

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) has generally been considered an inherited cardiomyopathy, which was first described in 1965.1) The defective cell-to-cell adhesion, which was mainly caused by seven dominant gene mutations that encode desmosomal proteins, is believed to be responsible for the pathogenesis of ARVD/C. As a consequence, the inflow tract of right ventricle (RV), RV apex, and right ventricular outflow tract (RVOT) are predisposed to the loss of cardiomyocytes and the substitution of ventricular myocardium to fibro-fatty tissue, which usually extends from the epicardium toward the endocardium.2)3) The inhomogeneous fibro-fatty infiltration of myocardium could result in slow conduction and anisotropic electrical propagation that potentially contribute to the arrhythmogenic substrates for reentrant circuits in ARVD/C. Apart from the above, the posterior lateral portion of left ventricle (LV) could be involved in an estimated 10% of patients with ARVD/C, which is frequently seen at the late stage of clinical course.4)5)Accompanying the histopathological changes, clinical manifestations of ARVD/C could vary from syncope, ventricular tachyarrhythmias, progressive heart failure (HF), and sudden cardiac death (SCD).5) Owing to the diverse phenotype, the 2010 modified task force criteria have been proposed to facilitate the diagnosis of ARVD/C.6) It is worth noting that ventricular arrhythmias (VAs) and the associated symptoms frequently bring patients with ARVD/C to medical attention, and an implantable cardiac defibrillator (ICD) implantation is highly desirable to prevent SCD or recurrent symptoms in patients with definite ARVD/C, especially among those with unexplained syncope, hemodynamically unstable ventricular tachycardia (VT), ventricular fibrillation (VF), and aborted SCD.
The clinical management of patients with ARVD/C aims at 1) reducing the mortality; 2) decreasing VT recurrences and/or ICD interventions (either appropriate or inappropriate); 3) preventing ventricular dysfunction and progressive HF; 4) improving symptoms and quality of life; and 5) increasing the functional capacity.7) To achieve these goals, multidisciplinary strategies, including restriction of intense exercise, antiarrhythmic drug therapies, and catheter ablation, are warranted.7)8) However, clinical hurdles persist for those with frequent drug-refractory ventricular tachyarrhythmias in ARVD/C. Amiodarone with and without beta-blockers have been considered to prevent the occurrences of ventricular tachyarrhythmias in patients with ARVD/C with nonuniform effectiveness.9)10) However, given the unsatisfactory efficacy and the potential adverse effects, clinical application of antiarrhythmic drugs in ARVD/C would be limited, especially for those with young age and high activity. Therefore, catheter ablation was implemented to treat the ventricular tachyarrhythmias in ARVD/C for decades. In the era of endocardial ablation, the catheter ablation was considered palliative treatment because of the high recurrences of ventricular tachyarrhythmia.11)12)13) The critical epicardial nidus of VT circuits in patients with ARVD/C explains the potential failure of conventional endocardial mapping and catheter ablation.12)14)15) The better understanding of the epicardial electro-pathologic substrates contributing to the ventricular arrhythmogenesis in patients with ARVD/C and the improvement of navigation mapping system enable the electrophysiologists to localize and target the critical VT isthmuses and yield higher procedural success and lower VT recurrences through the incorporation of endocardial and epicardial ablation.16)17) The above evolution enhances the promising effectiveness of catheter ablation to be the preferred strategies for ARVD/C patients with clinically-documented VTs.
