

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
For early scientific studies of mummies, as they were performed in Europe starting in the 17th century,1 the wrappings of the mummies had to be removed. The examination of their dentition remained limited to a visual inspection through the occasionally opened lips. This consequently led to misjudgments, as in the case of Ramses II. His teeth “are clean and in an excellent state of preservation: they were only slightly worn”, Smith stated in his description of the mummy unwrapped in 1886.2 A later radiographic investigation by Harris corrected this statement: “Ramesses II was in every sense a true dental cripple, suffering from extreme wear of his teeth […], extreme periodontitis […] periapical abscess”.3 The use of radiography for the non-invasive examination of mummies and their dentition then became widely used as a new method of investigation.45 Nonetheless, Moodie, in the first systematic radiographic analysis of a major collection of mummies,6 commented that the identification of caries involved “numerous difficulties, especially the intervention of many different objects producing obscurity of the teeth.”.7 The issue of superposition in planar X-ray imaging was only solved with the introduction of X-ray computed tomography (CT). This imaging modality, with its multiple post-processing capabilities, is considered somewhat of a gold standard in mummy research,8 and CT scans do indeed allow a detailed examination of dental pathologies.9 The possibilities and indications for conventional radiography, however, should not be overlooked.10 Under field conditions outside of the clinical setting, the chemical processing and development of analog X-ray films are especially difficult. The use of Polaroid film for such purposes remained an experiment.11 In this setting, digital conventional X-ray systems offer significant advantages. However, in any form of conventional radiography, the 3-dimensional structures of the skull base and the dentition are projected onto a 2-dimensional image. The resulting superposition of multiple structures on radiographs is known as anatomical noise.12 Different types of projections can be used to avoid or at least to minimize such superposition artifacts, but they require proper positioning of the head.13 When wrapped mummies are examined, especially within their coffins, the orientation of the head may be inconvenient, and compensatory adjustment of the incident angle of the X-ray beam is often limited by the thickness of the coffin walls and the position of the mummy. Furthermore, positioning of the detector plate and the X-ray source can become challenging when space in storage depots is limited. In many cases, superposition of anatomical structures therefore cannot be completely avoided and even the tube-shift technique remains of limited use.13 As a consequence, the interpretation of pathological changes of the dentition or the skeletal system in conventional radiographs of wrapped mummies remains challenging, and even the determination of laterality–that is, distinguishing between the left and right side of the dentition–is not always straightforward. CT scans allowing for later 2-dimensional multiplanar and curved multiplanar reformatting, as well as 3-dimensional volume rendering, can remedy such difficulties.14 However, for this purpose the specimens need to be transported to a facility where a CT scanner is located, at the risk of damaging fragile specimens and generating substantial costs.15 Portable digital X-ray equipment, in contrast, can be used on site and has proven its robustness under harsh conditions–heat, cold, dust, etc.–where the chemical processing of conventional X-ray film would be difficult and time-consuming.16 Furthermore, digital X-ray detector plates provide an excellent spatial resolution perfectly suited for the examination of oral and maxillofacial structures.17 Another advantage of digital X-ray systems is the almost immediate availability of images. This is especially useful under the above-discussed conditions, where it is often necessary to repeat a shot. An unknown position of the head within a coffin, amulets and jewelry obscuring an area of interest, superposition of anatomical structures, and the unknown densities of coffin walls, cartonnages, and their painted surfaces sometimes require repeated adjustments of imaging parameters (voltage and tube current). This can only be accomplished with a system that performs with minimal time consumption and cost.
In this article, the advantages and limitations of different approaches and projections are discussed for planar oral and maxillofacial radiography using portable digital X-ray equipment during archaeological excavations. Furthermore, based on our own experiences supporting anthropological investigations in the Valley of the Kings in Egypt, recommendations are provided regarding projections and sample positioning for examining the dentition of dry skulls and mummies.
