

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary vasospasm plays an important role in the pathogenesis of different clinical manifestations of ischemic heart disease, from vasospastic angina (VSA) to variable threshold exertional angina and sudden death.1) VSA can be diagnosed without performing coronary angiography (CAG); patients are considered to have definite VSA when ischemic changes are clearly observed on electrocardiography (ECG) during their attacks.2) If ECG documentation is not performed during the attacks or if ECG findings are unclear, then CAG with drug-induced coronary spasm provocation testing can be performed to provide a definite diagnosis of VSA.2)
Ergonovine stress echocardiography (ErgECHO) has been shown to be a reliable tool for the diagnosis of vasospasm with high diagnostic accuracy.3)4)5)6) However, the safety of performing ErgECHO continues to be questioned given the perceived risk of performing ergonovine provocation without the ability to reverse induced spasm with intracoronary nitroglycerin (NTG) and the limited safety data in large populations.7) Moreover, data supporting its prognostic value are limited. Therefore, the aim of this study was to evaluate the safety and positive rate of ErgECHO testing according to the patients' clinical presentation, and its long-term prognosis in real-world practice.
METHODS
Study population
From November 2002 to June 2009, 3,094 consecutive patients underwent an ErgECHO. The indication for ErgECHO included: 1) patient's refusal to undergo invasive CAG; 2) typical angina without significant evidence of coronary artery disease on CAG and taking β-blocker, calcium channel blocker or nitrate; 3) to rule out coronary vasospasm in patients presenting with atypical symptoms and negative non-invasive functional test. Demographic and clinical data were collected through a chart review of medical records and databanks from our coronary vasospasm registry. Clinical cardiac risk factors, including hypertension, dyslipidemia, and diabetes mellitus were recorded at the time of the ErgECHO. All the patients showed normal left ventricular ejection fraction (>55%) on baseline echocardiography. The Ethical Review Board at Gangneung Asan Hospital approved this retrospective study (2015-011) and waived the informed consent requirement.
Acute coronary syndrome was clinically diagnosed based on the criteria recommended by the current American College of Cardiology and European Society of Cardiology guidelines.8)9)10) A clinical suspicion of VSA was made if typical chest pain, defined as a retrosternal or left anterior chest pain tightness or pressure that lasted up to 15 minutes and could not be located by a single finger, was quickly relieved upon administration of NTG and if any one of the following criteria was met: 1) attacks occurring at rest, particularly between night and early morning; 2) marked diurnal variation observed in exercise tolerance (particularly reduction of exercise capacity in the early morning); 3) attacks induced by hyperventilation (hyperpnea); or 4) attacks suppressed by calcium channel blockers, but not β-blockers.2)
ErgECHO
Except for sublingual NTG, all anti-anginal medications including calcium channel blockers, nitrated and β-blockers were discontinued for at least 48 hours before ErgECHO test to eliminate the possibility of error in result interpretation. An intravenous line was placed in the left upper arm. Noninvasive blood pressure and 12-lead ECG monitoring were performed continuously during the entire procedure. Bolus injections of ergonovine (150 and 200 µg) were administered intravenously at 5-minute intervals until a positive response was obtained or a total dose of 350 µg was reached. Twelve-lead ECG signals were recorded after each ergonovine injection, and left ventricular wall motion was monitored continuously. Regional wall motion was analyzed by 2 experienced cardiologists by using a side-by-side, continuous, cine-loop display method with a commercially available dual- or quad-screen view system. Regional wall motion abnormalities (RWMAs) were generally used to describe any segment assessed as dyskinetic, akinetic, or hypokinetic. RWMA was assessed according to the recommendations of the American Society of Echocardiography by using a 17-segment model,11) and the territory of coronary vasospasm was diagnosed based on the segments showing RWMAs.
