

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ventricular septal defect (VSD) is the most common congenital heart defect.1)2) Surgical closure of VSD has been performed for many years with minimal mortality and is considered the gold standard for treatment. However, open heart surgery has significant morbidity and potential problems in the long term, including skin problems associated with the wound.3) Accordingly, catheter device closure of VSD has become an attractive alternative to surgery. Transcatheter closure of VSD is performed in the early period with various types of devices such as the Rashkind double umbrella device,4) CardioSEAL device (NMT Medical, Boston, MA, USA), and STARFlex device (NMT Medical, Boston, MA, USA).5) Transcatheter closure of muscular VSD has been accepted as a safe and acceptable alternative to surgery, especially in small children.6)7) In the recent past, the Amplatzer device (St. Jude Medical Corp, St. Paul, MN, USA), designed for closure of perimembranous VSD, was developed, but was associated with a high rate of post-procedural or late onset complete atrioventricular block (CAVB) that necessitated permanent pacemaker insertion.8)9)10) As a result, there are important modifications for the prevention of CAVB, and various positive clinical experiences have since been reported with those devices.11)12) In Korea, there was a report about transcatheter closure of perimembranous VSD with an Amplatzer duct occluder I,1) but it was an off-label use of the device. Recently, various types of Cocoon occluders (Vascular Innovations Co., Nonthaburi, Thailand) for VSD were developed. Cocoon devices for VSD are known to be softer than the Amplatzer device and superior in prevention of CAVB. Cocoon devices, including VSD occluders, are now available in South Korea; therefore, we reported our early experiences of transcatheter closure of VSD using Cocoon devices.
METHODS
Thirteen patients who underwent transcatheter VSD closure with Cocoon devices at Samsung Medical Center were enrolled retrospectively (Table 1). There were 7 males and 6 females. The median age was 5.8 years, ranging from 7 months to 48 years, and the median weight was 20.3 kg (range 7–59.9 kg). Diagnosis and detailed evaluation of anatomical classification and size were performed with transthoracic echocardiography (TTE) before the procedure. All patients had a significant systolic murmur on chest auscultation and VSD on TTE. Evidence of significant volume overload such as clinical symptoms, cardiomegaly on chest radiography, or left ventricular dilatation on echocardiography was resolved prior to closure. Patients with elevated pulmonary artery pressure, aortic valve regurgitation associated with VSD, or a defect too large for the device were not candidates for transcatheter closure.
Table 1
Patients' data
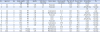
Data are expressed either as mean ± SD or as median (range). The institutional review board approved this study and waived the need for consent from patients or parents.
Characteristics of devices
The Cocoon VSD occluder is a percutaneous transcatheter VSD closure device intended for the occlusion of hemodynamically significant VSDs. It is a self-expandable, double disc device made from Nitinol wire mesh coated with platinum using nanofusion technology. The two discs are linked together by a connecting waist corresponding to the size of the VSDs. In order to increase closing ability, the discs and the waist are filled with polypropylene fabric, securely sewn to the wires using polyester thread. Cocoon VSD occluders are available in three different designs to match the types and location of the VSDs to close: membranous type (Figure 1A), muscular type (Figure 1B), and aneurysmal type (Figure 1C). In this study, the Cocoon duct occluder (Figure 1D) for patent ductus arteriosus is also used in the transcatheter closure of VSD. It is made from Nitinol wires coated with platinum using nanofusion technology. The distance between the two discs is different among the three types of VSD occluders: 4 mm, 7 mm, and 10 mm. Both side discs are 6 mm or 6.5 mm larger than the waist, but the side waist diameters are different for the aneurysmal type. The Cocoon duct occluder has the same profile as the Amplatzer duct occluder.
Device implantation and follow-up
The procedure was performed under general anesthesia and guidance with transesophageal echocardiography (TEE). A bolus infusion of 100 U/kg heparin was used immediately after the femoral artery was accessed. The device type and size were selected based on TTE images and LV angiographic images. The largest among the various diameters was used for deciding device size. The device with a waist 1–2 mm larger than the VSD size was selected.
Similar procedures were applied for every kind of VSD closure. The VSD was crossed in a retrograde fashion from the aorta using a Terumo® guide wire that was snared at the pulmonary artery and withdrawn through the femoral venous sheath. After ensuring that the tricuspid chordae was not crossed, the catheter was advanced over the guide wire to the inferior vena cava. A long delivery sheath was passed over the guide wire from the femoral vein to the ascending aorta or left ventricle. The device screwed on the delivery cable was passed through the delivery sheath. The distal disc was opened in the aorta or left ventricle, and the whole system was withdrawn. The right ventricular disc was opened in the right ventricle after confirming that the left ventricular disc was in the correct position. After verifying the position of the device and the aortic and tricuspid valves by TEE and angiography, the device was released.