Go to : 
Materials and Methods
Equipment
All radiographs were acquired using portable digital planar X-ray equipment, including an X-ray generator (Examion PX 60 HF, voltage range, 40–100 kV; exposure range, 0.4–100 mAs; weight, 14.6 kg; Examion GmbH, Fellbach, Germany), a flat panel detector (Examion DR 1417-600 WL; scintillator, gadolinium oxysulfide; active area, 358×430 mm (14 inches×17 inches); pixel matrix, 3072×2560 pixels; pixel pitch, 140 µm; gray scale, 14 bit; weight, 3.1 kg; Examion GmbH, Fellbach, Germany), a dental detector (Carestream RVG6500 DR-Sensor G2; active area, 27×36 mm; pixel matrix, 1440×1920 pixels; spatial resolution, 20 LP/mm; Carestream Health Inc., Rochester, NY, USA) and dedicated post-processing software (Examion AQS, Examion GmbH, Fellbach, Germany) running on a laptop computer (HP Elitebook 840 G3, LT4120 Snapdragon X5 LTE; HP Inc., Palo Alto, CA, USA) with Microsoft Windows 7 Enterprise Edition (Microsoft Corporation, Redmond, WA, USA) as the operating system.
Samples
The dentition of ancient Egyptian skulls and mummies was examined under field conditions, supporting the anthropological analysis of these human remains during excavations led by the University of Basel in the Valley of the Kings. The Valley of the Kings Project of the University of Basel started in 2009. Subsequently, in 2010, research in tomb KV 31 was initiated, where the remains of 4 mummies, assigned to the mid-18th dynasty, were found. In the same year work began in tomb KV 40, where the first anthropological field season started in 2014, with ongoing research to this day. So far, the human remains of more than 80 individuals dating from the 18th dynasty and from the tombs' reuse during the 22nd dynasty have been found, however most are severely damaged and scattered by looting and fire. Tomb KV 64 was discovered in 2012, containing the mummy of the original tomb owner from the 18th dynasty, as well as the mummy of Nehemesbastet from the 22nd dynasty. The specimens included in this study ranged from fully skeletonized, isolated dry skulls to isolated mummy heads with preserved soft tissue, as well as entire mummies with or without preserved wrappings. A total of 55 specimens, including 19 skeletonized mandibles, 14 skeletonized skulls, 18 separate mummified heads, and 4 partially preserved mummies, were subjected to radiographic assessment (in addition to photographic documentation). A frequent indication for X-ray imaging was age determination in children. Many of the excavated specimens, however, such as isolated mandibular fragments, did not need radiological assessment and were not included in this study.
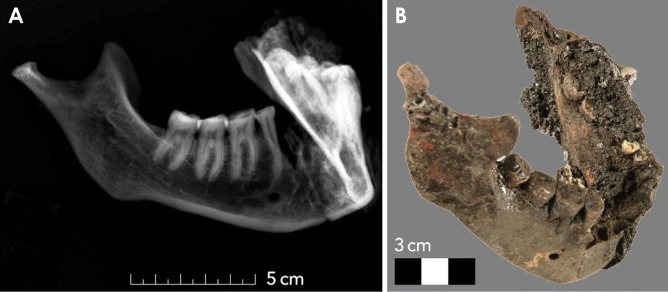
Specimens were divided into the following 4 categories, according to the practicability of various radiographic projections: 1) Partial or complete mummies (4 specimens): The facial skull (upper and lower jaw), including the soft tissues as well as the cranium and the shoulder belt, were at least partly preserved, with consequent limitations for positioning of the detector plate (Fig. 1). 2) Mummified heads (18 specimens): The entire facial skull (upper and lower jaw) including perioral soft tissues was preserved, and possibly also the cranium, with or without soft tissues (Fig. 2). 3) Skeletonized upper jaws (14 specimens): At least the facial skull was preserved, without any perioral soft tissues, including whole skulls (Fig. 3). 4) Skeletonized mandibles (19 specimens): An isolated mandible was preserved (Fig. 4). Frequently, only one-half of the mandible was found, and such half-mandibles could then easily be imaged using a lateral projection.
