

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Iodine is an essential element of thyroid hormone synthesis, and normal thyroid status is a prerequisite for normal growth and development. Since iodine deficiency during pregnancy can cause serious health problems, both in pregnant women and in their offspring, national salt iodization programs have been implemented, starting in many Western countries, and have improved iodine nutrition worldwide [1].
Furthermore, excessive iodine intake can lead to thyroid dysfunction in susceptible individuals [2]. Excess iodine transiently inhibits thyroid hormone synthesis through decreasing organification by an autoregulatory mechanism known as the acute Wolff-Chaikoff effect [3]. In healthy individuals, the thyroid ‘escapes’ from the acute Wolff-Chaikoff effect via downregulation of the sodium/iodide symporter in thyrocytes, after which normal thyroid hormone synthesis restarts [45]. However, in susceptible individuals (including those with Hashimoto thyroiditis and related genetic syndromes) and neonates (especially in premature infants), failure of this escape mechanism can result in iodine-induced hypothyroidism [5]. The fetal thyroid gland under 36 weeks of gestational age is not mature enough to fully escape from the acute Wolff-Chaikoff effect, so iodine excess can easily cause fetal hypothyroidism, even if maternal thyroid function is preserved [6]. Taken together, excessive dietary iodine intake and/or iodine supplementation during pregnancy may cause adverse effects on maternal and fetal thyroid function, birth outcomes, and offspring growth and development.
According to a recent cross-sectional study of 7,190 Chinese pregnant women during their first trimester in an iodine-sufficient region, the relationship between urinary iodine concentration (UIC) and thyroid function was U-shaped: the prevalence of overt or subclinical hypothyroidism was lowest in the group with a UIC 150 to 249 μg/L, and UICs that exceeded 250 μg/L were associated with an increased risk of subclinical hypothyroidism [7]. Korea is an iodine-replete area [89], and Korean lactating women traditionally consume brown seaweed soup, which contains high levels of iodine, daily during the early postpartum period [1011]. Therefore, offspring exposed to high iodine content in breast milk may be at an additional risk for thyroid dysfunction. Clinical research on the effects of iodine excess in pregnant and lactating women on offspring growth and development is lacking, although such studies would inform current recommendations for safe upper limits on the dietary intake of iodine and/or iodine supplementation.
We designed the Ideal Breast Milk (IBM) cohort, a prospective mother-child pair cohort, to investigate the effects of maternal iodine status during pregnancy and lactation on maternal thyroid function, offspring growth and development, and offspring thyroid function. The specific aims are as follows:
(1) To evaluate dietary iodine intake in pregnant and lactating women and their offspring's iodine exposure status in the neonatal period and infancy.
(2) To investigate the effects of iodine status during pregnancy on maternal thyroid function (gestational and postpartum).
(3) To evaluate the effects of maternal iodine status during pregnancy on the birth outcomes of offspring.
(4) To determine the influence of early-life iodine exposure (prenatal and postnatal) on growth and thyroid function in infancy.
Go to : 
METHODS
Study design
Participant recruitment and inclusion criteria
The IBM cohort recruited 198 pregnant women from a single tertiary center (Seoul National University Hospital, Seoul, Korea) between June 2016 and August 2017.
Participants were included if they met all the following criteria:
(1) Being a pregnant woman in the third trimester (with a paired newborn baby or babies).
(2) Agreeing to participate in the study and signing the consent form (for the pregnant women).
(3) For newborn babies, their legal representative agreeing to participate in the study and signing the consent form.
Participants who met any of the following criteria were excluded:
(1) Having three or more fetuses.
(2) Having a previous history of thyroidectomy.
(3) Currently taking anti-thyroid drugs to treat hyperthyroidism.
(4) In participants with a history of overt hypothyroidism, having taken levothyroxine for more than 12 months and currently taking levothyroxine.
(5) Having any other severe comorbidities.
