

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Minimally invasive follicular thyroid carcinoma (MIFTC) patients usually have an excellent prognosis, but may present with a distant metastasis at the initial diagnosis or during the follow-up period. Therefore, the most important issue in MIFTC patients diagnosed after hemithyroidectomy is whether to perform further treatments, including completion thyroidectomy and/or radioactive iodine (RAI) remnant ablation and to identify which patients can obtain prognostic benefits by receiving these additional treatments. The decision for further treatments should be based on the risk factors for distant metastasis or prognostic factors affecting the distant metastasis-free survival (DMFS) or cause-specific survival (CSS) rates.
On the basis of previously published studies, age ≥45 years, primary tumor size ≥4 cm, vascular invasion itself, extensive vascular invasion with ≥4 foci, lymph node metastasis, and distant metastasis at the initial diagnosis have been shown to have a prognostic impact in MIFTC patients. Therefore, these risk factors have been widely used as criteria for recommending further treatments to patients with MIFTC after diagnostic hemithyroidectomy.
Our hypothesis was that patients with multiple risk factors for distant metastasis would have a poorer prognosis compared to patients without risk factors, because the relative risk would be increased proportionately based on the increasing number of involved risk factors. We also hypothesized that each risk factor and combinations of risk factors might influence development of distant metastasis differently. The aims of our present analyses were to analyze the risk factors for distant metastasis. And we compared the DMFS rates between the groups based on the number of involved risk factors, and eventually stratified the risk groups with regard to DMFS rates.
METHODS
1. Study population
Patients who underwent an initial surgery at the Asan Medical Center and were eventually diagnosed with MIFTC were identified. The medical records of these patients were retrospectively reviewed, and their clinicopathological characteristics and outcome data were recorded. Written informed consent for the clinical records to be used in this study was not obtained from the participants. Instead, patient identifiers were removed from all samples, and all data were de-identified prior to the analysis by a researcher who did not participate in this study. Distant metastasis included both synchronous and metachronous distant metastasis. Synchronous distant metastasis was defined as a metastasis detected at the time of the initial diagnosis or within 12 months after the initial operation.
After evaluating the selected risk factors for distant metastasis, patients were divided based on the number of risk factors: group 0 with no risk factors, group 1 with any one risk factor, group 2 with any 2 risk factors, and group 3 with all risk factors. Groups 1–3 were also subdivided into several subgroups based on the kind of involved risk factors. The relative risk for distant metastasis in each subgroup was estimated respective to the reference risk in the group without any risk factors. Moreover, DMFS rates between the aforementioned 4 groups were compared. Finally, risk groups were stratified with respect to DMFS rates.
2. Surgical strategy
Diagnostic hemithyroidectomy is the standard initial surgical procedure used at our institution to treat patients diagnosed with a follicular neoplasm by preoperative fine needle aspiration cytology. When a patient has another concomitant thyroid disease (i.e., Graves' disease or a nodular goiter of the opposite lobe), a total thyroidectomy is performed as the primary surgery. Central compartment node dissection is not routinely performed. However, ipsilateral or bilateral central compartment node dissection is performed if there are enlarged or suspicious lymph nodes. Completion thyroidectomy for MIFTC diagnosed after hemithyroidectomy is usually recommended for patients, especially when they had large primary tumor size (≥4.0 cm) or vascular invasion. Patients who refused completion thyroidectomy were provided sufficient information about the potential risks and received follow-up without further treatments.
3. Postoperative follow-up protocol
All patients received follow-up examinations in the outpatient clinic at our institution. Patients were checked at 1, 6, and 12 months, and annually thereafter while receiving thyroid hormone treatment in order to decrease their serum thyroid-stimulating hormone (TSH) levels to subnormal levels without thyrotoxicosis. Thyroid function tests, including serum TSH, thyroglobulin (Tg), and anti-Tg antibody level, were routinely performed at every hospital visit, and neck ultrasonography and chest computed tomography (CT) scans were routinely performed once per year. Postoperative RAI remnant ablation was performed at 4–6 weeks after completion thyroidectomy or total thyroidectomy. Diagnostic whole body scan following thyroid hormone withdrawal or thyrogen administration was performed 6–12 months after remnant ablation with the simultaneous measurement of serum Tg.