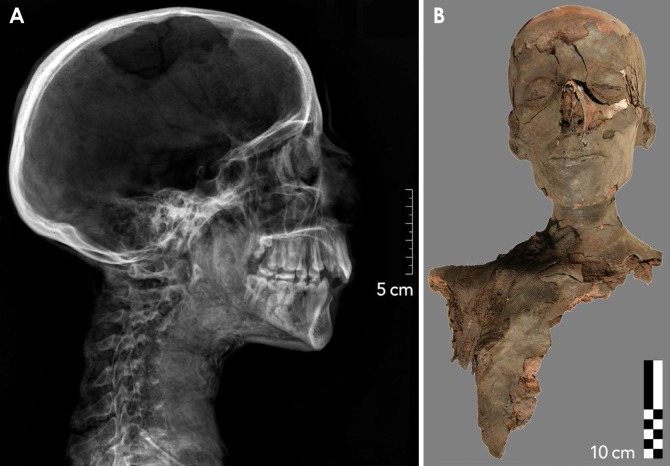 | Fig. 1Example of a partial mummy excavated in tomb KV 40, specimen number KV 40 080. A. Conventional digital radiograph, where the lateral projection provides an excellent overview. B. Correlative photograph, frontal view.
|
 | Fig. 2Example of a mummified head in tomb KV 40, specimen number KV 40 038. A. Conventional digital radiograph, lateral projection. B. Photograph in the frontal view of the same specimen.
|

Projections
All projections, as used for planar oral and maxillofacial radiography with portable digital X-ray equipment during the aforementioned excavations, are listed and explained below. The source-image distance was always set to approximately 120 cm. The properties and indications of specific projections are explained below.
1. For the lateral/cephalometric skull projection, hereafter referred to as the “lateral” projection, the detector plate is placed parallel to the central sagittal plane of the skull, with the central ray's incidence perpendicular to the detector plate, centered about 1 cm above the outer auditory canal. The sella turcica should be projected as a single line. For a tube-shift projection, a second image can be taken with the radiation source displaced in the axial direction.
2. The anteroposterior skull projection provides a good overview of the entire skull. Here the back of the skull is placed against the detector plate, with the central ray's incidence perpendicular to the detector plate and centered on the nasion. The image should be symmetrical and free of any rotation, with both orbital edges looking similar. The petrous ridge should overlap the lower third of the orbits.
3. The axial submentovertex skull projection, hereafter referred to as the “axial” projection, shows the inner temporal bone structures and the skull base in addition to the dentition. For this projection, the vertex of the skull is placed against the detector plate. The infraorbitomeatal line is aligned parallel to the detector plate, with the central ray's incidence perpendicular to the detector plate, centered approximately 4 cm inferior to the mandibular symphysis.
4. For the semi-axial anteroposterior skull projection, hereafter referred to as “semi-axial” projection, the back of the skull is placed against the detector plate with perpendicular alignment of the mento-mandibular line. The central ray's incidence is also perpendicular to the detector plate, centered on the acanthion. In this projection, the petrous ridges should project below the maxillary sinuses. Assessment of coronoid process symmetry will ensure rotation-free alignment.
5. The lateral-oblique mandibular projection is obtained through parallel alignment of the lateral external surface of the mandible and the detector plate. To avoid superimposition of the opposite side of the jaw, the angle of incidence of the central ray should remain perpendicular to the detector plate, centered 2 cm below and 2 cm behind the mandibular angle of the contralateral side (i.e., the side of the X-ray tube).
6. The axial mandibular projection is an axial craniocaudal projection of an isolated mandible. For this projection, the mandible is placed with its inferior borders aligned parallel to the detector plate. The central ray's incidence is perpendicular to the detector plate, centered between both mandibular condyles.
