

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease is one of the main causes of morbidity and mortality in patients with chronic kidney disease (CKD) and end-stage renal disease (ESRD). Prior studies have observed the subclinical damage to large arteries and have demonstrated that both structural and functional alterations of these large arteries are major contributing factors related to cardiovascular complications.1)2)
Notably, arterial stiffening and remodeling in patients with ESRD are of multifactorial origin, with extensive arterial calcifications, and have been shown to be a strong and independent predictor for both all-cause and cardiovascular deaths.2)3)4) It has been also observed that arterial stiffening occurs prior to the development of structural changes of the arterial wall.5) Thus, arterial stiffness has emerged as a reliable feature for the early detection of atherosclerotic vascular changes and also as a potential novel therapeutic target for cardiovascular risk reduction in patients with ESRD. Therefore, the accurate non-invasive assessment of arterial stiffness has developed a considerable clinical interest as there is no gold standard for evaluating arterial stiffness thus far.6)
A recently developed multi-directional carotid artery strain assessment method using speckle-tracking ultrasonography is one of the most accessible and reproducible non-invasive imaging modality that can directly and quantitatively assess arterial stiffness, compared to conventional aortic stiffness measures such as distensibility, elastic modulus, β stiffness index, or carotid femoral pulse wave velocity.6)7) The reliability and sensitivity of the speckle-tracking carotid strain imaging has been validated in both normal subjects and patients with hypertension and diabetes, but not in patients with ESRD so far.6)7)
In this regard, we aimed to explore the difference in the multidirectional movements of the common carotid artery (CCA) as assessed by the speckle-tracking carotid strain imaging method between patients with ESRD and those with normal kidney function.
METHODS
Study population
From April 2014 to May 2015, 121 patients who underwent carotid ultrasonography for the evaluation of atherosclerosis status were enrolled in this single-center study. Patients were divided into the following groups according to their renal function and history of dialysis: normal renal function, defined as estimated glomerular filtration rate (eGFR) > 90 mL/min/1.73m2, group (control) and the ESRD group according to the guidelines of the Kidney Disease: Improving Global Outcomes (KDIGO).8) Patients with eGFR ≤ 90 mL/min/1.73m2 but not undergoing dialysis, patients with significant CCA stenosis (>50%), and patients with CCA stent or prior history of CCA surgery were excluded. The study design was approved by the institution's human research committee, and the study protocol conformed to the ethical guideline of the 1975 Declaration of Helsinki and informed consent was provided by the patients to participate in the study. Clinical characteristics and laboratory results at the time of carotid ultrasound were collected.
Carotid ultrasound image acquisition
High-resolution carotid ultrasound images were acquired using a linear array transducer (nominal bandwidth of 3–12 MHz) with an 8-MHz center frequency (RS80A and HS70A, Samsung Medison, Seoul, Korea). To acquire a high frame rate (>120 fps), the view angle was reduced to ensure accurate measurements of CCA movements. Patients' heads were tilted slightly upward to the midline position, and both CCAs were examined using recordings at ≥2 consecutive beats.
Assessment of the multidirectional movements of the CCA
The images showing the multidirectional movements of the CCA were analyzed using commercially available software (Samsung Medison Co., Ltd., Seoul, Korea). The software assesses the functional property of CCAs by automatically calculating the displacement of the CCA walls (Figure 1).
Figure 1
Strain analysis of the common carotid artery using the speckle tracking method for carotid B-mode ultrasonography in a 69-year-old normal control patient (A) and an age-matched ESRD patient (B). The strain and strain rate values were all decreased in the end-stage renal disease patient compared to the normal control patient.

