

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Roflumilast is the only approved oral phosphodiesterase-4 (PDE4) inhibitor for the treatment of severe chronic obstructive pulmonary disease (COPD) patients with chronic bronchitis and a history of frequent exacerbations1. A dose of 500 µg roflumilast once daily has demonstrated modest improvements in lung function and reduced the frequency of exacerbations in patients with COPD23456789. However, roflumilast has also shown significant adverse effects (AEs), primarily gastrointestinal problems10. Previous clinical trials showed a relatively low incidence of AEs234. However, the AEs of roflumilast are commonly observed in clinical practice111213. In this study, we examined the AE incidence of roflumilast in a real-world setting and compared the incidence of AEs and the discontinuation rate between patients receiving 250 µg and 500 µg of roflumilast.
Materials and methods
1. Study population
All outpatients diagnosed with COPD at Seoul St. Mary's Hospital between May 2011 and September 2016 were identified, and a retrospective review of their medical records was conducted. Roflumilast was prescribed to patients in doses of 500 µg and 250 µg. The study population comprised adults aged 40 years or older with a history of COPD as defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria. This study was approved by the Institutional Review Board of Seoul St. Mary's Hospital (KC17RESI0294). The requirement for written informed consent from each patient was waived due to the retrospective nature of the study.
2. Clinical measurements
Demographic information including sex, age, and body mass index (BMI), smoking history, prescribed dose of roflumilast, pulmonary function test (PFT), adverse events and frequency of severe exacerbation were collected by retrospective review of medical records. PFTs were performed for all patients by experienced technicians. During the lung function test, multiple forced expiratory efforts were performed to meet American Thoracic Society acceptability criteria14. For data regarding exacerbation, only severe exacerbation was recorded due to the potential for underdetection of mild or moderate exacerbation based on chart review. Severe exacerbation was defined as a worsening of any respiratory symptoms or increased dyspnea, which required an emergency room visit or hospitalization with prescription of systemic corticosteroid and/or antibiotics. To assess the effectiveness of roflumilast, frequency of severe exacerbation in patients who received roflumilast more than 1 year were checked during 12 months from the initial prescription.
3. Statistical analysis
Data are expressed as frequencies with percentages or as means with standard deviation (SDs). Differences between groups were assessed using the chi-square test for categorical variables and Student's t test for continuous variables. The proportion of patients continuing with roflumilast was compared between the groups using the log-rank test. Cox's regression was used to identify variables associated with the discontinuation of roflumilast. Statistical analysis was performed using the SPSS statistical package version 24.0 (IBM Corp., Armonk, NY, USA); a p-value of <0.05 was considered statistically significant.
Results
1. Baseline characteristics
A total of 287 patients were prescribed roflumilast in our hospital during the study period. Of these, 18 patients who were incompatible with COPD according to their spirometry results were excluded. Finally, 269 COPD patients were included in the study. Among them, 178 patients were treated with 500 µg roflumilast once daily and 91 patients were treated with 250 µg once daily (Figure 1).
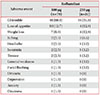
Baseline characteristics of the study population are shown in Table 1. The mean patient age (mean±SD) was 72.5±9.4 years, and 93.7% of the patients were male. The mean post-bronchodilator (pBD) forced expiratory volume in 1 second (FEV1, % predicted) was 42.50±15.34% in 500 µg roflumilast treatment group and 45.74±15.47% in 250 µg roflumilast treatment group (p=0.130) and pBD FEV1/forced vital capacity was 40.22±10.46 and 43.14±13.28, respectively (p=0.069). Overall, the demographics and baseline characteristics were similar between the groups, with the exception of age. Patients in the 250 µg roflumilast treatment group were older compared with the 500 µg roflumilast treatment group (p=0.017).
2. Incidence of AEs
During the study period, a higher percentage of patients in the 500 µg roflumilast treatment group reported AE than those in the 250 µg roflumilast treatment group. The incidence of AEs was 38.2% in the 500 µg treatment group and 25.3% in the 250 µg treatment group (p=0.034) (Figure 2A). One hundred and seventeen AEs were occurred, and 16 patients experienced more than two AEs, 10 patients in 500 µg treatment group, and 6 patients in 250 µg treatment group. The most common AEs were gastrointestinal symptoms including nausea, vomiting, and diarrhea (48 cases in the 500 µg treatment group and 16 cases in the 250 µg treatment group) (Table 2). The next most common AEs were loss of appetite (10 cases vs. 4 cases), headache (2 cases vs. 1 case), insomnia (2 cases vs. 1 case), and tremor (2 cases vs. 1 case) in the 500 µg treatment group and 250 µg treatment group, respectively (Table 2). No patients died during the study period.
3. Discontinuation rate
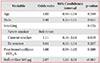
Roflumilast was discontinued due to AEs in 74 patients (41.6%) in the 500 µg treatment group and 21 patients (23.1%) in the 250 µg treatment group. The discontinuation rate differed significantly between the two groups (p=0.003) (Figure 2B). The mean duration of roflumilast use was 344.5±397.8 days (mean±SD). The proportion of patients continuing with roflumilast was analyzed between the two groups using the log-rank test (Figure 3A). There was a significant difference in the proportion of patients continuing with roflumilast (p=0.003). The survival rate for the continuation of roflumilast was lower in the 500 µg treatment group compared with the 250 µg treatment group. Cox's regression was performed to find significant factors associated with the discontinuation of roflumilast. When adjusted by age, sex, smoking status, and lung function, a dose of 500 µg was significantly associated with the discontinuation of roflumilast (odds ratio [OR], 2.87; p<0.001) (Table 3, Figure 3B).
