

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Abdominal bloating is a subjective sensation characterized by increased pressure in the abdomen,1 but may not necessarily be associated with an objective measurement of increased girth. The symptom is very common in patients with irritable bowel syndrome (IBS) or other functional gastrointestinal disorders (FGIDs), as well as those with organic disorders.2 It is the second most common symptom following abdominal pain for those with IBS.3 Despite its prevalence, the pathophysiology still remains elusive, and effective therapeutic options are limited. The production of intestinal gas and transit, as well as hypersensitivity of the gut might cause symptom onset. Recently, the role of gut microbiota in IBS symptoms, including bloating, has been suggested,456 and researchers have found the altered colonic flora in stool samples of IBS patients.78 Patients with bloating also have also been shown to have increased gas production from bacterial fermentation caused by small intestinal bacterial overgrowth.9
Rifaximin is a gut-selective antibiotic with little systemic absorption and broad-spectrum activity against gram-positive and gram-negative aerobes and anaerobes.10 The antibiotic has been increasingly used to treat IBS symptoms based on the notion that altered gastrointestinal flora or small intestinal bacterial overgrowth might cause distension symptom.11 However, due to the lack of large-scale cohort study, the indication, dosage, or treatment duration for rifaximin remains unclear.2 The aim of this retrospective study was to evaluate the final diagnosis profile of patients without organic disease treated with rifaximin for abdominal bloating, as well as to evaluate its response rate.
SUBJECTS AND METHODS
1. Patients
We retrospectively reviewed the medical charts of patients who visited Seoul National University Bundang Hospital between September 2007 and July 2013 for abdominal bloating. After finding no improvement from using common medication, such as probiotics, prokinetics, or antispasmodics, rifaximin (Normix®, Alfa Wassermann, Bologna, Italy) was prescribed. Patients who were found to have organic gastrointestinal disorder were excluded (Fig. 1). This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital, Korea (IRB No. B-1801/445-108).
2. Chart review
The clinical manifestations and final diagnosis according to the Rome III criteria were reviewed. Patients were classified as having irritable bowel syndrome (IBS), functional dyspepsia, or combined FGID. Those who did not meet the criteria for aforementioned diagnoses were diagnosed as functional bloating.
Medication record was searched for rifaximin treatment for abdominal bloating. The response rate to rifaximin treatment was determined by examining the follow-up medical record. The self-reported severity score, as described for abdominal distension/tightness, was used to evaluate the effectiveness. The severity scoring questionnaire is described elsewhere.12 Response to treatment was defined as having more than 50% improvement in the subjective score, four weeks after the cessation of treatment. The change in symptom after adding rifaximin to each patient's regimen was specifically recorded.
3. Abdominal simple X-ray
Those with bloating at the time of visitation to the clinic underwent abdominal X-ray. Examinations for interpretation were randomly assigned to three radiologists who were blinded to clinical information. The formal report of radiologist was obtained, and remarks, such as ‘gas distension’, ‘feces retention’, or ‘mild ileus’, were defined as having remarkable X-ray findings.
RESULTS
1. Baseline demographics
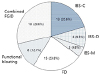
Sixty-three patients without organic diseases were enrolled. The average age was 56.8±14.2 years. Among them, 76.1% of the patients were older than 50 years (Table 1). Thirty-one out of the total 63 patients were female (49.2%). Among the 26 patients with the available records of abdominal X-ray, 10 had gas distension or feces retention with mild ileus, as documented by a radiologist. The average duration of bloating symptom before the prescription of rifaximin was 24.0 months (Table 1). According to the Rome III criteria, there were 22 patients (34.9%) with IBS, 15 (23.8%) with functional dyspepsia, and 18 (28.6%) with combined FGID. Patients who failed to meet the criteria for IBS or functional dyspepsia were classified as having functional bloating (12.7%) (Fig. 2).
2. X-ray findings
Out of the 26 patients with X-ray records, 10 patients (38.5%) showed remarkable X-ray findings, such as gaseous distension or feces retention with mild ileus (Table 2). Irritable bowel syndrome with constipation (IBS-C) group showed relatively high proportion of remarkable X-ray finding (5 out of 8 patients, 62.5%); however, the difference between the IBS-C group and others was not statistically significant (p=0.099, compared to other groups).
3. Response rate according to diagnosis
Excluding the 12 patients who were lost to follow-up, a total of 51 patients were analyzed. Twenty-six (51.0%) patients experienced an improvement of abdominal bloating after rifaximin treatment. Among them, 12 (46.1%) had 50% improvement, nine (34.6%) had 75% improvement, and five (19.2%) reported full recovery. The degree of response was not significantly different according to diagnosis (p=0.334).