Distant metastasis was diagnosed using whole body scan, chest CT, or 18F-deoxyglucose positron emission tomography/CT and confirmed by serial imaging or biopsy. We defined recurrence as the reappearance of pathologically proven malignant tissue and/or the appearance of structural lesions on imaging studies, regardless of the serum Tg levels. Biochemical recurrence with elevated serum Tg level but without clinical evidence of structural disease at 6 months after the initial operation was not classified as true recurrence.
4. Statistics
Categorical variables are presented as numbers and percentages, and continuous variables as means±standard deviations. The risk factors for a distant metastasis were evaluated using univariate and multivariate Cox proportional hazard models, and the results are presented as hazard ratio (HR) with 95% confidence interval (CI). Multivariate analysis was performed after adjusting for all variables. To improve their clinical utility, continuous variables were converted into categorical variables on the basis of cut-off values, which were calculated using receiver operating characteristic (ROC) curve analysis. DMFS rates were calculated using the Kaplan-Meier method. Differences between the groups were analyzed for statistical significance using the log-rank test. All P values were 2-sided. Data were considered statistically significant if P<0.05. All statistical analyses were performed using SPSS (version 23.0; IBM Corp., Armonk, NY, USA).
RESULTS
Between February 1996 and December 2007, 259 patients underwent an initial surgery at the Asan Medical Center and were diagnosed with MIFTC. Hematoxylin and eosin-stained sections were reviewed by an experienced endocrine pathologist (DE Song) according to the World Health Organization (WHO) classification system for the pathological diagnosis and classification of follicular thyroid carcinoma (FTC) (1). After the pathological review, 195 patients were confirmed as having MIFTC and finally enrolled in this study.
The clinicopathological characteristics of these patients are summarized in Table 1. The median follow-up period was 99.5 months (range, 13–244). Fifteen patients (15/195, 7.7%) had distant metastasis. Of these patients, 7 patients already had distant metastasis at the time of diagnosis of their MIFTC, while 8 patients developed distant metastasis during the follow-up period.
Table 1
Univariate and multivariate risk factor analysis for distant metastasis in the patients with minimally invasive follicular thyroid carcinoma

1. Risk factor analysis for distant metastasis
Age, gender, surgical extent, primary tumor size, and extensive vascular invasion with ≥4 foci were potentially significant factors for distant metastasis by univariate analysis (Table 1). Age ≥45 years (HR=5.95; 95% CI=1.44–24.55; P=0.014), primary tumor size >4.0 cm (HR=4.79; 95% CI=1.18–19.33; P=0.028), and extensive vascular invasion (HR=19.63; 95% CI=5.18–74.39; P<0.001) were identified as independent risk factors by multivariate analysis. However, surgical extent and RAI ablation were not risk factors for prognosis in our study.
2. Relative risk for distant metastasis according to the number and composition of involved risk factors
The relative risk of each risk factor for distant metastasis, based on its number and composition, to the reference risk (=1) in the group without any risk factors is described in Fig. 1 and Table 2. These risk factors differently influenced the development of distant metastasis according to their number and composition. Extensive vascular invasion with ≥4 foci was the most powerful risk factor for distant metastasis, irrespective of the presence or absence of other risk factors. The HRs of all subgroups with extensive vascular invasion were much higher than the others which did not have extensive vascular invasion.
Fig. 1
Relative risk for distant metastasis according to the number and composition of involved risk factors.