The positive criteria for the test included the appearance of transient ST-segment elevation or depression of >0.1 mV at 0.08 s after the J point (ECG criteria) or new RWMAs by 2-dimensional echocardiography (echocardiographic criteria). The criteria for terminating the test were as follows: positive response defined as ECG or echocardiographic criteria, total cumulative ergonovine dose of 350 µg, or development of significant arrhythmia or changes in vital signs (systolic blood pressure of >200 or <90 mmHg). Intravenous bolus injections of NTG (250 µg) and sublingual NTG (0.6 mg) were given immediately after detection of a positive response (ECG or echocardiographic criteria) or at the end of a test with a negative response. Sublingual nifedipine (10 mg) was also administered for possible delayed effects of ergonovine. The administration of these drugs was repeated as needed.5)6)
Clinical follow-up and events
Follow-up data were obtained from hospital records and telephone interviews with the patients and/or their families. The end point of the present study was the occurrence of a major adverse cardiac events (MACEs), defined as cardiac mortality, non-fatal myocardial infarction (MI), and/or any revascularization. Mortality was considered of cardiac origin unless an unequivocal non-cardiac cause of death was established. Revascularization was defined as revascularization of any coronary artery segment with percutaneous coronary intervention or bypass surgery.
Statistical analysis
Continuous variables are expressed as mean±standard deviation; and categorical variables, as number and percentage. Differences between the groups were assessed by using the independent t or χ2 test. Odd ratios and 95% confidence intervals (CIs) were obtained through a multivariate logistic regression analysis for positive ErgECHO test results by using variables that were significant in the χ2 or t-test. Cumulative survival curves were constructed by using Kaplan-Meier methods. Cox regression survival analysis was used to estimate the hazard ratio (HR) for clinical outcomes. A p value of <0.05 was considered statistically significant. Statistical analysis was performed by using the Predictive Analytics Software (PASW) Statistics 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
The baseline characteristics of the study patients are summarized in Table 1. Of the patients, 1,767 (57%) were men, with a mean age of 51±11 years. Prior to ErgECHO, 88% of the patients underwent exercise treadmill tests and 17% underwent thallium 201-labeled myocardial perfusion imaging. CAG was performed in 92 patients (3%), including patients with equivocal results in the noninvasive functional tests to exclude the presence of significant organic stenosis.
Table 1
Baseline characteristics of the patients who underwent ergonovine stress echocardiography (n=3,094)

Data are shown as mean±standard deviation or number (%).
CAG = coronary angiography; PCI = percutaneous coronary intervention; T-Chol = total cholesterol; Thallium scan = thallium 201-labeled myocardial perfusion scan; TMT = treadmill test.
![]()
ErgECHO was performed in an outpatient basis in 85% of the patients. Among the 3,094 tests conducted, no test was terminated prematurely. Ninety-six percent of the patients received a full dose of ergonovine in accordance with protocol. One patient showed RWMAs at the left anterior descending artery territory (LAD) with spontaneous ST-segment depression at the precordial leads before ergonovine injection. Figure 1 demonstrates the indications for ErgECHO, with the most common being evaluation for atypical chest pain (53%), followed by symptoms suspicious of VSA (34%), syncope (3%), and unstable angina (UA) (3%).
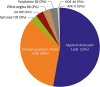 | Figure 1Clinical symptoms or diagnoses of the 3,094 study patients before undergoing ErgECHO. The pie chart shows the frequency and distribution of the initial clinical symptoms or diagnoses of the 3,094 study patients.
AMI = acute myocardial infarction; DOE = dyspnea on effort; ErgECHO = ergonovine stress echocardiography; UA = unstable angina; VSA = vasospastic angina.
|
ErgECHO results
Figure 2 summarizes the ErgECHO results categorized according to initial clinical symptoms or diagnosis. The overall positive rate of the test was 8.6%. While atypical chest pain was the most frequent referral diagnosis, only 1% of the patients had positive results. In addition, 21% of the patients with an initial clinical suspicion of VSA had positive ErgECHO results. Twelve (11%) out of 113 patients with clinical suspicion of UA and negative non-invasive functional test(s) or CAG had positive ErgECHO results.
