

 ePub
ePub Citation
Citation Print
Print



INTRODUCTION
One of the most difficult tooth movements in orthodontic treatment is to correct anterior crossbite in skeletal Class III malocclusion patients. Movements of lower anterior teeth in these patients should be carefully monitored in orthodontic camouflage treatment as the mandibular incisors are lingually tipped to achieve positive overjet. This is also considered when preparing patients for orthognathic surgery as the mandibular incisors are labially decompensated during alignment.
Tooth movement occurs via periodontal ligament widening and alveolar bone remodeling.1 Root resorption, alveolar bone loss, fenestration, and gingival recession may occur during tooth movements that exceed the biological limitations of the alveolar bone.2 When considering lower incisor movements, the cortical plates of the alveolar bone or mandibular symphysis near the root apex are anatomical barriers as bone remodeling is limited in this region than in the alveolar crest or midroot region.34 Therefore, detailed three-dimensional (3D) evaluations of the alveolar bone in the lower incisor area would be useful for clinicians even more so when correcting anterior crossbites as there may be greater buccal and lingual tooth movements to monitor.
A previous study comparing skeletal Class I to Class III subjects with normal mandibular plane angles reported relatively thinner mandibular anterior alveolar bone in the mid-root and lingual areas in the Class III group.5 Other studies have also found decreased bone thickness and elongated bone morphology of the mandibular anterior region in individuals with high mandibular plane angles.56 Taking into consideration the findings of the aforementioned studies, it is reasonable to assume that skeletal Class III high angle subjects may have thinner alveolar bone and should be carefully monitored for periodontal health during orthodontic treatment.
To verify these clinical findings, a majority of studies have used two-dimensional (2D) radiographs to measure alveolar bone thickness.5678910 However, alveolar bone measurements on lateral cephalograms may be inaccurate up to almost 1 mm from the actual thickness and may be questionable in terms of their diagnostic value. Thus, a 3D evaluation of alveolar bone thickness of the mandibular incisor area would better illustrate the actual buccal and lingual alveolar bone morphology, which may be directly affected by orthodontic tooth movement and aid in proper treatment planning for clinicians. Therefore, the aim of this study was to evaluate lower anterior alveolar bone thickness at various levels in skeletal Class III malocclusion patients of different vertical facial patterns and to compare the results to those of skeletal Class I patients by using cone-beam computed tomography (CBCT) images.
MATERIALS AND METHODS
This study evaluated CBCT images of adults who had visited the orthodontic department of Gangnam Severance Dental Hospital between January 2011 and July 2015. CBCT images had been acquired for surgical extractions of impacted third molars. All patients were scanned in an upright position in maximal intercuspation by using a CBCT scanner (Pax-Zenith3D; Vatech, Seoul, Korea) with a scan time of 24 seconds, tube voltage of 105 kVp, and voxel size of 0.3 mm. After analyzing cephalograms generated using CBCT images, 29 skeletal Class I (0° < angle between A point-nasion-B point [ANB] < 4°) and 90 Class III subjects (ANB < 0°) were included in this study. The inclusion criteria were less than 3 mm of crowding or 2 mm of spacing in the mandibular anterior teeth and no signs of periodontal disease, such as bleeding on probing, gingival recession, or alveolar bone loss, as determined using clinical and radiographic evaluations. The exclusion criteria were any previous orthodontic treatment, presence of prosthetic treatment involving the mandibular anterior teeth, missing or supernumerary teeth in the mandibular arch, facial asymmetry of greater than 2 mm or dentofacial deformity, presence of short mandibular anterior roots of less than 11 mm, and presence of alveolar bone loss extending 2 mm below the cementoenamel junction (CEJ). Vertical facial patterns were assessed according to the angle formed by the sella-nasion line (SN) and mandibular plane (MP), and skeletal Class III subjects were further divided into three groups: high angle (SN-MP > 38.0°), normal angle (30.0° < SN-MP < 37.0°), and low angle (SN-MP < 28.0°). Skeletal Class I subjects with normal angles (30.0° < SN-MP < 37.0°) were assigned as control group.1112 Demographic data of subjects are shown in Table 1. This study was approved by the Institutional Review Board of Gangnam Severance Hospital (3-2017-0200).
The images were reformatted to be viewed at a width of 1,726 Hounsfield units (HU) and level of 870 HU on a 3D imaging software (OnDemand3D™; Cybermed, Seoul, Korea). Sagittal images were oriented by following the long axis of each mandibular incisor that bisected the pulp chamber and canal in the sagittal and coronal planes. Thereafter, selected images were imported into an image analysis program (Image-Pro Insight; Media Cybernetics, Silver Springs, FL, USA) for measurement. Alveolar bone thickness was measured by drawing a reference line that passed the long axis of each incisor from the incisal edge to the tip of the root followed by the buccal and lingual perpendicular lines to this reference line at the alveolar crest (BT0 and LT0) as well as at 3, 6, and 9 mm apical from the alveolar crest (BT3, BT6, BT9, LT3, LT6, and LT9). Total alveolar bone thickness was also measured (TT0, TT3, TT6, and TT9). The alveolar crest was defined as the 2 mm apical level from the CEJ.1314 Subjects showing extreme variations in alveolar width measurements of over 1 standard deviation from the mean values for the Class I and Class III groups were further excluded from the samples. Measurements used in this study are shown in Figure 1.