Sample size
To estimate the sample size, we considered the significance level and statistical power, and we estimated the ratio of the exposed to the unexposed from the results of previous studies [121314]. According to a prospective study of 344 Korean pregnant women during their third trimester conducted among hospital-based participants, we calculated the ratio of the exposed to the unexposed by UIC levels [12]. In that study, the researchers used the World Health Organization (WHO) criteria to classify participants by iodine status based on the median UIC in pregnant women, as in this study. For the offspring's thyroid function, we referred to another prospective cohort study of a Dutch population [13]. Although their classification of UIC levels was different from that used in our study, we could refer to their odds ratios for thyroid function (thyroid stimulating hormone [TSH] levels) in the offspring. In addition, as no adequate study had evaluated associations between mothers' thyroid function and their offspring's thyroid function in a Korean population, we referred to the prevalence reported in a Chinese population-based study [14]. Ultimately, we used 0.5 as the ratio of the exposed to the unexposed, 2.5 as the odds ratio, and 34% as the prevalence, and set a significance level of 95% and statistical power of 80%. We calculated that the required sample size would be 179 mother-child pairs using a 2-sided test in Epi Info (CDC, Atlanta, GA, USA; 2016). Estimating a 10% rate of loss to follow-up, we aimed to recruit 198 mother-child pairs.
Follow-up protocols
Fig. 1 presents the process of the survey. Each maternal participant makes three visits: one during pregnancy (in the third trimester, maternal visit 1), one at 3 to 4 weeks after giving birth (maternal visit 2), and one at 12 to 15 months after delivery (maternal visit 3). For each visit, they complete a 3-day dietary record, and urine and blood are collected on the last day of the dietary record during the visit. The thyroid is evaluated by ultrasonography at visits 1 and 3. A breast milk sample is obtained at visit 2 (Table 1).
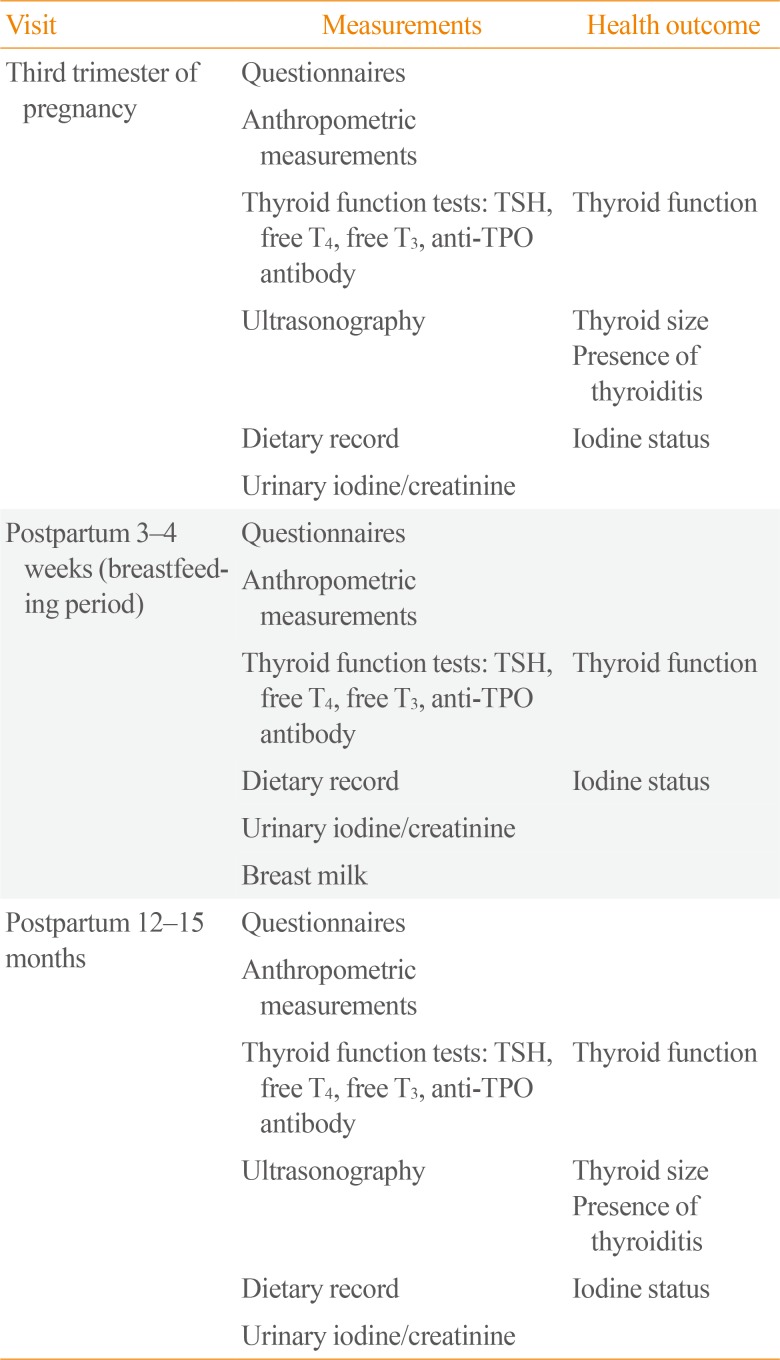
