

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The development and use of injectable fillers began with the invention of the syringe in the late 19th century.1 Since then, many cosmetic fillers have been developed and used for soft tissue augmentation.2 When a dermal filler is injected into the subcutaneous tissue, it can cause a foreign-body reaction, which leads to collagen aggregation around the filler, smoothing out wrinkles on the skin above.3 Facial rejuvenation using filler is a noninvasive procedure that is becoming increasingly common, regardless of age or gender, leading to the possibility that dental images may also contain findings corresponding to filler.4
Although plain radiography has been used in clinical practice for decades, the use of cone-beam computed tomography (CBCT), which provides high-quality, high-resolution images and a 3-dimensional evaluation in a relatively short period of time, is becoming more common.5 CBCT provides definitive images of radiopaque materials such as bone, hard tissue, or calcified deposits, contributing to improved diagnostic capabilities.5
This report describes the radiographic appearance of dermal fillers on panoramic and CBCT images in 3 women who had a history of soft tissue augmentation.
Case Report
Case 1
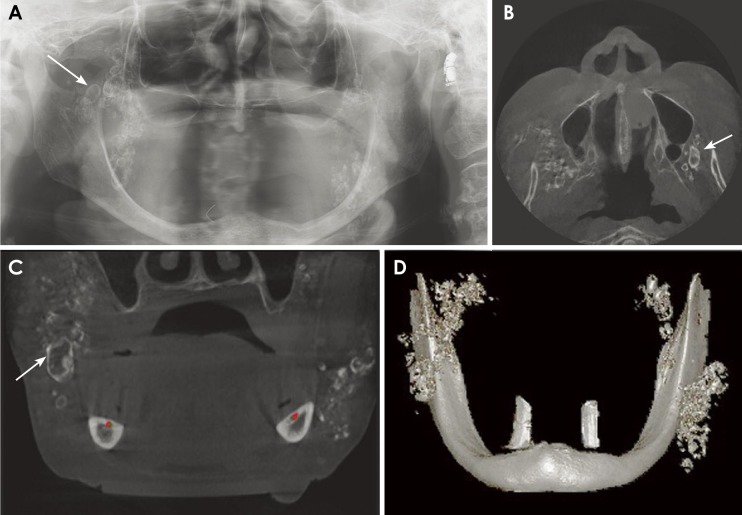
An 88-year-old woman was referred for removal of flabby tissue and implant placement to the Department of Oral and Maxillofacial Surgery of Kyungpook National University Dental Hospital. She was completely edentulous and her physical examination yielded no abnormal findings except for the presence of loose tissue in the anterior maxillary region. A panoramic radiograph (Orthopantomograph OP-100D, Instrumentarium Imaging, Tuusula, Finland) revealed a cluster of multiple discrete radiopacities in the bilateral cheek regions (Fig. 1A). Considering the imaging findings and the location of calcifications, we inquired whether the patient had undergone a dermal filler procedure. Approximately 40 years ago, the patient was treated twice with subdermal injections of filler into both cheeks and zygomatic areas, but the nature of the material used for cosmetic augmentation was unknown. She had no symptoms related to the calcification. CBCT images were acquired with a Pax-Flex 3D apparatus (Vatech, Seoul, Korea), using a 120-×85-mm field of view at 90 kVp and 10 mA for implant placement. The CBCT images demonstrated multiple calcifications in the soft tissue of the cheeks and retromaxillary spaces bilaterally (Figs. 1B–D). A few of the opacities were larger than 11 mm in diameter, and were surrounded by a thin radiopaque rim (Fig. 1C, arrow). The calcified lesions were distinct from the adjacent bony structures, and the surrounding soft tissues appeared intact. Based on all available information, the calcifications were concluded to be the consequence of either the long-standing presence of the cosmetic filler itself or as a secondary reaction to the filler.
Case 2
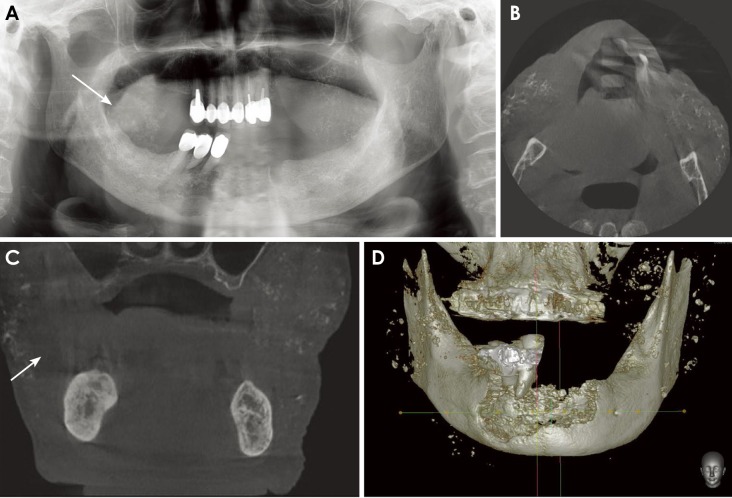
A 91-year-old woman was referred for osteomyelitis of the anterior mandible to the Department of Oral and Maxillofacial Surgery, Kyungpook National University Dental Hospital. Her physical examination revealed a purulent discharge with exposed necrotic bone in the anterior mandibular region. A panoramic radiograph taken with an Orthopantomograph OP-100D apparatus revealed ill-defined, osteolytic bony changes with internal radiopacities and surrounding sclerosis in the anterior mandibular area. Apart from this, small multiple radiopacities were observed in both cheeks and on the right side of the chin (Fig. 2A). When questioned, the patient gave a history of injection of some cosmetic material twice into both cheeks approximately 70 years ago. It was an unauthorized procedure and she could not recall the exact type of cosmetic material used. CBCT images were acquired with Pax-Flex 3D using the same parameters as described above, and showed multiple large calcifications in the soft tissue of retromaxillary space, both cheeks, and the right chin area (Figs. 2B–D). The calcifications were separate from the adjacent bony structures, and the surrounding soft tissues appeared normal. The multiple radiopacities were diagnosed as filler-induced radiopacities based on the imaging findings and history; the patient subsequently underwent surgical treatment for the anterior mandibular osteomyelitic lesion.