In the IBS-C group, the response rate was relatively low (41.7%) compared with the other diagnostic groups (50–54.5%); however, the difference was not statistically significant (p=0.460) (Table 2).
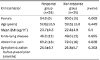
The proportion of females was higher in the non-response group than in the response group; however, without statistical significance (60.0% vs. 34.6%, p=0.069). Otherwise, there was no statistical difference between the response and non-response groups (p>0.05) (Table 3).
4. Response rate according to rifaximin dosage
With a dosage of 800 mg or 1,200 mg, rifaximin was used from 5 to 14 days, respectively. The most frequently prescribed regimen was rifaximin 1,200 mg for seven days (total dose of 8,400 mg, 19 patients, 37.2% of total). The response rate varied from 20–66.7%, according to different regimens. Ten-day regimens with 800 mg or 1,200 mg showed a relatively high response rate (62.5% and 66.7%, respectively). The lowest response rate was noted with 800 mg for 14 days (total 11,200 mg, 20%) and 1,200 mg for 14 days (total 16,800 mg, 25%). However, no statistical significance was noted between the groups (p=0.537) (Table 4). The degree of improvement was not significant between the groups (p=0.841).
DISCUSSION
Abdominal bloating is a widely prevalent and bothersome symptom in patients of all ages. Patients experience gaseous distension, not only in those with organic diseases but also in those with IBS and other FGIDs. It is a common complaint worldwide, with the prevalence of over 15% both in Asia and USA.131415 There have been many studies trying to explain the pathophysiology and to provide treatment; however, the exact pathophysiology of bloating remains unclear.23 The relationship between bloating and actual abdominal distension was also investigated; however, only half of patients with bloating had demonstrable increase in girth.16 Among many other possible etiologies, such as psychologic tendency, altered gut motility, visceral hypersensitivity, and malabsorption, the impact of gut microbiome has been studied extensively.456717
Based on studies showing a relationship between gut microbiota and bloating, rifaximin - a non-absorbable antibiotic - has been proposed as a possible therapy for treating bloating due to gut microbiota.1819 This antibiotic has been suggested to reduce the amount of abdominal gas by decreasing abnormal bacterial fermentation.20 Rifaximin was also reported to have an eradication rate for bacterial overgrowth as high as 70%.21
There have been several clinical reports with various dosage and treatment duration.222324 However, there is no widely accepted guideline or recommendation for the use of rifaximin for bloating, as reflected by the Japanese health insurance system not covering antibiotics to be used for the purpose.25
In the current study, the mean age of enrolled patients was 56.8 years. Patients older than 50 years constituted 76.1% of the study population. Compared with a previous randomized clinical trial on rifaximin therapy, which was published in 2011, showing a mean age of 46.2 years,22 our study had a population with relatively high mean age. A meta-analysis that reported the global prevalence of IBS revealed a trend that older patients have lower pooled prevalence, while those under the age of 30 years and between 30 and 39 have the highest prevalence (11.0; 95% CI, 6.0–18.0 and 7.0–16.0, respectively).26 In a meta-analysis focus on the efficacy and safety of rifaximin for IBS, age was a significant factor associated with the improvement of global IBS symptoms (correlation coefficient, 0.97).27 The study reported that older patients had higher rates of improvement.27 The response rate to rifaximin was 51.0% in our study. In the meta-analysis, the pooled odds ratio for the improvement of bloating was 41.6 compared with 31.7 in the placebo group.27 The higher rate of improvement in our study could partly be attributed to the enrollment of patients with relatively high age. This necessitates further large-scale study to confirm our findings.