For the analysis, ≥5 mm of the CCA below the origin of the carotid bulb was selected. The user-defined control points, the blood-intima boundaries of the CCA, were manually traced from a still frame image with the best image quality and were automatically tracked by the software based on an optical flow algorithm.9) The control points are constrained to maintain the global shape and to move within a local range, to ensure stability in tracking the motion of vessels. At least four speckles on the CCA wall were identified, and the movements of each speckle during the cardiac cycle were traced at the near and far walls. Radial movement of the CCA in the longitudinal plane and radial circumferential movements in the transverse plane were automatically calculated using the speckle-tracking technique. Peak radial and circumferential displacements, strain, and strain rate were also calculated.
For the calculation of conventional arterial stiffness parameters,10) the central blood pressure, derived from the aortic pulse wave, was measured after ≥5 min of resting in supine position by a trained technician with pulse wave analysis of the radial artery using a tonometry (SphygmoCor; AtCorMedical, Sydney, Australia). The SphygmoCor software calculated the aortic pulse wave by means of a generalized transfer function from the radial signal. The measured central blood pressure was entered into the software, and all arterial stiffness parameters were then automatically calculated from the software according to the pre-defined formula for each parameter. β stiffness index was defined as the ratio of the natural logarithm of central systolic/diastolic pressure to relative change in diameter. Arterial compliance was defined as the absolute change in CCA diameter for a given change in pressure (e.g., difference between the diastolic and systolic diameters [ΔD]/difference between the systolic and diastolic blood pressures [ΔP]). Distensibility refers to the relative change in vessel diameter for a given change in pressure (e.g., ΔD/[ΔP × CCA diameter in the diastolic phase (D)] in mmHg). The elastic modulus index was defined as the pressure change required for the theoretical stretch from the resting vessel diameter (e.g., [ΔP × D]/ΔD in mmHg). (e.g., log [systolic blood pressure/diastolic blood pressure]/[ΔD/D]). Pulse wave velocity β (PWV) was defined as the speed with which the pulse wave travels along the length of the artery (e.g., stiffness index × diastolic blood pressure/[2 × blood density]), while assuming the blood density to be 1.050 g/cm3.
The presence of carotid plaque was defined as a focal structure that protrudes into the arterial lumen and measured ≥1.5 mm or ≥50% of the surrounding intima-media thickness (IMT). Additional images were acquired at another location close to the CCA that does not contain the plaque for patients with carotid plaques for the analysis. Carotid IMT was measured in a semiautomatic manner in the end-diastole phase for bilateral CCAs in the longitudinal plane, and the mean value of the right and left IMTs was used in the analysis. In patients with carotid plaque, IMT was measured at a location where the plaque was not included.
Statistical analysis
Parametric continuous variables were presented as mean ± standard deviation, and categorical variables were expressed as count (%). Differences between continuous variables were compared using Student's t-test or Mann Whitney U test, as appropriate, whereas the Pearson's chi-squared or Fisher's exact test was employed, as appropriate, for categorical variables. To assess the impact of ESRD on the carotid strain values and conventional aortic stiffness parameters, multivariate linear regression analyses were constructed and adjusted for age, male sex, hypertension, diabetes mellitus, body mass index, creatinine level, high-density lipoprotein level, the presence of carotid plaque, and the maximal diameter of CCA. A two-tailed p-value <0.05 was considered statistically significant. All analyses were performed using SPSS (Version 23.0, IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics of the study population
A total of 85 control patients (61 ± 12 years old, 53% were male) and 36 with ESRD (55 ± 3 years old, 61% were male) were enrolled (Table 1). There was no difference in the percentage of male sex (p = 0.431), but patients with ESRD were younger and had more hypertension than control patients (89% vs. 47%, p < .001). Central systolic and diastolic blood pressures were also higher in the ESRD group (all p < 0.05), but there were no differences in body mass index and the presence of diabetes mellitus or hyperlipidemia (all p > 0.05). The level of total cholesterol was higher in the ESRD group (180.8 ± 40.5 mg/dL vs. 160.8 ± 40.0 mg/dL, p = 0.016), but there were no differences in the level of high-density lipoprotein, low-density lipoprotein, and triglyceride (all p > 0.05).