DIAGNOSIS OF ARRHYTHMOGENIC RIGHT VENTRICULAR DYSPLASIA/CARDIOMYOPATHY
The appropriate management of VT strongly relies on the clinician awareness and accurate diagnosis of ARVD/C. The International Task Force criteria for the diagnosis of ARVD/C was first proposed by McKenna et al.18) in 1994 and revised by Marcus et al.6) in 2010 through the incorporation of new knowledge and technology to improve the diagnostic sensitivity. Patients with suspicion or at-risk of ARVD/C should be evaluated by serial evaluations consisting of family history, electrocardiography (ECG), signal-averaged ECG, echocardiography and/or cardiac magnetic resonance imaging, Holter monitoring, and genetic analysis, and/or RV angiography, RV endomyocardial biopsy.19) In spite of the above information, distinguishing ARVD/C from other mimicking diseases, such as idiopathic RVOT VT, amyloidosis, myocarditis, sarcoidosis, or endomyocardial fibrosis, is sometimes challenging but of clinical importance in the viewpoint of ablation strategy and prognosis.20)21)
PATIENTS SELECTION FOR CATHETER ABLATION IN ARRHYTHMOGENIC RIGHT VENTRICULAR DYSPLASIA/CARDIOMYOPATHY
VAs in patients with ARVD/C frequently bring to medical attention as the initial manifestation during the second to fifth decade of life. The clinical manifestations of VA can range from isolated premature ventricular complex (PVC), non-sustained or sustained VT, to fatal ventricular flutter (VFL) and VF. Although there were no randomized trials to demonstrate the benefit of an ICD implantation in patients with ARVD/C, observational studies have consistently shown the effect to prevent SCD,9)22)23) mostly driven from episodes of VF or hemodynamic intolerable sustained VT. Hitherto, the updated guideline recommended an ICD implantation for the patients with ARVD/C with documented sustained VT/VF or survivors experiencing aborted SCD provided the high recurrences of VA-associated mortality or morbidity.24) In spite of several risk factors have been identified, it remains controversial for those at-risk or without life-threatening VAs to receive an ICD implantation as primary prevention.7)25)Furthermore, beta-blocker and other anti-arrhythmic drugs are frequently limited by the intolerable adverse effect or the unsatisfactory effectiveness to avoid the recurrent episodes of VAs and ICD interventions. Given the advancement of ablation techniques and mapping system, there are growing shreds of evidence to demonstrate the role of catheter ablation in preventing the recurrent VTs in patients with ARVD/C. Previously, catheter ablation was only considered an alternative choice for drug-refractory VTs. Nevertheless, though there was no randomized trial to investigate the timing of VT ablation in ARVD/C, recent study demonstrated that early referral for VT ablation in structural heart diseases was associated with less VT recurrences and the occurrences of acute complications.26) Future works are needed to elucidate the role of ablation as the initial step once if patients with ARVD/C have documented VTs. Also, the benefits of ablation in ARVD/C patients with inducible VTs during invasive electrophysiologic studies without clinically-documented VTs or patients presenting with PVC or VF remain questionable.
ELECTROPHYSIOLOGICAL STUDY IN ARRHYTHMOGENIC RIGHT VENTRICULAR DYSPLASIA/CARDIOMYOPATHY
First, the electrophysiological study could yield the valuable information to differentiate idiopathic RVOT VT from ARVD/C.27) The programmed electrical stimulation not only have a pivotal role to assess the vulnerability of ventricular tachyarrhythmias, but also provide clues for the diagnosis of ARVD/C. Denis et al.28) demonstrated that either the presence of polymorphic premature ventricular contractions with ≥1 couplet, sustained or non-sustained VT with left bundle branch block morphology after excluding RVOT VT by high dose isoproterenol (45 μg/min) infusion could help to diagnose ARVD/C in the early stage with a sensitivity of 91.4% and a specificity of 88.9%. Apart from the above, the role of inducible sustained VT or VF to predict future arrhythmic outcome remained unsolved.29)30) The multicenter studies demonstrated the limited value of programmed ventricular stimulation as a risk stratification strategy in patients with ARVD/C who carry the risk of fatal VA or cardiac arrest.9)23) Corrado et al.23) reported that the positive and negative predictive value of VT/VF inducibility for substantial outcome in patients with ARVD/C receiving an ICD implantation as primary prevention was 35% and 70%, respectively. The North American Multidisciplinary study also echoed the above findings that spontaneous VA before enrollment and a younger age of ICD implantation rather than the inducible VT/VF by programmed stimulation can predict the occurrence of life-threatening VT/VF in patients ARVD/C.31) However, Bhonsale et al.29) demonstrated that only positive inducibility and non-sustained VT could predict appropriate ICD therapy in patients with definite or probable ARVD/C receiving ICD implantation for primary preventions after multivariable analysis. The above conflicting findings may be caused by the heterogeneous study population, diverse disease spectrum, the different protocol of programmed stimulation, and the non-uniform endpoints.
