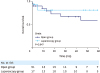
No significant difference was noted in the overall survival between the 2 groups (Fig. 1, P=0.947). The 3-year overall survival rate was 82.4% in the LG group and 71.4% in the OG group. Moreover, the 5-year overall survival rate was 82.4% in the LG group and 64.7% in the OG group. The median follow-up period was 51 months (range: 5–122 months). During the follow-up period, 14 patients (36.8%) died (8 in the OG group, 6 in the LG group). 2 patients in each group died because of gastric cancer. Among them, 3 patients died of immediate postoperative complications and 1 died of gastric cancer recurrence. Additionally, 5 OG patients and 4 LG patients died of aggravated renal failure. 1 patient died of prostatic cancer 94 months following gastrectomy (Table 4).

DISCUSSION
In the present study, laparoscopic radical gastrectomy in ESRD patients was not inferior to OG in terms of the short- and long-term survival results. LG had less intraoperative blood loss volume; however, both groups involved LND and had a similar extent of resection. The operation time, duration of hospital stay, postoperative morbidity, and long-term survival rate were similar in both groups. In general, ESRD is considered to be a major risk factor for postoperative morbidity and mortality in major abdominal surgeries [5671017]. The morbidity rate of all ESRD patients in our study was 36.8%. This rate is higher than that of non-ESRD patients in previous reports, ranging from 14.7%–21.2% [181920]. Although LG is a popular procedure for patients with gastric cancer regardless of the stage, its influence in chronic kidney disease (CKD) or ESRD patients has not been reported. In this study, we focused on analyzing the safety and oncologic feasibility of LG in ESRD patients with impaired hemostatic function and wound healing undergoing radical LND and bowel anastomosis.
Matsumoto et al. [18] reported that the severity of CKD was associated with an increase in surgical complications and a higher surgical mortality rate following radical gastrectomy. They classified 177 patients with CKD into 2 groups according to GFR (mild CKD: GFR of 30–59 mL/min/1.73 m2; severe CKD: GFR <29 mL/min/1.73 m2). Systemic complications and in-hospital mortality increased as the CKD stages became more severe. Anastomosis leakage, intra-abdominal abscess, and wound infection were more common in both CKD groups. LG was performed in 29 patients (16.3%) and was not associated with severe postoperative complications. A recent study comparing 108 patients divided into the CKD and non-CKD group demonstrated the influence of this disease on gastric cancer surgery [19]. The CKD group was defined as patients with an estimated GFR (eGFR) of <60 mL/min/1.73 m2. The CKD patients showed no significant differences compared with the non-CKD group. The relapse-free survival rates of the 2 groups were similar but only 13 patients from this study had severe CKD (eGFR <30 mL/min/1.73 m2). Another study retrospectively analyzed 26 patients with ESRD after radical gastrectomy; however, no information on laparoscopic procedures was shown [20]. To the best of our knowledge, this study is the first to analyze the safety of laparoscopic radical gastrectomy in ESRD patients.
ESRD patients have underlying cardiovascular comorbidities such as hypertension, atherosclerosis, and hyperlipidemia. They are known to be vulnerable to major perioperative cardiac complications [1821]. Patients who underwent LG will endure high pneumoperitoneum pressure during the operation; therefore, they are exposed to perioperative hemodynamic instability and pulmonary complications. However, the effect of intra-abdominal CO2 gas insufflation on CKD patients has not been investigated. In the present study, no major cardiac complications occurred in either LG or OG group, and only 1 patient in the LG group had a pleural effusion requiring percutaneous drainage. Although more studies are required, ESRD patients seem to tolerate intra-abdominal CO2 gas insufflation for about 200 minutes of laparoscopic procedure. Uremia and malnutrition in ESRD patients cause platelet dysfunction that leads to decreased hemostatic function [1922]. Intraluminal anastomosis bleeding occurred in 2 (11.8%) LG patients and 1 OG patient expired due to recurrent bleeding after the third operation. Moreover, increased bleeding tendency in ESRD patients increases the difficulty of D2 LND. The technically feasibility, safety, and oncological outcome of LND up to the D2 level is challenging for surgeons, especially in advanced gastric cancer. Approximately 52.6% underwent D2 LND and an adequate number of patients with LN (OG: 30.0%, LG: 26.5%) were retrieved. However, the safety of radical LND in ESRD patients should be validated by further studies.