After device implantation, continuous intravenous heparin infusion was given for 24 hours. The patients were monitored with electrocardiography and chest radiography every day until discharge two days after the procedure. Aspirin as an antiplatelet agent was prescribed for 6 months. One week and every month after the procedure, routine chest radiography and 12-lead electrocardiography were carried out at an outpatient clinic. Follow-up TTE was performed at 3 months post procedure and then 6 months later.
RESULTS
A device was successfully implanted in all patients. The follow-up period was 10 ± 6 months, and no mortality was observed. There were no associated malformations in any patient. The results of all the patients are summarized in Table 1. Only one device was implanted for each VSD, except for one patient who received two devices for perimembranous VSD closure. In that case, a Cocoon VSD occluder of the aneurysm type was implanted first, but then replaced with an Amplatzer duct occluder II and Cocoon duct occluder due to multiple exits to the right ventricle with significant residual shunt. Devices were implanted for muscular VSD in 2 patients, postoperative residual VSD in 2 patients, and perimembranous VSD in 9 patients. Muscular type devices were used for 5 patients, membranous type for 3 patients, aneurysmal type for 3 patients, and a duct occluder for 2 patients. The mean fluoro time was 29.7 min (range 6.8–76.0 min). No patients experienced major procedural complications, but residual leaks and conduction abnormalities were observed in some patients. An immediate residual leak observed on TTE on the next day was detected in 7 patients (4 patients with perimembranous VSD, 2 patients with muscular VSD, and 1 patient with postoperative residual VSD). However, 6 months later, TTE revealed a residual leak in only 2 patients with perimembranous VSD and 1 patient with muscular VSD. Conduction abnormalities were observed in 3 patients, all with perimembranous VSD. In patient No. 2, right bundle branch block was observed. Patient No. 5 had PR and QRS prolongation, and patient No. 7 had accelerated junctional rhythm (Figure 2). No significant CAVB requiring consideration of a pacemaker was observed. All conduction abnormalities were resolved after steroid pulse treatment. The dose of methylprednisolone was 30 mg/kg/day for 3 days. Two cases were associated with a Cocoon muscular type VSD occluder and one case with a Cocoon duct occluder. The perimembranous VSD size on the LV side measured on TTE images was 4.3 ± 0.75 mm, ranging from 3.5 to 5.8 mm. The muscular VSD in two patients was 4.6 mm and 9.0 mm in size. In the perimembranous VSD closure, the ratio of device waist size to VSD size varied from 1.0 to 2.5, with a mean of 1.6. One patient (No. 2) showed newly developed mild aortic regurgitation on angiography just after deployment. He had perimembranous VSD that was closed with a muscular type occluder. Because the device was not seemed to touch the aortic valve on angiography and parents refused surgery, close observation was recommended rather than surgical removal of the device. Aortic regurgitation was decreased spontaneously but still existed at the 6 month follow-up. However, we could not make clear whether the aortic regurgitation was related to the procedure or device. No hemolysis or embolization was noted on the next day or during the follow-up period.

DISCUSSION
We experienced good results after VSD closure using newly developed Cocoon devices. However, conduction abnormalities and new aortic regurgitation early after perimembranous VSD closure were observed in a few patients. Since the first transcatheter closures of VSD were performed by Lock et al.13) in 1988, many studies have utilized Amplatzer occluder devices.14) Although surgery has been the “gold standard” for treatment of large VSD for many years, transcatheter device closure offers distinct advantages, such as obviating the need for cardiopulmonary bypass, minimizing other complications relating to surgery, reducing the psychological impact, shorter hospital stays, reduced utilization of intensive care units, and faster recovery time to normal activities.15) Transcatheter closure of muscular VSD has been performed successfully for many years,16)17) and the technique has been tried with various devices for perimembranous VSD.18) Although a meta-analysis reported no significant differences between surgical closure and transcatheter closure of perimembranous VSD,18) perimembranous VSD closure with a device remains a challenging procedure. Our indications for VSD closure using Cocoon devices were similar to those for surgery. Left ventricular dilatation on echocardiography was the most important. In spite of left ventricular dilatation, hemodynamic Qp/Qs (range 1.20–2.41) was less than 1.5 in some patients, though this was attributed to inaccurate measurement during the procedure.