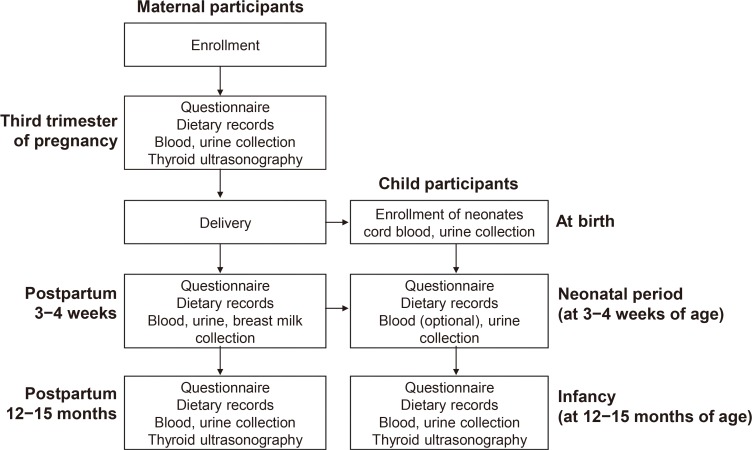
Table 1
Measurements of Maternal Participants
![]()
The child participants are enrolled at birth. A cord blood sample is collected in the delivery room. First-void urine is collected in the nursery after birth. A neonatal screening test is performed at 3 to 7 days of life. Urine samples are also collected at 3 to 4 weeks of age (maternal visit 2) along with the collection of breast milk. When the child is 12 to 15 months old (maternal visit 3), blood sampling for a thyroid function test and thyroid ultrasonography are performed along with an evaluation of growth and development (Table 2).

Table 2
Measurements of Child Participants
![]()
Dietary assessment
To assess the maternal diet during pregnancy and lactation, 3-day dietary records are collected during pregnancy (in the third trimester, visit 1) and at 3 to 4 weeks after delivery (visit 2). The dietary records include 2 weekdays and 1 weekend day. The dietary record booklet is designed to be entirely self-administered, and contains written instructions to help the maternal participants record the relevant details of all foods and beverages consumed, as well as an example of a correctly completed record.
Energy and nutrient intake, except for iodine, are estimated using the nutritional analysis program (CAN-Pro) version 4.0 (Korean Nutrition Society, Seoul, Korea). Iodine intake is calculated using an established database [9]. The iodine values for some food items that newly appeared during the period of this study are imputed using substituted or calculated values based on the rules used to establish the iodine database.
Measurement of iodine concentrations
Iodine concentrations are measured in random urine and breast milk samples using a 7900 ICP-MS apparatus (Agilent Technologies, Santa Clara, CA, USA). Random UICs are adjusted by urinary creatinine. According to the 2007 WHO recommendations [15], pregnant women will be divided into four groups by UIC values: iodine-insufficient (UIC <150 μg/L), adequate (UIC 150 to 249 μg/L), more than adequate (UIC 250 to 499 μg/L), and excessive (UIC ≥500 μg/L).