All statistical analysis was performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Measurements were performed by one examiner, and five subjects were randomly measured three times for over 6 weeks to test intra-examiner reliability, which showed high reliability (r > 0.9). The average values for alveolar bone thickness were obtained by calculating the average measurements from the right and left incisors. The Shapiro-Wilk test was used to test normal distribution of the variables. Paired t-tests were used to compare statistical differences between the measurements for the central and lateral incisors. A linear mixed model followed by the Bonferroni post-hoc test was used for comparisons between the four groups (control, Class III high angle, Class III normal angle, and Class III low angle). Pearson correlation analysis was used to identify associations between changes in the SN-MP angle and mandibular anterior alveolar bone thickness in skeletal Class III patients. A p-value of less than 0.05 was considered statistically significant.
RESULTS
The mandibular central and lateral incisors did not show significant differences in most measurements except at BT3 in the Class I, Class III normal, and Class III high angle groups as well as at LT3 in the Class III normal angle group (Supplementary Table 1). In order to simplify intergroup comparisons, the average values of the central and lateral incisors were used throughout this study despite the differences in the four regions.
In all groups, buccal and lingual alveolar bone thickness had the smallest value at the alveolar crest and had a tendency to gradually increase as the measurements moved apically from the CEJ to the 9 mm apical level. Buccal and lingual alveolar bone thickness did not show significant differences at the alveolar crest and 3 mm apical level for all groups. However, at the 6 mm and 9 mm apical level, lingual alveolar bone width was significantly greater than that of the buccal side for all groups (Table 2).
The Class III high angle group showed significantly smaller buccal and lingual thickness compared to the Class I group at all levels excluding the buccal alveolar crest and LT9. The Class III high angle group had significantly thinner alveolar bones in all areas compared to that of the Class III low angle and normal angle groups except at BT0, BT3, and LT9. The Class III low angle group showed significantly greater thickness values at BT6 and LT9 compared to the Class III normal angle group. Total alveolar bone thickness was significantly smaller at the alveolar crest and 3 mm apical level with similar trends in the 6 and 9 mm apical level in the Class III high angle group than in the Class I, Class III normal, and Class III low angle groups (Table 3). From the incisor mandibular plane angle (IMPA) adjusted linear mixed model, the Class III high angle group had significantly smaller width measurements at most variables except at the alveolar crest as well as the total alveolar thickness measurement at the 9 mm apical level compared to the Class III normal and low angle groups (Supplementary Table 2).
In the Class III high angle group, 9 openbite and 22 normal overbite subjects were included, and the average overbite was −2.8 ± 1.62 mm in the open bite group and 1.1 ± 0.80 mm in the non-open bite group. No significant difference was observed between the open bite and non-open bite groups in alveolar bone thickness at all levels except for the buccal alveolar bone at the 6 mm apical level between the two groups (data not shown).
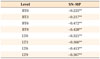
The mandibular plane angle (SN-MP) was negatively correlated with buccal and lingual alveolar bone thickness values. Buccal and lingual alveolar bone at the 6 mm and 9 mm apical levels showed moderate negative correlations (0.4 < r < 0.5) (Table 4).
Supplementary data is available at https://doi.org/10.4041/kjod.2018.48.6.349.
DISCUSSION
CBCT images have been used in previous studies evaluating the alveolar bone in various locations and angulations to provide quantitative evaluations of bone thickness.1516 This study evaluated mandibular anterior alveolar bone thickness of skeletal Class III subjects by using CBCT images that enabled comparisons between the mandibular central and lateral incisors as well as detailed buccal and lingual measurements at various levels of the alveolar bone, which should be considered during tooth movements to overcome anterior crossbite. The Class III subjects were further divided by mandibular plane angles in order to provide detailed classifications of facial dimensions in a vertical direction.