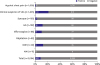 | Figure 2Results of ErgECHO according to initial clinical symptoms and diagnosis (n=3,094). The vertical axis represents the initial diagnosis or symptoms before undergoing ErgECHO. The black areas show the proportion of patients with positive results; and the white areas, proportion of patients with negative results. The numbers within each bar represent the number of patients.
AMI = acute myocardial infarction; DOE = dyspnea on effort; ErgECHO = ergonovine stress echocardiography; UA = unstable angina; VSA = vasospastic angina.
|
The RWMA patterns in the patients with positive ErgECHO results are shown in Figure 3. Multi-vessel territory was observed in 19 patients (7%), and RWMAs were not clearly observed in 3 patients (1%) for various reasons. The right coronary artery territory (RCA) was the most common site of coronary vasospasm (38%), followed by the LAD (36%).
 | Figure 3Frequency and distribution of coronary vasospasm territories during ErgECHO (n=265). Three patients had ischemic ECG changes but no RWMAs (brown area).
ECG = electrocardiography; ErgECHO = ergonovine stress echocardiography; LAD = left anterior descending artery; LCX = left circumflex artery; MULTI = multi-vessel territory; RCA = right coronary artery; RWMA = regional wall motion abnormality.
|
Predictors of a positive ErgECHO result
Table 2 compares the baseline characteristics of the patients with positive and negative ErgECHO results. The patients with positive ErgECHO results were more likely to be older (56 vs. 51 years, p<0.001), to be men (78% vs. 55%, p<0.001), to have diabetes (16% vs. 8%, p<0.001), and hypertension (68% vs. 47%, p<0.001) than those with negative results. Multivariate logistic regression analysis identified age, male sex, hypertension, and diabetes as the independent predictors of a positive, as opposed to a negative, response to ErgECHO (Table 2).
Table 2
Comparison of positive and negative ergonovine stress test group (n=3,094)

CI = confidence interval; OR = odd ratio; PCI = percutaneous coronary intervention; T-Chol = total cholesterol.
![]()
Complications of ErgECHO
Table 3 is a summary of the major symptomatic events in the 3,094 patients that occurred during ErgECHO. We did not experience any procedure-related mortality or MI. During ErgECHO, 19 cases (0.6%) of transient symptomatic adverse events, including atrioventricular (AV) block, marked sinus bradycardia, junctional bradycardia, sinus pause, paroxysmal atrial fibrillation, frequent ventricular and atrial premature complexes, and wide QRS complex tachycardia (14/19 events, 74%), were bradycardia related. Of the 19 events, 12 (63%) were related to positive results. All the events except one were transient and completely recovered spontaneously within several minutes or after intravenous NTG, sublingual NTG, and nifedipine administration. In one patient, complete AV block with bradycardia and hypotension occurred after injection of a cumulative ergonovine dose of 350 µg. She had severe typical chest pain and newly observed RWMAs in the RCA. She was successfully recovered with an appropriate treatment including cardiopulmonary cerebral resuscitation.
Table 3
Major symptomatic events in the 3,094 cases of ErgECHO
AF = atrial fibrillation; APC = atrial premature complexes; AV = atrioventricular; bpm = beats per minute; ErgECHO = ergonovine stress echocardiography; VPC = ventricular premature complexes.
![]()
Clinical outcomes according to ErgECHO results
The 3,094 patients were followed up for a median of 10.5 years (mean, 10.4 years). During this period, all-cause of death occurred in 211 (6.8%) of the 3,094 patients, which was significantly higher in the positive ErgECHO group than in the negative group (14.3% vs. 6.1%, p<0.001). The incidence of cardiac death, acute coronary syndrome, MI, and revascularization were all significantly higher in the positive ErgECHO group. The cumulative MACE rate in the patients with positive ErgECHO results was 14.0% (37/265), which was also significantly higher than that in those with a negative ErgECHO result (5.1%, 143/2,829, p<0.001; Table 4).