4. Effectiveness of roflumilast
During the study period, 96 patients maintained roflumilast for more than 1 year, 61 patients in 500 µg treatment group and 35 patients in 250 µg treatment group. The mean duration of roflumilast use in these patients was 834.64±308.35 days (mean±SD). Eleven patients (18.1%) in 500 µg treatment group and five patients (14.3%) in 250 µg treatment group experienced at least one severe exacerbation. There was no significant difference between the two groups (p=0.635) (Figure 2C).
Discussion
COPD is a common, preventable, and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases15. Chronic inflammation causes structural changes, narrowing of the small airways, and destruction of the lung parenchyma that leads to the loss of alveolar attachments to the small airways and decreases lung elastic recoil15. A loss of the small airways may also contribute to airflow limitation; mucociliary dysfunction is a characteristic feature of the disease15. Roflumilast is the only approved oral PDE4 inhibitor for the treatment of severe chronic COPD patients with chronic bronchitis and a history of frequent exacerbations1. The principal action of PDE4 inhibitors is to reduce inflammation by inhibiting the breakdown of intracellular cyclic adenosine monophosphate16. A dose of 500 µg roflumilast once daily has demonstrated modest improvements in lung function and reduced the frequency of exacerbations in patients with COPD2345679.
However, compared with placebos, roflumilast significantly increases the incidence of adverse events. Calverley et al.4 studied a worldwide population and showed that the incidence of adverse drug reactions (ADRs) was 67.6% in the roflumilast group and 62.0% in the placebo group (OR, 1.28; 95% confidence interval [CI], 1.11–1.49), while Zheng et al.9 conducted their study in an Asian population (including China, Hong Kong, and Singapore) and showed that the incidence of ADR was 20.3% in the roflumilast group and 5.8% in the placebo group (OR, 4.15; 95% CI, 2.40–7.19). In more detail, the worldwide randomized clinical trial showed that the study population's mean BMI broken down into roflumilast and placebo groups was 26.4±5.5 and 26.0±5.5, respectively, while the Asian randomized clinical trial showed that the study population's BMI in each group was 21.8±3.4 and 22.4±3.4, respectively. Based on these results, the two studies have significantly different BMIs. The odds ratios of the incidence of ADR in the worldwide randomized clinical trial and the Asian randomized clinical trial were 1.28 (95% CI, 1.11–1.49) and 4.15 (95% CI, 2.40–7.19), respectively. This reflects the fact that the incidence of AEs was relatively high in Asian groups with a relatively lower BMI. Moreover, a previous study reported that pBD FEV1 at the end of treatment significantly improved with 250 µg roflumilast (by 74±18 mL [±SD]) and 500 µg roflumilast (by 97±18 mL) compared with the placebo (p<0.001). In addition, the improvement in health-related quality of life was greater with 250 µg roflumilast (−3.4±0.6 units) and 500 µg roflumilast (−3.5±0.6 units) compared with placebo (−1.8±0.8 units)2. A lower roflumilast dose (250 µg) was generally associated with fewer AEs than the higher dose17. Considering these results, a pulmonary specialist in our hospital prescribed two doses of roflumilast depending on the patient's condition. Therefore, we were able to compare the incidence of AEs in a group of patients who received both 500 µg and 250 µg of roflumilast. To our knowledge, this is the first roflumilast study to compare doses of 250 µg and 500 µg in real-world practice. In this study, the incidence of AEs was significantly higher in the 500 µg roflumilast group compared to the 250 µg roflumilast group. The most common AEs in this study were gastrointestinal troubles including diarrhea, nausea, and vomiting, while the next most common AE was loss of appetite. Our results are compatible with those of previous studies.
In our study, we showed that the discontinuation rate in the 250 µg roflumilast group was lower than the rate in the 500 µg roflumilast group. Roflumilast was better tolerated in patients who received 250 µg compared with patients who received 500 µg. The frequency of AEs leading to discontinuation in our study was greater than those reported in several randomized clinical trials235. This could be explained chiefly by the considerable differences in baseline characteristics and comorbidities of real-world patients compared to those included in clinical trials.
This study had several limitations. First, most patients (93.7%) in this study were male. The high rate of male in COPD is due to extremely low rate of smoking in female. There are two large COPD cohorts study in Korea, one is Korea Obstructive Lung Disease (KOLD) cohort and the other is Korea COPD Subgroup Study team (KOCOSS). These two cohorts are multicenter observation study that includes more than 600 and 2,000 patients who were enrolled from tertiary and university affiliated hospitals. Participants in these two cohorts were mainly male, 91% in KOLD18 and 91.2% in KOCOSS19. Therefore, the ratio of our study to male is not different, and it is similar to real-world data. Second, given its retrospective observation design, clinical parameters such as dyspnea, exercise capacity, and quality of life as subjective indicators of efficacy were not adequately reviewed. Third, the sample size may not be sufficiently large to compare effectiveness on exacerbation between the 500 µg group and the 250 µg group. Finally, this was a single-center study.
In conclusion, treatment with 250 µg roflumilast leads to a lower incidence of AEs and discontinuation than treatment with 500 µg roflumilast. Also, there was no significant difference in percentage of patients who experienced severe exacerbation between 250 µg and 500 µg groups. Further studies regarding the optimal dose of roflumilast are required.




 XML Download
XML Download