7. “Intraoral” radiography is taken using a dental detector in the parallel periapical projection or in the bisecting-angle periapical projection. Due to its superior spatial resolution, it can provide valuable additional information and is applicable in skeletonized upper and lower jaws.
Evaluation and statistical analysis
All images were evaluated by 2 of the authors with different levels of experience in dental radiography (a board-certified dentist with 30 years of experience (R1=R.S.) and a fifth-year medical resident with extensive radiological and paleoradiological experience (R2=P. E.) with regard to the visibility of diagnostically relevant dental structures using a 4-point grading system (Likert scale): 1, poor visibility (no details, mainly due to superposition, were recognizable); 2, moderate visibility (details of the tooth rows were only partially discernible, or only a part of a tooth row was distinguishable); 3, good visibility (details of the tooth rows and the periodontal tissue were well identifiable); 4, excellent visibility (details of teeth, interdental septa, the periapical region, etc., were clearly visible). Statistical analysis was performed by one of the authors (P.E.) using dedicated software (IBM SPSS Statistics, release 24, IBM Corp., Armonk, NY, USA). Interobserver agreement was assessed by calculating intraclass correlation coefficients (ICCs)1819 based on a mean rating (k=2), a 2-way mixed-effects model, and the “absolute agreement” definition. The following interpretation for the ICCs was used: values less than 0.5 were considered to indicate poor reliability, values between 0.5 and 0.75 indicated moderate reliability, values between 0.75 and 0.9 indicated good reliability, and values greater than 0.90 indicated excellent reliability.
Go to :
Results
Images could be acquired successfully within the expected practical limitations according to our experiences from previous similar expeditions.
Skeletonized skulls comprising the dentition of the upper jaw were mainly radiographed using the lateral, anteroposterior or semi-axial projections, primarily for evaluation of the osseous structures. However, the dentition was only partially assessable with these projections. Lateral projections provided good results in all categories.