Nowadays, catheter ablation is emerging as one of the therapeutic options to prevent VT recurrences in the patients with ARVD/C through the combination of endocardial and epicardial approaches.13)32) The understanding of the electrophysiologic characteristics and electroanatomic substrates responsible for the ventricular arrhythmogenesis was derived from the reports of international electrophysiologic laboratory over the world. The detailed electrophysiologic study during catheter ablation not only help understand the underlying characteristics, reproduce clinically-documented VT, but also help to assess the ablation outcome. Through these experiences, the mechanism of ventricular arrhythmogenesis and ablation strategies have been learned to facilitate successful catheter ablation and long-term freedom from VT recurrences.
CATHETER SELECTION FOR SUBSTRATE MAPPING
Some electrophysiologists use the traditional mapping catheters with a 3.5 mm distal tip electrode that is separated by 2 mm from a 2 mm proximal electrode for substrate mapping. Therefore, the bipolar electrogram only represents the underlying tissue diameter ranging from 3.5 to 7.5 mm. The newly developed multielectrode mapping catheters with ≤1 mm electrodes and shorter inter-electrode spacing can record the electrogram from a significantly smaller underlying tissue diameter ranging from 1 to 3 mm (also dependent on catheter orientation relative to the surface). The small electrodes and shorter inter-electrode spacing of multielectrode mapping catheter demonstrated the advantages of not only higher density but better resolution of the abnormal substrates, which could therefore facilitate to delineate the heterogeneous area of low voltage and to localize the potential channels compositing surviving myocardial bundles that might be responsible for the development of VAs in ARVD/C (Figure 1).33) In spite of the better illustration of the abnormal electrograms, current automatic annotation criteria of the navigation system may not be precise enough, especially for fractionated low voltage signals in the scarred myocardium and manual adjustment and exclusion of noise and artifacts are frequently needed.34) The improvement of annotation algorithms will be highly desirable to overcome the current frontier.
Figure 1
Example of differences in the bipolar voltage map created using the 1-mm electrode catheter and 3.5-mm electrode catheter in the patient with ARVD/C. During substrate mapping and activation mapping, the 1-mm electrode catheter (upper panel) identified the potential channels (white arrows and white arrowheads) in the epicardial RV inferior free wall and inferior tricuspid annulus (left and middle panel). The local electrograms of 1-mm electrode catheter showed delayed fractionated potential at the distal part of the conducting isthmus during sinus rhythm (right penal). On the other hand, the 3.5-mm electrode catheter (lower panel) in the same area could not identify the conduction gap within the epicardial scar in the same area (left and middle panel). The local electrograms of 3.5-mm electrode catheter only identified far-field potential at the same area during sinus rhythm (right penal).
ARVD/C = arrhythmogenic right ventricular dysplasia/cardiomyopathy; ECG = electrocardiography; RV = right ventricle.
ENDOCARDIAL AND EPICARDIAL SUBSTRATE MAPPING IN ARVD/C
Advances in 3-dimensional (3D) electroanatomic mapping fasten the electrophysiologists to understand the throughout substrate properties in patients with ARVD/C, which can be helpful to localize the VT origins. The distribution of electroanatomic scar in patients with ARVD/C typically extends from the tricuspid annulus and RVOT toward the RV free wall and RV apex, which was known as the triangle of dysplasia (Figure 2) despite that the LV abnormalities surrounding the basal perivalvular area have been reported.11) The detailed assessment of substrates underlying these arrhythmogenic areas during sinus or paced rhythm by 3D-colored electroanatomic voltage mapping provides pivotal insights to localize the reentrant circuits and decide the ablation strategies.