Table 1
Baseline characteristics and laboratory results of the controls and patients with ESRD

Carotid ultrasonographic findings
Carotid ultrasonography and subsequent strain analysis were successfully performed on all participating patients. Atherosclerotic carotid plaques were detected in 82.4% of the controls and 31.4% of patients with ESRD (p = 0.002) (Table 2). The mean maximal diameter of CCAs in the longitudinal plane were greater in patients with ESRD than in the controls (7.54 ± 1.32 mm vs. 6.54 ± 0.91 mm, p < .001), but the IMT was not different (0.76 ± 0.15 mm vs. 0.81 ± 0.17 mm, p = 0.121). There were no differences in the β stiffness index and arterial compliance (all p > 0.05) between groups, but the arterial distensibility was lower and the elastic modulus and PWV were higher in the ESRD group (all p < 0.05). When the strain parameters were compared, the radial strain rate in patients with ESRD was significantly lower than that in the controls (0.711 ± 0.298 /s vs. 1.005 ± 0.508 /s, p = 0.001), although there were no differences in displacement and strain.
Table 2
Comparison of ultrasonographic parameters in the longitudinal plane between the controls and patients with ESRD

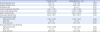
The results of the assessment of the transverse plane were also consistent (Table 3). The minimal and maximal CCA diameters were greater in patients with ESRD (all p < 0.05). β stiffness index and arterial compliance were not different, but the patients with ESRD exhibited lower arterial distensibility and higher elastic modulus and PWV compared with the controls (all p < 0.05). The speckle-tracking carotid strain analysis revealed that while there were no differences in displacement and strain between both the radial and circumferential methods, both radial and circumferential strain rates were significantly reduced in patients with ESRD (0.72 ± 0.47 /s vs. 0.97 ± 0.45 /s and 0.74 ± 0.54 /s vs. 0.99 ± 0.47 /s, all p < .001).
Table 3
Comparison of ultrasonographic parameters in the transverse plane between the controls and patients with ESRD
Impact of ESRD on strain parameters
In the multivariate linear regression analyses adjusted for age, male sex, hypertension, diabetes mellitus, body mass index, creatinine level, high-density lipoprotein level, the presence of carotid plaque, and the maximal diameter of CCA, ESRD had no impact on both conventional aortic stiffness parameters, including distensibility, elastic modulus, and PWV, and strain parameters assessed in the longitudinal plane (all p > 0.05) (Table 4). ESRD also had no impact on distensibility, elastic modulus, and PWV assessed in the transverse plane (all p > 0.05).
Table 4
Multivariate linear regression analysis for the impact of ESRD on aortic stiffness and strain parameters*
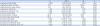
In contrast, ESRD was negatively and independently associated with both transverse radial strain and strain rate (β: -6.087 (95% confidence interval [CI]: -10.790 to -1.384) and β: -0.833 (95% CI: -1.390 to -0.275), respectively, all p < 0.05). ESRD also independently reduced the transverse circumferential strain and strain rate (β: -6.771 (95% CI: -11.525 to -2.018) and β: -0.976 (95% CI: -1.582 to -0.371), respectively, all p < 0.05). There was no correlation between male sex and strain values in all models.
DISCUSSION
In the present study, speckle-tracking strain ultrasonography of the CCA was successfully performed in both normal subjects and patients with ESRD. When compared with patients with normal renal function, the CCA diameter was greater and the overall conventional aortic stiffness indices and strain parameters were reduced in patients with ESRD. In multivariate analyses, ESRD independently reduced both radial and circumferential strain parameters assessed on the transverse plane, while not exhibiting an impact on the longitudinal strain values and conventional aortic stiffness parameters.
