

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary liver sarcomas are unusual neoplasms in adulthood and constitute approximately 0.2% of all primary liver tumors.1 They represent a heterogeneous group of neoplasms including undifferentiated embryonal sarcoma (UESL), which was first described by Stocker and Ishak2 in 1978 as a mesenchymal tumor without any specific differentiation. Until now, few adult patients with UESL have been reported in the literature, with a slight preference for females and a mean age at diagnosis of 51.3 Although UESL is associated with prognosis with a reported survival time of less than one year, early diagnosis is essential to increase the overall survival.4
CASE
Case 1
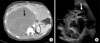
A 53-year-old female presented with abdominal distension and pain localized to the right upper abdominal quadrant radiating to the back. It was partially controlled with oral analgesia and was associated with fever. Due to pain progression, the patient was treated at the emergency department three months later for diaphoresis and dyspnea on exertion associated with right chest wall pain that irradiated to ipsilateral shoulder. On examination, the patient presented with abdominal distension and a painful palpable mass in the right hypochondrium. Laboratory studies indicated leukocytosis and neutrophilia, while the liver tests were normal. Multiphase contrast-enhanced computed tomography scan showed a liver with an occupying hypodense mass in the right lobule and heterogeneous reinforcement in the periphery, a central necrotic component and satellite lesions in the 6th and 8th segments. Importantly, a 39 mm left auricular multi-lobulated mass associated with a lytic lesion was detected in the fourth right costal arch, both of which suggested secondary deposits (Fig. 1).
The patient was hospitalized for extensive work-up and initiated with intravenous antibiotics. Evaluation of intracardiac lesion included a transthoracic echocardiogram, which demonstrated a multinodular image attached to left auricle causing intermittent obstruction with a gradient of 32 mm/Hg. The right ventricle was dilated (43 mm) with tricuspid annular plane systolic excursion (TAPSE) of 18 mm suggestive of right heart failure and pulmonary hypertension confirmed by a pulmonary artery systolic pressure (PASP) of 87 mmHg. Biopsy of the hepatic lesion revealed no complications and revealed undifferentiated embryonal sarcoma. Throughout the follow-up, the patient manifested inflammatory response syndrome characterized by fever, leukocytosis, and tachycardia. No infectious focus was identified and the patient's urine and blood culture tested negative. Due to the poor prognosis, palliative radiotherapy and escalated intravenous analgesia were initiated without clinical improvement. Finally, the patient presented refractory hypoxemia resulting in cardiac arrest and death.
Case 2
A 41-year-old woman presented to the emergency room with 1 month-long right upper quadrant abdominal pain associated with chills, nausea and emesis. Physical examination showed tachycardia and hepatomegaly with tenderness on palpation, and the remainder of the examination was normal. Laboratory studies showed normal levels of complete blood count and liver function parameters. Alpha-fetoprotein was within normal levels. An abdominal computed tomography showed a 20×16 cm-sized cystic lesion in the right hepatic lobule, with multiple septae and hypervascularization. Doppler ultrasound confirmed the finding and showed compression of intrahepatic vascular structures including portal vein (Fig. 2).
The patient underwent extended right hepatectomy without complications. Histopathological study reported high-grade undifferentiated embryonal sarcoma with negative margins and without lymphovascular and perineural invasion, or gangliona metastasis. The patient was discharged without pain and remained stable for two years, when a cystic lesion on the surgical site was documented during the follow-up. The lesion was located close to one of the main branches of the portal vein, and contraindicated for surgical resection.
Due to disease recurrence, chemotherapy with doxorubicin and isophosphamide was scheduled; however, only three cycles were administered due to hematological toxicity manifesting as neutropenia and fever. The lesion remained stable until three years when an increase in size and appearance of new lesions suggesting disease progression were observed (Fig. 3). After five years from the initial diagnosis, the patient was scheduled to receive chemotherapy with gemcitabine and docetaxel.
DISCUSSION
Patients with UESL usually present with an abdominal mass and abdominal pain, associated with anorexia, lethargy, and weight loss. Other symptoms may include nausea, vomiting, constipation, and respiratory distress secondary to compression caused by the tumor.5 Spontaneous rupture of the neoplasm has also been documented.6 Liver test results and neoplastic markers are usually normal. In patients with associated hemorrhage and necrosis inside the tumor, fever and increased levels of systemic inflammatory markers including C reactive protein, erythrocyte sedimentation rate, and leukocytosis, may be present.7
Liver tumors originate in hepatocytes, bile duct epithelium, neuroendocrine cells, and/or mesenchymal cells, which include fibroblasts, endothelium, adipocytes, myoblasts and chondroblasts.8 Macroscopically, UESL are single and well-circumscribed lesions with both cystic and solid components of gray-white gelatinous appearance and a fibrous pseudocapsule formed by compressed liver parenchyma. Frequently, dark-brown areas of hemorrhage and yellow-softer areas of necrosis are found.69 Microscopically, UESL shows undifferentiated spindle cells with ill-defined borders, inconspicuous nucleoli, hyperchromatic nuclei, and eosinophilic cytoplasm surrounded by a myxoid matrix showing undifferentiated and highly proliferative phenotype. Multinucleated giant cells and focal periodic acid Schiff-positive cytoplasmic inclusions resistant to diastase digestion were observed. Several mitotic figures are present as well.110 Immunohistochemically, UESL does not show a specific pattern. It may express histiocytic, muscle and epithelial markers, commonly vimentin and α1-antitrypsin, suggesting origin in primitive stem cells.1112 Ultrastructural studies under electron microscope of UESL revealed fibroblastic or fibrohistiocytic differentiation with rough endoplasmic reticulum cisternae and prominent electron-dense lysosomes and actin filaments in the cytoplasm.13 Lauwers et al.14 demonstrated a common cytogenetic alteration on chromosome 19 in a UESL arising from a mesenchymal hamartomas (MH), suggesting a connection between the two entities similar to UESL representing a malignant progression from MH.
Radiographically, UESL presents as a large solitary tumor with cystic appearance due to its high-water content in the myxoid stroma that may lead to a mistaken diagnosis of benign cystic lesion. Computed tomography (CT) shows a well-defined, low intensity, heterogeneous, multilocular, cystic tumor with gross septa, characterized by an enhancing solid compartment and a non-enhancing cystic compartment.15 Tumors with a solid compartment are usually accompanied by hemorrhage and necrosis that is clearly evident on ultrasound, displaying a honeycomb appearance.16 The presence of discordant imaging findings of solid lesion on ultrasound and cystic lesion on CT are suggestive of UESL. Magnetic resonance imaging (MRI) reveals a well circumscribed hypodense lesion with multiple hyperdense septations and water attenuation. Solid lesions commonly show contrast enhancement although mild and heterogeneous peripheral enhancement secondary to central necrosis and hemorrhage may be observed. Cystic lesions show low signal intensity on T1-weighted MRI and high signal intensity on T2-weighted images suggesting water content. Furthermore, areas with high signal intensity on T1-weighted images and low signal intensity on T2-weighted images suggest hemorrhage.1718
Surgical resection and chemotherapy are the primary treatment modalities for UESL, and chemotherapy is based on a combination of vincristine, actinomycin, ifosfamide and doxorubicin.19 In the absence of complete tumor resection at the time of diagnosis, definitive surgery may be indicated after neoadjuvant chemotherapy. The current 1-year and 2-year survival rates in patients with UESL are 61% and 55%, respectively, with a median survival of 29 months. However, recurrence is a common scenario reported in 32% of the cases with complete resection and adjuvant chemotherapy after a median follow-up of 28 months.20


 XML Download
XML Download