Complications of transcatheter closure of perimembranous VSD seem to be limited to the acute phase of the procedure and have been described in small numbers of patients. Reported complications have included aortic and tricuspid regurgitation, device embolization, CAVB, hemolysis, small residual shunts, and perforation. Patients with transient heart block after device placement need to be followed carefully to assess whether they are at risk of later onset permanent heart block.19)20) Two important concerns for percutaneous closure of perimembranous VSD, namely risk of CAVB requiring permanent pacemaker implantation and aortic valve regurgitation, have made this approach less preferable than surgery.18)
The types of Cocoon VSD occluder include membranous, muscular, and aneurysmal types. Depending on the type of VSD, waist length and device type can be determined. Because of the very small number of patients in our experience, it is hard to propose the indications of device selection for each type of device. Muscular type VSD occluder was preferred in most VSD including perimembranous VSD due to concern regarding clumpy force of device. Membranous type of VSD occluder was used for post-operative VSD. Aneurysmal type device was preferred for perimembranous VSD with aneurysm and closed VSD on the LV side. A previous report had described a Korean experience with perimembranous VSD closure with an Amplatzer duct occluder.1) To our knowledge, most of the perimembranous VSD in that experience was associated with an aneurysm, and the device was positioned inside the aneurysm. The Amplatzer duct occluder is very different from the Cocoon occluder for VSD. Accordingly, those results cannot be compared with ours.
Newly developed aortic valve regurgitation was confirmed in only one patient with perimembranous VSD. The main reason of aortic regurgitation in device closure of VSD has known to be mechanical touching of aortic valve by device. Therefore it can be prevented when the defect is located with a distance more than 3 mm from the aortic valve, as with the Cocoon device. Alternately, new aortic regurgitation could develop because of aortic valve damage during the procedure when the device opens at the ascending aorta and passes the aortic valve. In general, newly developed aortic regurgitation should be observed after the device removal, however surgical removal was refused by the parents. It was supposed that we could make clear the reasons of aortic regurgitation by observing after device removal. Therefore it was more reasonable to be confessed that the aortic regurgitation in our patient was from the device or procedure-related complication. But for whatever reason, the long-term outcome of new aortic regurgitation after transcatheter closure of perimembranous VSD remains unclear and should therefore be monitored closely.
CAVB was not observed in our patients. Because the conduction bundle is located very close to a perimembranous VSD, mechanical forces of the device can cause conduction abnormalities.21)22) CAVB is the most serious conduction abnormality after device closure of a perimembranous VSD, and an incidence of 0.3% was reported by Zhao et al.23) The Cocoon occluder for VSD is softer and has a longer waist than the Amplatzer occluder for perimembranous VSD. From these modifications, we expected a reduction in the incidence of CAVB. However, oversized devices should be avoided. We experienced a newly identified arrhythmia other than CAVB after the procedure in three cases of perimembranous VSD. These arrhythmias were detected within 10 days after implantation, and recovery to normal was confirmed. From a Chinese experience, various kinds of transient conduction abnormalities occur more frequently than CAVB,23) which is similar to our experience. Even though most of these transient conduction abnormalities had a benign course, long-term follow-up is mandatory. There was neither hemolysis nor left ventricular outflow obstruction in our experience. In spite of good positions of devices in every patient (Figure 3), residual leaks were observed on 6 month follow-up TTE in three patients, including one patient with muscular VSD. However, these residual leaks were not hemodynamically significant. Considering that the results are from very early experience in a very small series of patients, the complete closure rate is likely to be improved with experience. In general, VSD is elliptical rather than circular in shape, and there might be multiple RV exit holes. Therefore, a clear evaluation for VSD closure prior to intervention is not easy. In addition, residual leaks might occur in order to prevent large CAVB. In any case, the risks of infective endocarditis and outflow obstruction should be monitored carefully afterward.
Figure 3
Transthoracic echocardiogram after the procedure. 4 chamber view (A), parasternal long axis view (B), parasternal short axis view (C), color Doppler image of parasternal short axis view (D).

Study limitations
We describe a very limited experience in a small number of patients. Various types of VSD were included, although the major type was perimembranous. As a result, it is difficult to compare our results to those using other devices. Our follow-up period was very short, and long-term results should be considered for device safety. Because this was an initial experience, there was no standard for device selection in terms of diameter and length.
Conclusions
Cocoon devices can be used safely and effectively for VSD closure. However, residual leaks, newly developing aortic regurgitation and conduction abnormalities may occur, especially early after implantation in patients with perimembranous VSD. Although late complete closure and spontaneous improvement were observed in our patients, long-term evaluation remains essential.
 XML Download
XML Download