Table 4
MACEs of the study patients during follow-up

Data are shown as number (%).
ErgECHO = ergonovine stress echocardiography; MACEs = major adverse cardiac events; MI = myocardial infarction.
![]()
The Kaplan-Meier curve showed that the patients with positive ErgECHO results had significantly lower MACE-free survival than those with negative results (HR, 2.95; 95% CI, 2.06–4.24; log-rank p<0.001; Figure 4). Cox regression survival analyses revealed that among the various clinical variables, male sex (HR, 1.86; 95% CI, 1.33–2.59; p<0.001), age (HR, 1.08; 95% CI, 1.07–1.10; p<0.001), presence of diabetes (HR, 2.43; 95% CI, 1.70–3.49; p<0.001), total cholesterol level of >220 mg/dL (HR, 1.43; 95% CI, 1.06–1.94; p=0.02), and positive ErgECHO result (HR, 1.77; 95% CI, 1.22–2.57; p=0.003) were independent factors associated with MACEs. In the positive ErgECHO group, no relationship was observed between the location of ischemic segments or the presence of symptomatic events during the provocation test and subsequent cardiac events.
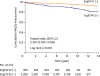 | Figure 4Kaplan-Meier estimates of cumulative MACEs-free survival curves in the patients grouped according to ErgECHO result. The figure shows the Kaplan-Meier estimate of the cumulative MACE-free survival. The mean and median follow-up durations were 10.4 and 10.5 years, respectively. In the comparison with stratification according to ErgECHO result, the HR for MACEs was 2.951 (95.1% CI, 2.055–4.236; p<0.001).
CI = confidence interval; ErgECHO = ergonovine stress echocardiography; HR = hazard ratio; MACEs = major adverse cardiac events.
|
DISCUSSION
To our knowledge, this study represents the largest cohort of patients who underwent ErgECHO. We demonstrated that ErgECHO is a safe non-invasive diagnostic test for coronary vasospasm and provides useful prognostic information for appropriately selected patients. However, the positive rate of ErgECHO was relatively poor for most patients except for those with clinical suspicion of VSA.
The overall incidence of symptomatic complications in this study was 0.6% (19/3,094), which is lower than those reported in previous reports.3)6) In addition, 63% of the complications (12/19) were associated with positive ErgECHO results. Song et al.6) observed complications in 1.9% (26/1,372) of their patients, but they did not document the number of symptomatic patients in their study and 20 out of 26 events were not associated with any positive test response. Our complication data showed only symptomatic patients indicated in the medical records because we did not collect data considered to be non-major common adverse events such as headache, nausea, anxiety, and sinus bradycardia (>40 bpm), which were not related to the positive results and resolved spontaneously within several seconds without any sequelae. However, the incidence of AV block in this study was the same as that in the study by Song et al.6) (0.3%). Three cases of tachycardia events occurred, including 2 cases of paroxysmal atrial fibrillation with rapid ventricular response lasting less than several minutes and one case of non-sustained wide QRS complex tachycardia. While the 2 paroxysmal atrial fibrillations were not associated with the positive results, the wide QRS complex tachycardia after intravenous injection of NTG was related to RWMAs at the LAD.
What cardiologists are concerned of the most might be mortality associated with intractable spasm. One case of cardiac arrest during ErgECHO was reported12); however, thus far, ErgECHO test-related mortality has been scarcely reported. The incidence of fatal ErgECHO complications (0.3%) appears to be similar to that of dobutamine stress echocardiography, which is commonly used for the diagnosis of coronary artery disease.13) In VSA, ventricular arrhythmias may result from coronary artery occlusion and/or reperfusion; both types correlate with the severity of ischemia, and reperfusion arrhythmias are associated with the duration of ischemia.14) Even if such an event occurred in only 1 of 1,000 patients during the test, the outcome could be catastrophic, as no central venous access was available for temporary pacing or intracoronary catheter for immediate intracoronary medicine infusion. In addition, intravenous NTG, which can relieve both symptoms and RWMAs in patients with a positive response, requires 2–5 minutes to take effect.