The lateral-oblique projection was only applicable for mandibles, while axial projections could be applied for both isolated skulls and mandibles. In addition, the skeletonized upper and lower jaws were accessible for the small, high-resolution dental detector. This procedure was, however, not applicable when perioral soft tissues were preserved, leaving the oral cavity inaccessible. Isolated mummified heads were therefore radiographed using the above-mentioned most common projections as well as the axial projection and the tube-shift technique.
Entire mummies, with the head still attached to the rest of the body, were the most challenging specimens to image. Projections were often difficult to adjust, and several test shots were required to properly achieve the desired projections. Nevertheless, in many situations, not all possible projections were required for optimal diagnostic outcomes. In addition, it must be kept in mind that the investigation of these human remains was also assisted by photographic documentation, without further indication for radiography.
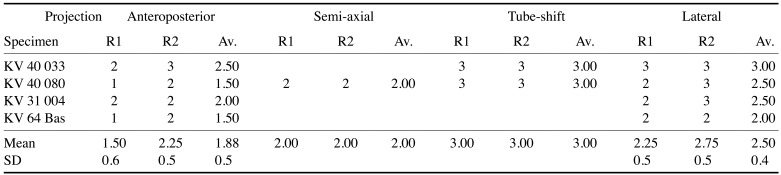
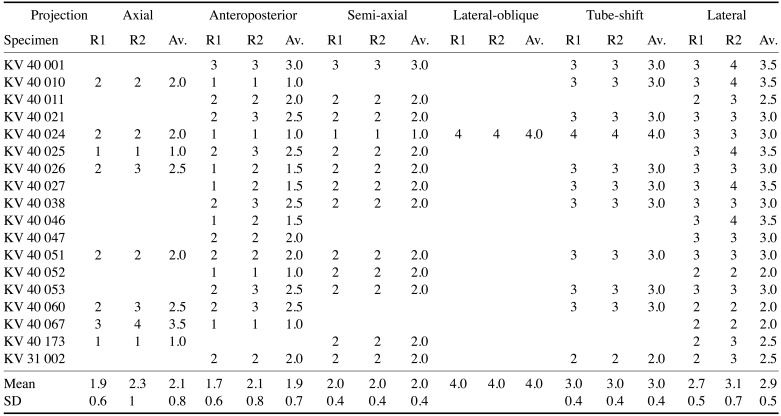
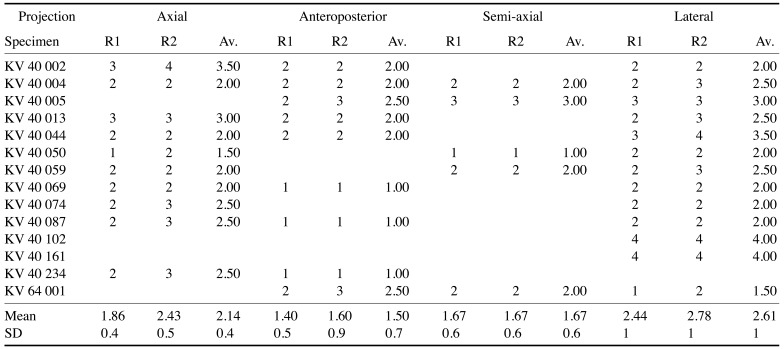
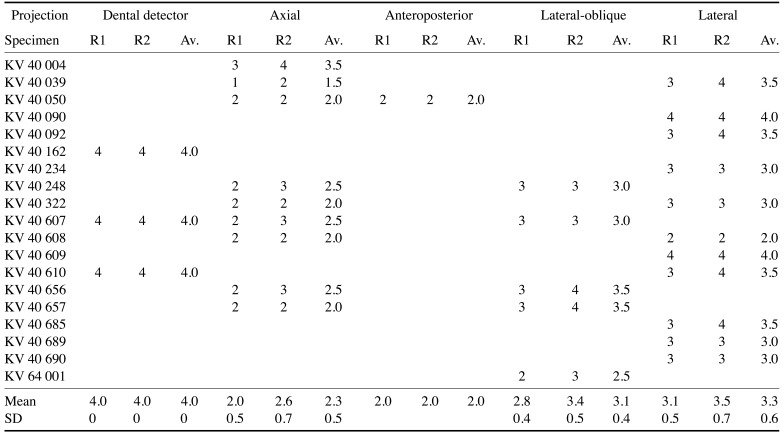
Descriptive statistical data (semi-quantitative data) for both readers (R1 and R2), as well as the mean values of both readers are listed in Tables 1, 2, 3, 4. ICC calculations showed that the 2 readers had good consistency in their ratings of diagnostic image quality, with values of 0.765 for single measures and 0.867 for average measures. Overall, the visibility of diagnostically relevant dental structures was rated highest by both authors on X-ray images acquired using the dental detector (consistent ratings of 4 points on the 4-point Likert scale for the imaged mandibles), the high resolution of which revealed the finest dental and osseous structures, but at the cost of a very small detector size (27×36 mm). Tube-shift projections of the dentition used for the imaging of mummified heads and entire or partial mummies achieved the second-best rating (average over both readers of 3.0±0.4 points on the 4-point Likert scale), with well-identifiable details of tooth rows and periodontal tissues, but with a slightly lower resolution, since a standard-size digital detector was used (358×430 mm). Lateral projections achieved the third-best ratings (average ratings of 2.5±0.4, 2.89±0.5, 2.61±1, and 3.27±0.6 on the 4-point Likert scale) for entire or partial mummies, mummified heads, skeletonized upper jaws, and skeletonized mandibles, respectively, still providing images of acceptable diagnostic quality. Lateral projections were the most used type of projection (in 46 out of 55 specimens).