Case 3
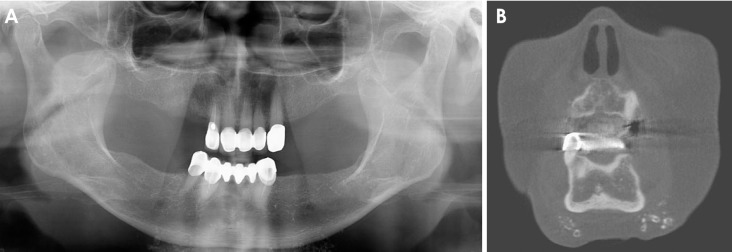
A 77-year-old woman was referred to the Department of Oral and Maxillofacial Surgery, Kyungpook National University Dental Hospital for delayed healing of the extraction sockets of her right maxillary premolars. The patient reported pain in the extraction socket area and physical examination showed bone exposure and purulent discharge around the sockets. Her medical history included rheumatoid arthritis, and she had been on bisphosphonate therapy for the last 5 years. A panoramic radiograph revealed recent extraction sockets in the right maxillary premolar area (Fig. 3A). In the chin area, a cluster of small multiple radiopacities was noted in the soft tissue. Upon enquiry, the patient gave a history of subdermal filler injection into the chin area at an unlicensed center approximately 40 years ago. CBCT images acquired with a CB MercuRay apparatus (Hitachi Medical Systems, Tokyo, Japan), using a 190-×190-mm field of view at 120 kVp and 15 mA demonstrated multiple nodular or ring-shaped radiopacities in the soft tissue of the chin area (Fig. 3B). The masses were distinct from the adjacent bony structures, and the surrounding soft tissue appeared healthy. Considering her history and the clinical and radiographic information, it was concluded that the symmetrical calcification was due to the implantation of a cosmetic filler.
Discussion
This report presents 3 cases in which dermal filler manifested as multiple bilateral calcified lesions in the soft tissue of the facial area. Recently, with increasing interest in maintaining a youthful appearance, there has been an increase in the number of people undergoing face-lift procedures, including those undergoing dermal filler implantation, in clinics, at plastic surgery and dermatology centers, and even at non-hospital facilities. Prior to 1980, paraffin wax and liquid silicone were widely used as esthetic soft-tissue augmentation substances, before questions about the biocompatibility of these materials arose.2 However, the severe side effects associated with these filler materials led to discontinuation of their use.2 A variety of absorbable (collagen, hyaluronic acid, calcium hydroxyapatite, poly-L-lactic acid) and non-absorbable (polymethylmethacrylate beads) materials have been developed since collagen was first approved in 1981 by the FDA for use as a cosmetic filler.267
To date, 3 cases have been reported in the maxillofacial radiology literature regarding facial fillers observed on plain radiographs;8910 2 of these reports included CBCT or CT images.910 The mineralized filler material was clearly observed on plain X-ray and CT images and no discomfort was observed at the filler injection site. Although the patients had a history of filler injection, they did not mention it until a specific question was asked.
The patients in this report were all elderly women who had a history of facial rejuvenation a minimum of 4 decades ago. They had bilateral calcified lesions, distinct from the surrounding bone and at the level of the deep dermis on CBCT images, consistent with the filler administration sites described by the patients. Although no histologic examination was performed, the radiopacities were determined to be related to the fillers based on the imaging characteristics and patient history.10
The patients of case 1 and case 2 underwent soft tissue augmentation twice, so the mineralized particles were observed in a broader area, with various densities and in varying shapes. The difference in density in the image might depend on the composition of the filler10 or the period elapsed since injection, because the radiodensity of filler decreases with time.11 Case 3 showed filler only in the chin area, highlighting the point that filler can be present at diverse regions in the image, according to the administration site. Therefore, depending on the composition of the filler, the timing of the procedure, and the injection site, filler can be detected at any site with diverse radiopacities and shapes on panoramic and CBCT images.12
Current cosmetic fillers are safe,712 but they can cause short-term and/or long-term side effects.1213 Short-term complications include immediate hypersensitivity reactions, over-injection, necrosis, and change in skin color at the injection site.1213 Long-term adverse effects include delayed hypersensitivity, infection, filler migration, scarring, and foreign-body granuloma formation.61213 In addition, the artificially synthesized filler itself promotes a calcification reaction and contributes to the observation of opacities with amorphous or specific shapes on imaging.8 Further, foreign-body granulomas are an important cause of secondary calcification, presenting as ring-shaped calcifications, as seen in case 1.4
When multiple radiopacities are incidentally encountered as part of a routine radiographic examination in the facial region, phlebolith, miliary osteoma cutis, myositis ossificans, dermal fillers, and iatrogenic implant material should be considered in the differential diagnosis.810 Filler-related radiopacities can be diagnosed by their symmetrical location, the absence of associated symptoms, a positive history of esthetic soft tissue augmentation, and the absence of pathological findings associated with systemic disease.8910
In conclusion, dental practitioners should be familiar with the radiographic appearance of dermal filler and should be able to distinguish it from true pathology when multiple bilateral dermal calcifications are observed on panoramic or CBCT images.
 XML Download
XML Download