Figure 2
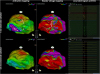
3D electro-anatomic characteristics in the patients with ARVD/C. Example of substrate mapping in a patient with definite ARVD/C. The distribution of electroanatomic bipolar and unipolar scar typically extends from the tricuspid annulus and RVOT toward the RV free wall (A–C) and RV apex. The septum was scar-sparing. The electroanatomic bipolar epicardial scar area was correlated to the endocardial unipolar low-voltage area at a cut-off threshold of 5.5 mV (D).
3D = 3-dimensional; ARVD/C = arrhythmogenic right ventricular dysplasia/cardiomyopathy; AP = anteroposterior; PA = posteroanterior; RV = right ventricle; RVOT = right ventricular outflow tract; TV = tricuspid valve.

In our laboratory, we defined the bipolar voltage <1.5 mV, prolonged electrogram duration, fractionated potentials, and isolated late potentials (LPs) as the abnormal substrates of RV endocardium,35)36)37) whilst the voltage threshold of 1.0 mV is used for the setting of epicardial bipolar voltage mapping.38) These abnormal low voltage areas were frequently correlated with the histopathologic findings of myocyte loss with fibrofatty replacement in patients with ARVD/C,19) whilst the distribution of abnormal electrograms is usually comparable to the VT reentrant circuits.39) Sometimes, the potential channels and VT isthmuses can be visualized through the adjustment of voltage limit within the widespread scar area.40) Noteworthy is that the thick epicardial fat layer surrounding atrioventricular/interventricular grooves or adjacent to epicardial coronary vessels can result in epicardial bipolar low voltage area without the existence of abnormal fractionated or isolated electrograms.41) Imaging modalities such as cardiac computed tomography and magnetic resonance imaging can be integrated to the electroanatomic map to delineate theses epicardial structures beyond the scar/low voltage zone. Operators should carefully review all the electrograms surrounding these epicardial vessels to prevent the overestimation of the low-voltage area or accidental vascular complication during ablation. The previous study based on contrast-enhanced magnetic resonance imaging also supported that the bipolar low voltage area and the territories displaying abnormal electrograms were correlated to the transmural scar.41)42)
In general, the disease process in ARVD/C initiates from the epicardium toward the endocardium. It is reasonable that the epicardial scar is larger than those within endocardium in ARVD/C (Figure 2). Though the endocardial substrate mapping is traditionally considered the first step, it is important to evaluate the estimated extent of RV epicardial substrates and clarify the benefit and necessity of epicardial approaches in patients with ARVD/C noninvasively. Moreover, the epicardial abnormal substrate is usually the target for successful VT ablation.15)43) However, elimination of epicardial circuit from endocardial ablation could be achieved in certain patients.44) Given the concern of safety and complications, an epicardial approach has been reserved for patients with failed endocardial ablation of VT in ARVD/C in certain electrophysiological laboratories.14) In the viewpoint of the above consideration, recognition of the potential epicardial substrates/circuits is of clinical significance.