Statistical analysis
The baseline demographic and clinical characteristics of maternal participants will be identified from a descriptive analysis of questionnaire survey and laboratory results. In the descriptive analysis, the distribution of maternal participants for most measured variables will be stratified by the predefined iodine exposure category. The main exposure in this study is maternal iodine exposure. As outcomes, the baseline demographic and clinical characteristics of the child participants will be identified from a descriptive analysis of neonate profiles, including gestational age, height, weight, head circumference, and UIC. The Kolmogorov-Smirnov test will be performed on continuous variables to determine whether they show a normal distribution. Continuous variables will be expressed as the mean±standard deviation or as the median with an interquartile range, depending on their distribution. Categorical variables will be summarized as the frequency and proportion. The Pearson correlation test will be applied to assess continuous associations between various measurements for data with a normal distribution, and the Spearman correlation test will be used for data that do not show a normal distribution. To address concerns about non-linear relationships, generalized additive models (GAMs) with a smoothing function will also be used. This model can be applied to both linear and non-linear associations, and it provides more comprehensive insights into associations between predictors and response variables than standard modeling techniques. To make a primary measurement of GAM fit, the Akaike information criterion (AIC) will be used; a lower value of the AIC indicates better model fit.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Seoul National University Hospital (IRB No. 1512-039-727 for mothers, 1606-117-772 for children), and all mother-child pair participants provided written informed consent.
Go to :
RESULTS
Maternal participants
A total of 198 pregnant women in their third trimester were recruited. Their demographic characteristics are summarized in Table 3. Their mean age was 35.1±3.5 years, and 78 (39.4%) of them were pregnant with twins. Thirty-three (16.7%) of them had a previous history of thyroid disease. Eleven of those patients had a previous history of hyperthyroidism, of whom nine had previously received an anti-thyroid drug. The other 22 patients in this category had a previous history of hypothyroidism, and 18 of those patients had been diagnosed with subclinical hypothyroidism at a pre-pregnancy check-up and were receiving levothyroxine. Sixty-eight participants (34.3%) had a history of iodinated contrast medium exposure. Eleven of those patients had been exposed to intravenous contrast medium for computed tomography imaging, and 57 had received an intrauterine injection of contrast medium for hysterosalpingography.
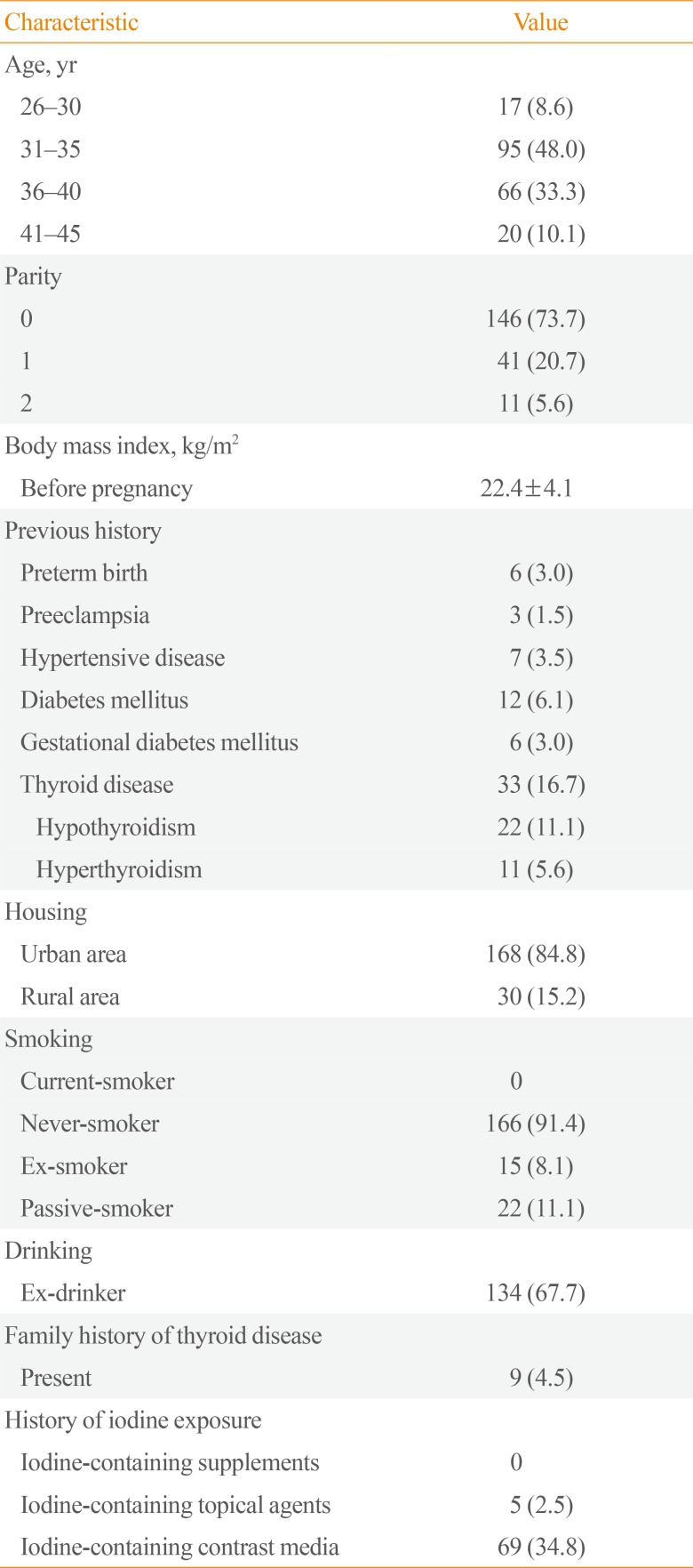
Table 3
Demographic Characteristics of the 198 Pregnant Women Recruited to This Study