Buccal and lingual alveolar bone thickness at 3 mm apical level was about 0.6 mm and lingual alveolar thickness coronal to the 9 mm apical level was within 1 mm for the Class III high angle group. These measurements were relatively thin compared to those of the Class I, Class III normal, and Class III low angle groups. The findings of this study were consistent with those of previous studies in that mandibular anterior alveolar bone thickness was affected by vertical facial patterns.56717 Although studies using lateral cephalograms showed mandibular alveolar thicknesses that were greater than those measured in this study by an average of 0.32 mm, this could be due to the inaccuracy of width measurements obtained from 2D radiographs, which may be enlarged by almost 50% compared to actual values.18 On the other hand, the mandibular alveolar thickness in this study showed similar values to those reported of human cadavers which is in line with previous studies that report the accuracy of measurements made on CBCT images.19
Several reports have documented detrimental periodontal consequences, such as loss of buccal cortical bone and gingival recession, resulting from orthodontic treatment and extending throughout the retention phase in areas with thin alveolar bone.202122 On the other hand, there have been different views that the amount of labial decompensation in orthodontics is not enough to cause clinical significance.2324 In this study, alveolar bone thickness at the 6 mm and 9 mm apical level was thinner on the buccal side and showed the smallest value in the Class III high angle group which indicates that care must be taken when decompensating mandibular anterior teeth during pre-surgical orthodontics in skeletal Class III high angle patients.25 However, the Class III normal and low angle groups showed similar thickness values compared to Class I control group in most areas which may imply that there is some leeway for different orthodontic treatment strategies in Class III normal and low angle patients. The Class III low, average, and high angle groups did not show significant differences in ANB and Wits appraisal. However, the IMPA was significantly smaller in the high angle group. This is in accordance with previous studies in that subjects with increased mandibular plane angles have long and thin shaped symphysis with extrusion and lingual compensation of mandibular incisors.2627 Considering that the alveolar bone is considerably thinner and the mandibular incisors are even more lingually tipped in the Class III high angle group, monitoring the periodontal health of the mandibular anterior area throughout the retention phase would be necessary.
According to a previous study on adults aged over 20 years, the Class I normal angle patients showed a continuous decrease in thickness for most areas of the alveolar bone with age.9 In this study, the average age of patients in all the groups was around 20 years, and no significant difference was observed in age between the groups. Therefore, it is reasonable to assume that alveolar bone change due to aging was not an influential factor in this study.
In previous studies, extensive development of perioral and masticatory musculature has been observed in low angled subjects which has been associated with thicker cortical bone.2829 Also, high angled subjects with posterior rotation of the mandible have been reported to have narrow shaped symphysis which is similar with the findings of this study in that Class III high angled subjects showed significantly thinner alveolar widths at most levels compared to that of Class III normal and low angled subjects.30 Chung et al.8 reported that skeletal Class III openbite patients showed thinner alveolar bone and lower bone height compared to patients in normal overbite relationships which could be related to a loss in function that could affect bone morphology. However, this study included 9 openbite and 22 normal overbite subjects in the Class III high angle group and there was no significant difference in alveolar bone thickness at all levels except for the buccal alveolar bone at 6 mm apical level between the two groups. Among the patients in the current study, overbite did not seem to have a distinct effect on mandibular alveolar thickness in the Class III high angle group.
Teeth with a healthy periodontium have an average total attachment of 2.04 mm from the gingival sulcus to the alveolar crest, which is where the CEJ is located.13 Therefore, the alveolar crest was defined as the 2 mm apical level from the CEJ. This study included broader areas in the mandibular alveolar bone by measuring 3 mm, 6 mm, and 9 mm level from CEJ as well as evaluating both buccal and lingual aspects which were detailed evaluations compared to previous studies.7931
Several reports have suggested that CBCT images of thin cortical bone may show blurring and that the voxel size may affect diagnostic accuracy.3233 A previous study suggested that cortical bone smaller than the voxel size may show a decrease in thickness of about 75.94% in the lingual bone and 62.88% in the buccal bone.7 Other studies have suggested using voxel sizes of 0.25 mm to measure cortical bone thickness.3435 However, a 0.3 mm voxel size was used in this study, which is a limitation for accurately evaluating cortical bone thickness, especially in the Class III high angle group. Future studies evaluating cortical and medullary bone thickness in detail would be beneficial for clinical application in orthodontic tooth movement. In addition, as this study focused on finding trends of difference in alveolar bone thickness in Class I and Class III individuals, subjects with extreme variations in bone thickness were excluded from this study. Moreover, this study included only patients with Korean ethnicity, which should be taken into consideration when interpreting the results as there are ethnic differences in craniofacial dimensions.36 Therefore, the findings of this study should be focused on relative comparisons of mandibular alveolar bone thickness in skeletal Class III patients with different vertical facial dimensions.
CONCLUSION
1. Class III high angle group showed thinner mandibular anterior alveolar bone at all levels except at the buccal alveolar crest and 9 mm apical level on the lingual side compared to the Class I group.
2. Class III high angle group showed thinner mandibular anterior alveolar bone than Class III normal and low angle group in most regions.
3. The mandibular plane angle was negatively correlated with buccal and lingual alveolar bone thickness.




 XML Download
XML Download