Although plain abdominal film is a simple and noninvasive method to identify intraluminal gas,28 to the best of our knowledge, there is no specific guideline for conventional radiography in FGID according to systemic review articles.2930 In contrast to the cases of acute abdominal pain,31 there is no widely accepted relevant radiologic findings for FGID. There have been efforts to objectively describe the amount of abdominal gas in FGID patients using simple X-ray; however, they reported mixed results. One of the studies measured gas bubble to be more than 1 cm in diameter to quantify bowel gas area (BGA).32 It reported higher BGA in the constipation-predominant IBS and unspecified functional bowel disorder patients than the control group (p<0.01); but, BGA did not correlate with symptoms.32 Another study employed a gas volume score (GVS) by calculating the pixel value on images and found significantly higher GVS of IBS patients than the control group (p<0.001).33 However, a research on subjective symptom and GVS failed to report a significant correlation between them.34 Another study using GVS also found no difference between IBS patients and the control group.35 There was no significant relationship between GVS and organic acid or bacterial counts as well.35
As there is no universally accepted plain X-ray finding for FGID, we defined ‘remarkable’ film as ‘gaseous distension’ or ‘feces retention with mild ileus’. We found specific X-ray reports in 38.5% of patients with bloating. Among them, IBS-C patients showed the highest proportion of patients with abnormal X-ray. Although the number of cases is small, this is a similar finding to the previous report with IBS-C patients.32 A future large-cale study with IBS-C patients could be helpful to prove the utility of plain film in the population. Our result of X-ray may be limited in that not every patient underwent X-ray because it was performed only for those with symptoms, such as abdominal distension at the time of visit. It could be meaningful if the plain films were compared before and after the treatment to investigate the effects of treatment on the image and correlated it with the symptom.
Our study was designed to investigate the effect of rifaximin in clinical practice, according to various dosages and treatment durations with different diagnoses. Patients with bloating were finally diagnosed as IBS 34.9% (IBS-C 20.6%, IBS with diarrhea 9.5%, mixed type IBS 4.8%), functional dyspepsia 23.8%, functional bloating 12.7%, and combined FGID 28.6%, based on the Rome III criteria. It shows that many functional disorders present bloating as a symptom, although the response to rifaximin did not show a significant difference between the diagnoses.
There have been several clinical studies that included randomized trials. Sharara et al.19 reported the significant difference in global symptom relief in IBS patients treated with rifaximin compared with placebo (41.3% vs. 22.9%, p=0.03); however, they did not classify IBS into subgroups for analysis. A randomized trial by Pimentel et al.18 also reported greater improvement in IBS symptoms in rifaximin group than the placebo group (36.4% vs. 21.0%, p=0.020). They found a significantly better bloating severity score (p=0.010).18 However, they also did not report the analysis for IBS subgroups.18 According to a previously conducted randomized study that exclude IBS-C, the response rate for bloating symptom was 39.5% and 41.0%, compared with that of placebo (28.7% and 31.9%, respectively).22 Another retrospective study for non-constipated IBS subjects reported that as high as 75% of patients had clinical improvement.36 A phase 3 study for relapsing IBS-D patients also reported the efficacy and safety of repeat rifaximin treatment.37
In our study, 51.0% of the entire patient population showed clinical improvement. For IBS-C patients, 41.7% of them responded. When the response rate was calculated, excluding IBS-C, it was 53.8% (21 out of 39). The current study shows a relatively high effectiveness of the treatment, especially for non-IBS-C patients. As clinical reports on the effect of rifaximin with various subtypes of IBS are scarce, our report could provide meaningful information.
The mechanism of rifaximin in FGID is complex. Its direct effect on bacteria and virulence factors, as well as indirect effects like reduction of mucosal inflammation, had been documented.38 There was a molecular approach to explain the effect of rifaximin for non-constipated IBS patients based on gut microbiota modulation.39 Rifaximin treatment relieved IBS symptom; however, it did not show any shifts in the overall composition of microbiota.39 It implied other mechanisms of action by rifaximin, as suggested by an animal study, such as prevention of gut inflammation and visceral hyperalgesia,40 might have contributed to the clinical improvement. A study with subjects without small intestinal bacterial overgrowth confirmed by negative lactulose breath test reporting the relief of belching and bloating symptoms41 could further support the complex mechanism of rifaximin other than its effect on intestinal microbiota.
The response rate varied according to the dosage and duration of the treatment. Ten-day regimens with 800 mg or 1,200 mg showed a relatively high response rate. The lowest response rate was noted with a regimen of 14 days. Although the sample size was small, this result could imply that the effect of rifaximin varies according to the treatment duration.
Our study has many limitations. It was conducted as a single-center, retrospective study with a relatively small sample size. The reason of this small size mainly originated from the preliminary trial to evaluate the efficacy of rifaximin, which was not officially proved for bloating symptom of FGID. Nowadays, as there is great deal of accumulated data, a large-scale prospective cohort study with different regimens in Korea may help establish recommended dosage and duration of antibiotic treatment for bloating symptom. The limitation of this retrospective study not having a control group and lack of randomization should also be noted. The possible confounding factors and the placebo effect, which is especially prominent in FGID patients, also need be considered in the interpretation of our results. In conclusion, we report the response rate of rifaximin for various FGIDs in clinical practice.




 XML Download
XML Download