![]()
Go to :
DISCUSSION
The optimal and safe ranges of iodine intake during pregnancy and lactation are a matter of concern. Although vulnerable individuals such as preterm infants [12], pregnant and lactating women, and individuals with preexisting thyroid disease are susceptible to adverse outcomes of excess iodine intake and exposure [16], safe upper limits for iodine intake during pregnancy and lactation have not been well defined [17].
A few studies on iodine status in pregnant and lactating women in Korea, an iodine-replete country, have been reported. The median UIC of healthy pregnant women in Korea was 427.3 μg/L [12], which is more than adequate on the basis of the 2007 WHO criteria. Median breast milk iodine levels at the 1st and 3rd weeks postpartum were found to be 2,529 and 1,153 μg/L, respectively [1218], which are higher than those reported in other iodine-abundant countries [1920] and exceed those associated with the upper limit of iodine intake of 1,100 mg/day recommended by the Institute of Medicine [21]. Since the traditional intake of brown seaweed (Undaria pinnatifida) soup was the most likely cause of excessive iodine in Korean lactating women [11], a careful dietary history for thyroid dysfunction-related symptoms was suggested as part of the evaluation and follow-up of postpartum Korean women and their infants [10]. In Chinese women during early pregnancy [7] and late pregnancy [22], it was found that iodine excess may lead to maternal subclinical hypothyroidism. In Norway, an association between breast milk iodine concentrations and thyroid dysfunction was reported in lactating women [23], although neither UIC nor breast milk iodine levels predicted TSH levels among breastfed infants with excess iodine [24]. In preterm Korean infants, excessive iodine intake from breast milk was associated with subclinical hypothyroidism [12]. However, no studies have included a prospective follow-up of iodine status and thyroid function in mother-child pairs from gestation to childhood.
No apparent developmental toxic effects have been reported in humans exposed to excess iodine, although toxic doses of iodine during pregnancy adversely impacted pregnancy and fetal outcomes in mice, with effects including skeletal variation [25]. It remains controversial whether maternal iodine excess adversely affects birth outcomes, anthropometry [2627], and/or neonatal thyroid function [262728]. A single study reported that maternal iodine status and serum TSH levels during early pregnancy had no relationship with child development in infancy [28]. Prospective human studies are needed to investigate whether excess iodine during developmental windows of susceptibility has a long-term effect on growth and development in infancy and childhood and to identify the optimal iodine ranges for preventing adverse outcomes. This study of the IBM cohort is expected to help develop guidelines for optimal and safe iodine nutrition in pregnant and lactating women.
Go to :
 XML Download
XML Download