Go to :
Discussion
This article reflects radiographic fieldwork over a relatively long period of time. According to our experiences, we can give some recommendations to facilitate a practicable workflow in similar conditions:
1. Fully skeletonized skulls can be positioned in almost any desired projection. Therefore, even “intraoral” shots with the dental detector placed on the uncovered dentition of the upper and lower jaw are feasible and useful. In such cases, “intraoral” radiography using a small dental detector follows standard positioning and projections, such as the parallel periapical projection or the bisecting- angle periapical projection.20 However, if soft tissues are missing, dental pathologies, such as occlusal, more extended approximal carious lesions or root caries and alveolar bone loss, can be identified immediately by visual inspection. The indications for X-ray imaging may therefore be more restrictive, for example only if hidden carious lesions or intraosseous bone alterations are suspected. A full set of oral radiographs is not initially required. Axial radiographs, using a larger standard-size X-ray detector, give an overview of the whole dentition, possibly impacted teeth, or the cortices of the upper and lower jaw. An anteriorly or laterally shifted axial projection can provide additional information on the frontal or lateral part of the dentition. In such cases, the skull or the mandible can directly be placed on the detector. In addition, the “extraoral,” lateral-oblique projection of the mandible, again using the larger standard-size X-ray detector, provides a good overview of the posterior teeth and the adjacent osseous structures. Therefore, in case of dry skulls, the specified “intraoral” techniques using the dental detector can be combined with an “extraoral” technique using a larger standard-size X-ray detector.
2. Isolated mummy heads with preserved soft tissue, in contrast, may still be freely positioned, but the intraoral space is no longer accessible due to the completely dried and rigid soft tissues. Therefore, lateral, axial, anteroposterior, semi-axial, and lateral-oblique projections have to be performed. The anteroposterior projection should be favored over the usual posteroanterior projection. This way, the fragile soft tissue structures of the face, including the nose, the lips, the chin, and the skin covering the supraorbital region, are at less risk of being damaged, since the head rests on its occipital region. The distortion resulting from the greater distance to the detector plate seems to be an acceptable trade-off in order to prevent damaging the specimen. Such a set of projections provides a good overview of the skull, the skull base, and the oral and maxillofacial structures. In semi-axial projections, defects of the skull base, often created for excerebration, can be identified and localized in the ethmoid or sphenoid region.20 The superposition of the right and the left tooth row can present a further problem, which can be countered by the tube-shift technique. This technique helps to reduce superposition and allows the laterality of the rows of the dentition to be determined. For this, two additional images, one with a more cranial and one with a more caudal positioning of the X-ray tube, are required. The row of teeth nearer to the detector plate will then move “with” the tube, and in this manner, the right and left sides can be distinguished.
3. In cases of an entire mummy, with its head still attached to the rest of the body, the situation is again different. Most the time the head's position is set and can only be slightly moved or may even not be altered at all. Nevertheless, under such conditions the intended projection of an X-ray image should still be directly verified. If the wrappings of a mummy are still preserved or if the mummy rests in a coffin or a cartonnage, a test shot is recommended to obtain information about the posture and the localization of the head. The positioning of the X-ray tube and the detector plate can then be adjusted for further images of the desired projections.
We would also like to mention some of the limitations of our study. Since some of the discussed projections are only applicable for certain types of specimens, the number of evaluated projections per object was small, which has to be considered in addition to the inherent limitations of semi-quantitative grading systems. In addition, the number and type of radiographs acquired mainly depended on the anthropologists' questions. The main objective therefore was not the production of “clinically correct” images, but to answer questions such as determination of the age at death, which explains some of the qualitative limitations of the resulting X-ray images.
In conclusion, radiographic examination of the dentition and its adjacent structures in the context of archeological excavations is a challenging task. New imaging modalities, such as CT and DVT, have substantially improved diagnostic capabilities in routine clinical practice.21 With some limitations, this also applies to mummy research. However, when investigations have to take place under field conditions, conventional planar digital X-ray imaging, due to its ubiquity, remains an excellent method-and often the only practicable one-for examining the skulls and teeth of ancient Egyptian mummies. Despite challenging field conditions, radiographic images of excellent diagnostic quality can be obtained, if an appropriate methodology regarding the selected projections and sample placement is followed.
Go to :
 XML Download
XML Download