First of all, the depolarization and repolarization manifestations of 12-lead ECG have been correlated with the substrate characteristics of ARVD/C in several studies. Tanawuttiwat et al.45) demonstrated that the presence of epsilon wave could be associated with severe conduction delay and the extensive endocardial scarring within the sub-tricuspid area based on the activation timing of epsilon wave. Tschabrunn et al.46) also reported the fragmentation of QRS in different territories provides information to localize the abnormal electroanatomic substrates and the origin of VAs. Furthermore, Kubala et al.47) demonstrated the area with abnormal electroanatomic mapping could be correlated to the extent of T wave inversion, while the down-sloping elevation of ST-segment in V1 and V2 was associated with larger abnormal endocardial unipolar voltage. The interelectrode dispersion of 12-leads ECG during sinus rhythm in ARVD/C reemphasized the importance of conduction heterogeneity in the contribution of depolarization abnormalities,48) whilst the Q wave or QS in regional leads during VAs may reflect the probable epicardial origin for RV VT.49) Second, unipolar voltage mapping of RV endocardium has been explored to predict the disease and the epicardial arrhythmogenic substrates.37) The RV endocardial voltage mapping not only illustrates the substrate characteristics but helps to evaluate the extent of epicardial abnormalities. Evaluation of the epicardial abnormal substrates can be achieved using the RV endocardial unipolar voltage mapping with a cutoff value of 5.5 mV, and the abnormal area is correlated to the epicardial scar in ARVD/C (Figure 2),37) though the different cut-off value of 4.4 mV has been proposed through the site-by-site comparison.50) Our group also found that the RV endocardial unipolar peak-negative voltage at a cut-off value of 1.66 mV is useful to predict the epicardial dense scar (<0.5 mV) in ARVD/C.51) Aside from the above, the discrepancy between endocardial and epicardial scar distribution was associated with the development of fatal VAs. In terms, the horizontal expansion rather than the transmural distribution of the substrates may result in the likelihood of electrical instability and predisposition to unstable ventricular tachyarrhythmias as the initial presentation.15) It is notably crucial to identify and annotate the location of fractionated signals, LPs, and/or high-frequency arrhythmogenic potentials which are potentially responsible for the VT isthmuses. Pacing maneuver or the novel simultaneous amplitude frequency electrogram transformation may facilitate the recognition of these arrhythmogenic potentials and elimination of these abnormal electrograms could potentially yield better prognosis.39)52)53)54)
MAPPING OF VENTRICULAR TACHYCARDIA AND ABLATION STRATEGIES
The majority of VAs in ARVD/C is VT, though VF/VFL can still occur.29) Multiple monomorphic VTs in patients with ARVD/C were not rare, which therefore attract clinical electrophysiologists' interests to eliminate these catastrophic events through catheter ablation. The VT induction in ARVD/C usually can be achieved by programmed ventricular stimulation with or without isoproterenol. Once if the VT is induced, the morphology should be compared to clinically-documented VT, if available, and/or the ICD electrograms recorded.
Identification of the initiation and perpetuation of ventricular reentry is the primary objection during mapping of the VT isthmuses because the visualization and delineation of the critical components of the circuits can facilitate to effectively terminate the VTs through limited ablation. For hemodynamically-tolerable VT, the localization of the critical isthmuses relies on both activation and entrainment mapping. Pacing from the mapping catheter at a cycle-length of 20–30 msec faster than the tachycardia cycle length is needed when entrainment mapping was performed. The VT isthmuses are confirmed once the following criteria are achieved; 1) concealed fusion of all 12-lead ECG during entrainment, 2) the post-pacing interval within 30 msec of the VT cycle length, 3) the stimulus-to-electrogram interval was within 20 msec of the electrogram-QRS interval following entrainment, and 4) the local electrogram to QRS interval is between 30% and 70% of the VT cycle length.55) Notwithstanding the foregoing the above criteria, there are still several pitfalls during the entrainment pacing and accurate interpretation of the results could sometimes be challenging.56) Furthermore, recent findings from high-resolution mapping demonstrated that entrainment mapping may overestimate the lengths of VT isthmuses in a post-infarct experimental model.57) Therefore, high-density and high-resolution activation mapping by the acquisition of the earliest fractionated or splitting mid-diastolic potentials preceding QRS by at least more than 30 msec would be better to illustrate the VT isthmuses. Of interest, the endocardial electroanatomic activation mapping of VT frequently represents a centrifugal activation pattern with radial spreading. Usually, concealed entrainment could be achieved at the earliest activation site, implying the potential exit of the reentrant circuit.58) In patients with ARVD/C, the tricuspid annulus is frequently involved in the VT circuits. Therefore, the whole annulus should be mapped in detail. The application of long deflectable sheath is recommended to achieve the adequate contact and catheter stability. Nevertheless, unmappable VTs are frequently encountered in ARVD/C, mostly owing to the hemodynamically unstable condition, multiple reentrant circuits, or non-sustained VT. Though pace mapping in scar-related VT is less precise, pacing surrounding the dense scar border can help to identify the VT exit.59) Despite that only a minority of fractionated potentials may participate in the VT isthmuses,60) extensive substrates modification through local abnormal ventricular activities elimination,52) scar homogenization,61) scar dechanneling,62) or core isolation63) have been proved to decrease VT recurrences given the and was associated with better outcome. Given the potential fraught of voltage-based assessment, several different methods, such as fragmentation or frequency analysis mapping,39)64) decrement evoked potentials mapping,65) ripple mapping,66)67) isochronal late activation mapping,68) or omnipolar mapping,69) have been proposed to assist in more effective and objective analysis of abnormal potentials or potential channels supporting VT isthmuses. Substrate modification relying on the integration of the above methods is usually the strategy of choice to achieve acute procedural success.