Arterial remodeling in patients with ESRD is characterized by increased arterial diameters, outward remodeling, and arterial stiffening.11)12) These arterial remodeling also affects the arterial wall viscoelastic properties.11) The alterations of the intrinsic elastic properties of arterial walls, caused by fibroelastic intimal thickening, calcification of vessel walls, inflammation, and increase in collagen, promote the hardening and stiffening of arteries in patients with ESRD.2)3) This changes in arterial viscoelastic properties have shown to be associated with the development of left ventricular hypertrophy and congestive heart failure.11) In hemodialyzed patients, arterial stiffening was associated with calcification of the arteries and worsened as calcification increased.13)14) Recent studies have also emphasized the role of arterial stiffness as an independent cardiovascular risk factor in various disease populations.2) In this regard, various indices that either directly or indirectly measure aortic stiffness have been developed and validated.
Conventional indices for aortic stiffness require the measurement of the central blood pressure and certain assumptions to be calculated. PWV, the most widely adopted technique for the assessment of aortic stiffness so far, assesses the propagation velocity of the pressure wave from the proximal aorta toward the peripheral vessels. PWV can be measured on any arteries, but only the carotid to femoral PWV has been proven to have a predictive value for clinical outcomes.15) PWV assesses the stiffness of an artery as a hollow structure, and is dependent on the artery geometry, the intrinsic properties of the arterial wall biomaterials, and blood density, which is difficult to measure in clinical setting and has to be assumed.
The speckle-tracking carotid strain ultrasonography enables the direct measurement of arterial dimension changes during the cardiac cycle. This straightforward method can provide the stress-strain relationship and does not requires the value of central blood pressure or any assumptions for the calculation, hence can be yielded at any given blood pressure level. Our group recently has shown the feasibility and value of carotid strain analysis in patients with stroke.16) In the current study, the analysis of carotid strain was also easily and successfully completed in patients with ESRD.
ESRD is characterized by a high prevalence of cardiovascular risk factors, such as hypertension, diabetes mellitus, dyslipidemia, inflammation, and metabolic disturbances.17) Exposure of arteries to these environments might induce arterial remodeling and stiffening. Previous studies emphasized the role of arterial stiffness in the development of cardiovascular diseases, and the parallel increases of the risk of cardiovascular disease and aortic stiffness along with the deterioration of CKD have already been observed.18)19) In this, only circumferential wall stress was independently associated and occurred in parallel with the deterioration of CKD.18) The aortic stiffness was greater in CKD patients even after age and blood pressure were adjusted for, when compared with healthy subjects and hypertensive patients.13)18)
In the current study, while the CCA diameter was greater in patients with ESRD, there were no significant differences in IMT, β stiffness index, and arterial compliance. This observation is in line with a recent study reporting that carotid IMT declined during the worsening of CKD.18) Although arterial distensibility, elastic modulus, and PWV, among conventional aortic stiff indices, showed a significant difference between the patients with normal renal function and patients with ESRD, these parameters also have failed to demonstrate an independent association with ESRD in the multivariate analyses. In contrast, ESRD independently reduced both transverse radial and circumferential strain and strain rate. These results suggest that the carotid strain analysis in the transverse plane, which can be easily and readily be performed, might be a better parameter for the evaluation of aortic stiffness that has an independent relationship with ESRD.
This study had several limitations. First, due to the study's cross-sectional design, the prognostic value of the carotid strain parameters on clinical outcomes could not be evaluated. Second, because only patients with ESRD were enrolled, the feasibility and validity of the strain values in patients with CKD were not assessed. However, given the fact that strain values were the only parameters that were independently associated with ESRD in this study, prospective studies enrolling patients with both CKD and ESRD to determine the relationship between CKD deterioration and carotid strain, and the predictive value of strain analyses, now seem warranted.
In conclusion, we have demonstrated the feasibility of carotid strain analyses in patients with ESRD and its value in the assessment of aortic stiffness. ESRD had an independent and negative relationship only with transverse radial and circumferential strain and strain rate, but not with the conventional aortic stiffness indices. Multidirectional carotid strain analyses in patients with ESRD have the potential to provide useful information for risk stratification.
 XML Download
XML Download