Liu et al. [20] reported that one of the major causes of complications in 26 ESRD patients undergoing radical gastrectomy is anastomosis leakage. The rate of anastomotic leakage in CKD patients was more than two-fold that of the normal population, and CKD was also an independent risk factor for esophagojejunal anastomotic leakage. In our study, 1 case of esophagojejunostomy leak after LG (5.9%) was observed, and each group had 1 patient with duodenal stump leak (OG: 4.8%, LG: 5.7%). In this case, the LG patient died. With the immune response deficiency in ESRD patients, the anastomotic leakage easily leads to fulminant infections. Surgeons should pay attention when performing the anastomosis in gastrectomies involving ESRD patients, especially when performing esophagojejunostomy in total gastrectomy.
Seven patients (18.4%), including 4 in the OG group and 3 in the LG group, were on PD at the time of gastrectomy, and although insignificant, the PD patients required longer operation time compared with the HD patients. This may be caused by the presence of intra-abdominal adhesions induced by repetitive PD and handling of the indwelling PD catheter. The incidence of postoperative complications was similar in both groups (PD vs. HD: 42.9% vs. 37.9%, P=1.000) but 2 OG patients who expired were on PD. 1 LG patient showed chylous ascites through a closed drain that spontaneously improved with a low-fat diet. 1 patient from each group did not have the PD catheter removed during the gastrectomy and resumed PD after the operation. The patient who underwent LG was admitted 1 year after gastrectomy due to an adhesive ileus that was managed conservatively. A recent review cited that the use of laparoscopic techniques was effective in continuing PD in the early postoperative period by reducing peritoneal membrane stress, preserving peritoneum integrity, and decreasing the risk of postoperative dialysis fluid leakage [23].
Iannuzzi et al. [17] analyzed the database from the American College of Surgeons National Surgical Quality Improvement Program in 2013 and reported that bowel resection in patients with ESRD conferred a high mortality risk and that laparoscopy was associated with a reduced postoperative morbidity. Although most parts of this study include both small bowel and colon surgery, the authors presumed that laparoscopic surgery resulted in an attenuated surgical stress response and better preservation of the cell-mediated immune response. Furthermore, it is associated with a quicker return to baseline through reduced postoperative pain, earlier mobilization, and return of bowel function. Although the only significant advantage in the present study was the reduction of intraoperative blood loss volume, there were some better outcomes in operation time and postoperative hospital stay. Some positive influences of LG in the postoperative outcomes of ESRD patients can be found. With innovations in minimally invasive surgery, more favorable evidence will be gathered on the effects of LG on ESRD patients.
In the survival analysis, there was little difference between the 2 groups (P=0.947). The main causes of death were caused by the complications of ESRD or early surgical mortalities, not the recurrence of carcinoma (Table 4). This result demonstrates that limited LND and resection in ESRD patients seem to be more reasonable than performing an extensive radical procedure that strictly follows the guidelines. ESRD itself has a poor prognosis, with the average survival of 60-year-old patients with ESRD reported as 5.5 years and that of 65-year-old patients as 4.3 years [24]. In this aspect, laparoscopic procedures can provide better safety to ESRD patients without compromising long-term survival or prognosis.
There are some limitations to our study. First, a relatively small number of patients were enrolled. Second, the number of surgeons that participated in our study was relatively large in relation to the number of patients. The disparity of the surgeons' surgical skills may have affected the consistency of surgical outcomes. Third, the OG group had a relatively large proportion of advanced stage gastric cancer patients and patients who underwent total gastrectomy. These factors introduced a degree of heterogeneity of surgical procedure and might influence the short- and long-term surgical outcomes. Finally, the study was designed retrospectively. Study limitations are probably attributed to the paucity of operable gastric cancer patients with ESRD. To date, this study includes the highest number of ESRD patients who underwent radical gastrectomy. With more experience and well-designed multi-centered studies, the influence of LG on ESRD will be more clearly elucidated.
In conclusion, LG showed comparable short- and long-term surgical outcomes in ESRD patients than OG. With careful consideration in terms of patient selection and preparation for operation, laparoscopic procedures might be safely adopted in ESRD patients so they can benefit from the advantages of minimally invasive surgery.
 XML Download
XML Download