To date, radiofrequency is the most common energy source applying for VT ablation. A 3.5 or 4-mm irrigated-tip catheter is widely accepted to be more effective to create deeper lesions for intramural or epicardial circuits.70) In our laboratory, the power delivery is usually initiated at 30 W for the endocardial site and 20 W for epicardial site. The energy is titrated up to a maximum of 40 W for endocardium and 35 W for the epicardium while targeting an impedance drop of 10 Ω by maintaining for a minimum of 120 seconds to site of termination in stable VT or the disappearance of abnormal potentials at each point for substrate modification.
CONSIDERATION OF EPICARDIAL ABLATION
Though the percutaneous pericardial access was firstly introduced for epicardial VT ablation in Chagas disease in 1996, it has currently been applied to several different entities of diseases, such as ARVD/C, idiopathic dilated cardiomyopathy, ischemic cardiomyopathy with transmural scar, myocarditis, and Brugada syndrome.11)71)72)73)74)75)76) Epicardial approach has been proved to provide a better understanding of the arrhythmogenesis of abnormal substrates and ablation efficacy.77)78)79) However, the epicardial procedure still carries certain risks of catastrophic complications, such as coronary vessel injuries, major bleeding, delayed tamponade, or major pericardial reaction, even in the experienced and high-volume centers.80) Aside from the above, the presence of thick epicardial fat constraints the energy penetration to the protected isthmus,81)82) and endocardial ablation has been reported to be able to eliminate the epicardial local abnormal ventricular activities in 73% of patients with ARVD/C (Figure 3).44) Therefore, the first-time application of epicardial procedure should be balanced between the benefits of procedural success and the risk of procedure-related cardiac or extra-cardiac complications.83)84)85)
Figure 3
Elimination of epicardial arrhythmogenic potentials by endocardial catheter ablation. An example of elimination of epicardial LPs by endocardial ablation in a patient with ARVD/C and sustained VT. 2 clinical VTs with difference axis were induced during the electrophysiological study (A). The ablation catheter and multielectrode catheter nearby the corresponding isthmus showed mid-diastolic potentials (yellow stars) during VT and delayed potential after VT terminated into sinus rhythm (B). Catheter ablation from the endocardium eliminated the LPs of the corresponding epicardial area successfully. Notably, the epicardial LPs were disappeared before the elimination of endocardial LP (yellow stars). Additionally, the programmed extra-stimuli revealed non-inducible after ablation. The 3D electro-anatomic mapping of epicardial showed the conducing isthmus surrounded by epicardial scar. The shadow of the multielectrode catheter represented the position during VT mapping and endocardial ablation (D, E).
3D = three-dimensional; ARVD/C = arrhythmogenic right ventricular dysplasia/cardiomyopathy; EP = electrophysiological; LP = late potential; VT = ventricular tachycardia.