According to previous studies, the development of RWMAs of the left ventricle is known to be an early phenomenon of myocardial ischemia and can be detected on echocardiography before any ECG change during spasm provocation testing in the catheterization laboratory.15)16)17) Therefore, the best way to prevent test-related mortality and cardiac arrest is not to delay the administration of NTG and to carefully monitor patients throughout the test phase and even after completion of the test, especially in patients with large ischemic territories or long ischemia durations during the assessment.
Among the 3,094 tests completed, 265 (8.6%) showed positive results, which was a lower rate than those indicated in previous reports.3)6)18) The low positive ErgECHO result rate may be due to over-testing. Nevertheless, ErgECHO showed a similar positive rate as the ergonovine-provoked CAG for those patients with clinical suspicion of VSA. During the concomitant study period, 271 (25%) of 1,105 patients were diagnosed as having VSA by using ergonovine-provoked CAG in our institution. Consequently, ErgECHO may be useful to confirm clinical suspicion of VSA. It could also be an alternative non-invasive tool for those patients who are not good candidates for CAG such as kidney failure, allergy to contrast medium or refuse to undergo CAG.
A considerable number of patients with UA might reveal near-normal coronary angiograms; ErgECHO has detected coronary vasospasm in some of these patients.19) In this study, although the most common referral symptom for ErgECHO was atypical chest pain, only one of every 5 patients with a positive ErgECHO result presented with atypical chest pain. We believe that several physicians at our institute tend to order ErgECHO to rule out the small possibility of VSA in patients with atypical or ambiguous symptoms. On the other hand, we should keep in mind that vasospasm of the small coronary arteries may also be implicated in some patients with atypical chest pain.20)
The prevalence of VSA may be decreasing globally due to increased use of calcium channel blockers or under-diagnosis of VSA using the spasm provocation tests.1)21) Specifically, a recent study in Europe has shown that nearly 50% of patients who underwent diagnostic CAG for typical exertional chest pain had angiographically normal or near-normal coronary angiograms.22)23) Similarly, a large American College of Cardiology National Cardiovascular Data Registry database of 565,504 patients showed only 45% median rate of obstructive coronary artery disease.24) According to our literature review, most studies did not have a control group to investigate long-term clinical outcome of VSA (i.e., subjects with negative results in spasm provocation tests).25)26)27)28)29)30) In this study, the cumulative MACE rate among the patients with positive ErgECHO results was higher than those with negative ErgECHO results (12.7% vs. 3.4%, p<0.001). Our result is concurring with one of the studies with a control group (14.0% vs. 5.1%, p<0.001).18) Thus, this may imply that a positive ErgECHO test could be an independent risk factor for long-term MACEs. It would also be imperative for clinicians to consider coronary vasospasm as an important part of non-obstructive coronary artery disease pathophysiology.
Although this is a retrospective analysis of data obtained in a single-center, the number of patients in this study is sufficiently powered. We could not address the sensitivity and specificity of our ErgECHO results because our analysis focused on the safety of ErgECHO and we did not perform any other provocation tests such as a hyperventilation test or ergonovine-provoked CAG in all our study populations during the same study periods. Finally, in our echocardiography laboratory, we did not collect data about smoking, which is an important risk factor of VSA. Despite these limitations, the detailed account of our center's experience regarding the clinical characteristics of referred patients, observed results, complications, and long-term clinical impact may provide physicians helpful information about patients undergoing ErgECHO.
In conclusion, ErgECHO can be performed safely by experienced physicians and its positive result may be associated with long-term adverse outcomes. It may also be an alternative tool to ergonovine-provoked CAG for patients with clinical suspicion of VSA.
 XML Download
XML Download