Table 2
Relative risk for distant metastasis according to the number and composition of involved risk factors

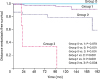
3. DMFS rates based on the number of involved risk factors and risk group stratification
As the number of involved risk factors increased, DMFS rates became significantly poorer (Fig. 2). Patients in groups 2 and 3 showed significantly worse DMFS rates compared to those of group 0 (P<0.001 for both) and group 1 (P<0.001 for both). The DMFS rates of group 3 were also significantly poorer than those of group 2 (P=0.004). Group 1 patients tended to have poorer DMFS rates compared to those of group 0 patients, but this difference was not significant (P=0.078). Therefore, these enrolled patients can be stratified into 3 risk groups with respect to DMFS rates: a low-risk group with ≤1 risk factor, an intermediate-risk group with any 2 risk factors, and a high-risk group with all 3 independent risk factors for distant metastasis.
DISCUSSION
In our present study, older age (≥45 years), larger primary tumor size (>4.0 cm), and extensive vascular invasion (≥4 foci) were found to be independent risk factors for distant metastasis in MIFTC patients. Among these independent risk factors, extensive vascular invasion was the most powerful risk factor as both of a single risk factor and combined with other risk factors. As expected, the DMFS rates worsened as the number of involved risk factors increased. On the basis of these results, MIFTC patients can be stratified into 3 risk groups with regard to DMFS rates; low- (with one or no risk factors), intermediate- (with any 2 risk factors), and high-risk groups (with all 3 independent risk factors).
There was still controversy about performing further treatments in the patients with MIFTC after diagnostic hemithyroidectomy (2-7) and many previously published studies have demonstrated various kinds of risk factors for distant metastasis and their prognostic impacts on DMFS or CSS rates in MIFTC patients. These risk factors include age ≥45 years (2,6-11), primary tumor size ≥4 cm (2,8,10,12,13), vascular invasion itself (6,9,14), vascular invasion with ≥4 foci (8,15), and distant metastasis at the initial diagnosis (2,6,8,12). These results were mostly consistent with the results from this present study except for distant metastasis at the initial diagnosis. The reason why distant metastasis at the initial diagnosis was not an independent risk factor in our study might be due to our definition of distant metastasis including both synchronous and metachronous one.
Most previous studies simply recited risk factors associated with prognosis, but did not demonstrate the relative risk for distant metastasis or the different influence on prognosis of combined multiple risk factors. Moreover, these earlier studies had other limitations, including small sample sizes, heterogeneity of their patient cohort, and relatively short follow-up durations. Unlike previous reports, however, our present study focused on the prognostic impact of the number of involved risk factors. Our findings revealed that the larger number of involved risk factors was related to the higher risk for development of distant metastasis and the poorer DMFS rates. Moreover, DMFS rates in patients with any one risk factor did not show a significant increase in metastasis risk compared with those without risk factors.
To the best of our knowledge, our current study is the first to attempt to stratify risk groups in patients with MIFTC with regard to DMFS rates based on the number of involved risk factors. We thought that our result may contribute to suggest a guideline of further treatments in MIFTC patients. Therefore, the decision of whether to perform further treatments for the patients with MIFTC after diagnostic hemithyroidectomy should be made carefully according to not only the risk factors themselves but also those number and composition.
In a similar manner to previous studies on MIFTC, our study shares the limitations of retrospective studies, which may be affected by various confounding selection biases. And small number of patients' cohort made difficult to accept our result entirely. Patients who had one risk factor with extensive vascular invasion in group 1 were only 3 cases, and none of them developed distant metastasis. This might be why high relative risk of extensive vascular invasion could not be reflected in group 1 survival rate. Therefore, our findings should be re-evaluated using a larger number of patients and a longer follow-up period.
CONCLUSION
On the basis of our findings, MIFTC patients can be stratified into 3 risk groups based on the number of involved risk factors: a low-risk group with any one or no risk factors, an intermediate-risk group with any 2 risk factors, and a high-risk group with all 3 independent risk factors for distant metastasis. MIFTC patients involved in an intermediate- or high-risk group should be considered to perform further treatments, whereas MIFTC patients with no or only one distant metastasis-related risk factor (even with only extensive vascular invasion) may be followed under close observation without additional treatments.
 XML Download
XML Download