OUTCOME OF VENTRICULAR TACHYCARDIA ABLATION IN ARRHYTHMOGENIC RIGHT VENTRICULAR DYSPLASIA/CARDIOMYOPATHY
Most of the literatures reported the ablation outcome of ARVD/C from limited and nonuniform population, the different ablation strategies, distinct disease stages, and variable follow-up duration with heterogeneous results (Table 1).12)13)15)17)32)86)87)88) Initially, the long-term efficacy in prevention of VT recurrence could be achieved in only 25–53% of cases by endocardial ablation.86)87) The understanding of the underlying pathophysiology of ARVD/C and the application of epicardial ablation improved the unsatisfactory outcome.12) Recent studies demonstrated a significant benefit of freedom from VT recurrences or ICD therapy by 45–84.6% through the combination of endocardial and epicardial ablation.12)13)15)17)32)88) Again, the non-uniform ablation outcomes were likely caused by the mapping and ablation strategies, the variable endpoints, follow-up assessment, and operators' experiences.12)55)58)86)89)90) Even though there has been a great improvement in ablation techniques and clinical outcomes through epicardial ablation, clinical hurdles remain in the realm of managing patients after the failed epicardial ablation, patients with recurrences owing to rapid disease progression.
Table 1
Clinical outcome of VT ablation in ARVD/C

| Author | Number of patients | Mapping strategies | Sites of targets | Acute results | Follow-up duration | Short-term freedom from VA recurrences (≤1 years) | Long-term freedom from VA recurrences |
|---|---|---|---|---|---|---|---|
| Dalal et al.87) | 24 | Conventional or 3D mapping | Endocardial | 46% for all inducible VT; 31% for clinical VT; 23% procedural failure | 32±36 months | 50% (5 months) | 25% |
| Verma et al.88) | 22 | 3D mapping | Endocardial | 82% | 37 months (median) | 77% (1 years) | 53% |
| Garcia et al.12) | 13 | 3D mapping | Endocardial+epicardial | 92% (for all targeted VT) | 18±13 months | - | 77% |
| Philips et al.13) | 87 | Conventional or 3D mapping | Endocardial+epicardial | Complete success 47%; partial success 38%; procedural failure 15% | 88.3±66.1 months | 1 years: 47% (endocardial: 45%; epicardial 64%) | 5 years: 21%; 10 years: 15% (5 years-endocardial 19%; 5 years-epicardial 45%) |
| Bai et al.32) | 49 | Conventional or 3D mapping | Group 1: endocardium alone, (n=23); group 2: endo+epicardium (n=26) | Polymorphic VT/VF: 1 in group 1 and 2 in group 2 | At least 3 years | 300 days follow-up | 3-years follow-up |
| group 1: 1,224±310 days; group 2: 1,175±112 days | group 1: 88.5%; group 2: 100% | group 1: 52.2%; group 2: 84.6% | |||||
| Santangeli et al.17) | 62 | 3D mapping | Endocardial±epicardial | VT non-inducibility: 71% | 56±44 months | - | 71% |
| Wei et al.89) | 48 | 3D mapping | Endocardial±epicardial | 81.3% | 71.4±45.7 months | - | 56.3% |
| Lin et al.15) | 80 | 3D mapping | Endocardial±epicardial | 100% | 38±11 months | 95% (1 year) | 51.2% |
CONCLUSION
In summary, ARVD/C is predominantly an inherited progressive disease with fibrofatty infiltration and potentially the ventricular arrhythmogenesis. An early and accurate diagnosis relies on the detailed evaluation of cardiac imaging, ECG, histopathology, family history, genetic screening, and electrophysiological study in selected cases. Provided the better understanding of the pathogenesis, the underlying substrate properties, improvement of navigation mapping system, and widespread of epicardial approaches, ablation outcome has been tremendously improved to reduce recurrent VT and ICD therapies, and therefore catheter ablation is emerging as a preferred therapeutic choice for VT in ARVD/C in well-developed electrophysiological laboratories. Further investigations are warranted to elucidate the role of catheter ablation as the first line therapy or primary ablation of VT in patients with ARVD/C, and the novel solution for those with failed endocardial/epicardial ablation or recurrent VT caused by rapid substrate evolution.
 XML Download
XML Download