

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Nonrecurrent laryngeal nerve (NRLN) is a rare anomaly representing a major risk factor for injury during thyroid surgery. Due to its unique anatomical position, it may be misdiagnosed and damaged. This damage may potentially cause subsequent vocal cord paralysis, decreasing overall physical as well as psychological quality of life.
Both the recurrent laryngeal nerve (RLN) and NRLN provide innervation to all intrinsic laryngeal muscles, with the exception of the cricothyroid muscle. Providing sensory input, either the RLN or NRLN innervates the mucosal surface of the larynx inferior to the vocal cords. As a result, injury to this nerve may produce ipsilateral vocal cord paralysis, resulting in permanent hoarseness. However, if bilateral lesions are present, aphonia, and life-threatening dyspnea may potentially occur following medial placement of the paralyzed vocal cords and subsequent obstruction of the glottis. For these reasons, proper identification and procedural preservation of RLN or NRLN are critical for patients receiving neck surgery.
To prevent injury of RLN or NRLN during thyroid surgery, many surgeons now commonly utilize intraoperative neuromonitoring (IONM). Indeed, IONM has gained wide-spread acceptance as a therapeutic adjunct to the gold standard of visual nerve identification. Further, previous studies have demonstrated that IONM significantly improves clinical outcomes following thyroidectomy, preserving individual voice performance as well as reducing the incidence of vocal cord palsy (12).
Emerging as an alternative to conventional surgery, transoral thyroid surgery significantly reduces surgical incisions and scarring, endoscopically inserted through the mouth and into the thyroid. Previous reports have proposed surgical anatomy as the rationale for transoral endoscopic thyroid surgery, performing transoral thyroidectomy on human cadavers (34). Further, several investigations have adopted endoscopic or robotic thyroidectomy utilizing a vestibular approach in live patients (56). Recently, we encountered a thyroid cancer patient with right NRLN receiving transoral robotic thyroidectomy via the vestibular approach in combination with IONM.
CASE REPORT
1. Clinical presentation
Physical screening of a 44-year-old female patient identified a nodule in the right thyroid lobe. Subsequent ultrasound revealed a solitary nodule 7 mm in size over the right lobe of the thyroid. Results of fine-needle aspiration cytology were indicative of papillary carcinoma. No other masses or enlarged lymph nodes were detected during either physical examination or following imaging of the neck, by both ultrasound and computed tomography (CT) scan. Further, CT scan identified an aberrant right subclavian artery arising from the distal aortic arch, suggesting the presence of a NRLN (Fig. 1).

2. Operative method
The operative techniques utilized were similar to those previously described by Lee et al. (6). Specifically, the patient received endotracheal intubation with electromyographic surface electrodes integrated for monitoring. No additional neuromuscular blocking agents were utilized following intubation. The patient was laid in the lithotomy position, with both legs extended; slight neck extension was achieved utilizing a thyroid pillow. Skin and oral cavity preparation, as well as surgical draping was performed in accordance with standard protocols. Skin marking and epinephrine administration were conducted at the operation field. Blunt dissection was performed utilizing a vascular tunneler, running from the midline portion of mandible to the sternal notch. A midline port was inserted through the midline vestibular incision and 2 additional ports were inserted at either side, lateral to the midline incision. Subsequently, the right axillary port was inserted. Next, the strap muscles were dissected from the right lobe surface. Following dissection of middle thyroidal vein, superior pole dissection and ligation was performed. The thyroid gland was retracted medially and the suspensory ligament of Berry was dissected to identify the right NRLN with IONM. Following identification of the right NRLN, a complete right lobectomy was performed. The specimen was contained in an endoscopic bag and removed through the oral midline incision. Following hemostasis and irrigation, both fibrin glue as well as an anti-adhesive barrier was applied at the operation field. A J-P drain was inserted via the right axillary port and midline incision closure was achieved utilizing continuous 3-0 V-lock suture. The incision was closed in one layer and an aseptic dressing was applied.
3. Operative and postoperative findings
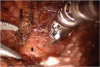
During the operation, the right vagus nerve was identified and stimulated by a nerve stimulator. However, movement of the vocal cords was not detectable. A NRLN was definitively identified utilizing IONM in the proximity of the Berry ligament (Fig. 2). Specifically, this nerve emanated from the right vagus nerve almost at a right angle and entered the larynx (Fig. 3). Importantly, the nerve did not follow a recurrent course and, as a result, was spared from surgical injury. The post-operative period was uneventful, and laryngoscopic examination demonstrated normal vocal cord movement.

DISCUSSION
Significant variation has been reported regarding the incidence of NRLN in the general population. In the largest series reported, comprised of 6,637 observations of the RLN during neck surgery, the frequency of NRLN was 0.54% (17 cases in 3,098) on the right and 0.07% on the left (2 cases in 2,846), corresponding to a mean prevalence of 0.32%. The embryological basis for this finding is proposed to stem from a vascular disorder termed arteria lusoria characterized by abnormal absorption of the fourth right aortic arch (7). Consequently, when the heart descends and the neck elongates during embryonic development, this vessel fails to draw the right RLN in the caudal direction (8). This anatomic anomaly generally produces a right subclavian artery originating as a branch off the normal aortic arch, travelling upward and to the right behind the esophagus. Interestingly, the incidence of this vascular malformation in the general population is reportedly as high as 0.5% to 2% of Attmann et al.'s study (9). Theoretically, the pre-operative diagnosis of a NRLN could be easily determined utilizing imaging studies, CT scans, or magnetic resonance imaging to visualize the arteria lusoria. In the case of our patient, preoperative CT scan demonstrated aberrant right subclavian artery arising from the distal aortic arch, indicating NRLN.
Drawing from previous investigation, NRLN can be categorized into 3 subtypes (10). In type 1, the NRLN runs with the superior vascular pedicle of the thyroid gland. In type 2a, the NRLN travels superior to the trunk of the inferior thyroid artery. In type 2b, the NRLN passes either inferior to the trunk or between the branches of the inferior thyroid artery. In our patient, the NRLN was classified as type 2a because the NRLN passed superior to the trunk of the inferior thyroid artery. The dissection during transoral robotic thyroidectomy progresses in the cranio-to-caudal direction so that the vagus nerve superior to origin of NRLN was difficult of access and we could not detect movement of the vocal cord during vagal nerve stimulation in this case.
Transoral robotic thyroidectomy represents a recent advance in thyroid surgery. Although investigations validating the feasibility of this procedure have been conducted on cadavers (34), few case reports are available regarding the performance of transoral robotic thyroidectomy on live patients (6). Although robotic thyroidectomy through trans-axillary or chest wall access routes produces minimal scarring, these procedures involve substantial surgical dissection. Conversely, utilizing the transoral approach, scarring is completely absent and minimal dissection is required, decreasing post-operative complications. Furthermore, the dissection required for transoral robotic thyroidectomy progresses in the cranio-to-caudal direction. In contrast to conventional, trans-axillary, or bilateral axillo-breast approaches, the transoral approach allows identification of the RLN with IONM in proximity of the Berry ligament regardless of nerve direction. As this location occurs more superior relative to other approaches, transoral access provides a significant advantage for identifying the NRLN without iatrogenic injury.
To the best of our knowledge, this investigation is the first to report the use of transoral robotic thyroidectomy with IONM in a patient with NRLN. Further, we propose that transoral robotic thyroidectomy with IONM may potentially reduce adverse complications for patients presenting with NRLN as identified by preoperative imaging.
 XML Download
XML Download