

 ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The bone morphology of the patient and the biomechanics used during treatment are important factors that must be taken into account before orthodontic treatment.1 If there is an imbalance between the resorption and apposition of the alveolar bone during orthodontic tooth movement, the tooth will move out of the alveolar envelope in a “through-the-bone” manner.2 Therefore, orthodontic forces can lead to different tissue responses, such as alveolar bone loss, gingival inflammation, root resorption, and pulpal reactions.34
Anterior deep-bite is a common complaint among orthodontic patients. The main treatment steps of anterior deep-bite and retroclined maxillary incisors involve incisor protrusion and intrusion mechanics. Intrusion of the maxillary incisors is particularly indicated in patients with excessive incisor and gingival display.56 An intrusive force would also tip the incisor teeth labially, because of the position of the force vector according to the center of resistance of the incisors.7 The effects of both intrusion and protrusion movements on the alveolar bone surrounding the incisors have previously been evaluated. Steiner et al.8 and Batenhorst et al.9 have experimentally demonstrated that marginal bone loss is associated with incisor proclination. Thongudomporn et al.10 investigated maxillary alveolar bone thickness after maxillary incisor proclination and extrusion, and found statistically significant decreases in the palatal and total bone thickness at the mid and apical levels of the root. Additionally, a recent study11 revealed that alveolar bone height and thickness decreased in response to different intrusion mechanics. Orthodontists may be unaware of the detrimental effects of the tooth movement, such as irreversible hard tissue changes, since the clinical observations may not reflect the underlying periodontal structures.12
Because of the limitations of two-dimensional lateral cephalograms in terms of investigating alveolar bone changes, particularly in the anterior region,1314 cone-beam computed tomography (CBCT) is the preferred tool for evaluating the alveolar bone qualitatively and quantitatively. 151617 To our knowledge, only one previous study11 has used CBCT to evaluate changes in the alveolar bone after incisor intrusion using 2 different segmented arches.
Given this lack of information, the primary purpose of the present study was to evaluate the effect of maxillary incisor intrusion on alveolar bone height and thickness, using CBCT scans. The secondary purpose of the study was to investigate dehiscence around the maxillary central incisors. The null hypothesis was that there would be no significant difference in terms of alveolar bone changes between the use of base-arch and of miniscrew intrusion mechanics.
MATERIALS AND METHODS
This retrospective study was approved by the Ethics Committee of Hacettepe University, with institutional review board number GO 17/13–11. The present study included patients' CBCT images obtained between 2010 and 2011 for a previous study, which had been conducted prospectively to evaluate the skeletal and dental effects, treatment period, and amount of root resorption observed when 4 maxillary incisors were intruded with miniscrew or base-arch approaches.18
In that previous study, the patients had been randomly assigned to either of the 2 treatment modalities. The sample size for the present study was calculated based on a significance level of 0.05 and a power of 80% to detect a significant difference of 0.78 mm with standard deviation of 0.72, according to the results of another study19 that evaluated changes in alveolar bone width. The power analysis showed that the minimum sample size should be 11 in each group.
The CBCT images were selected from the database of the department according to the following inclusion criteria: (1) post-adolescent patients (older 15 years); (2) anterior deep-bite ≥ 4 mm; (3) Class II or Class I malocclusion (2° < ANB < 6°) with a hypodivergent growth pattern (sella-nasion-mandibular plane < 32°); (4) no history of trauma to the maxillary anterior teeth; (5) a treatment plan including the intrusion of the maxillary incisors for correcting deep-bite malocclusion, by means of either conventional mechanics (base-arch) or miniscrews; (6) no evidence of periodontal or gingival problems at the start of orthodontic treatment; (7) CBCT scans available at the pre-intrusion phase (T0) as well as after achieving normal overbite (T1).
CBCT scans had been acquired previously, using an Iluma CBCT Scanner (3M IMTEC, Ardmore, OK, USA), with a voxel size of 0.3 mm at 3.8 mA, and 120 kVp. The data were recorded in Digital Imaging and Communication in Medicine & Management Solutions format and were evaluated using Dolphin 3D Imaging software v. 11.5 (Dolphin Imaging, Chatsworth, CA, USA).
Group I consisted of the CBCT images of 12 patients (8 female, 4 male) with a mean age of 16.51 ± 1.32 years, while Group II consisted of the CBCT images of 13 patients (6 female, 7 male) with a mean age of 17.47 ± 2.71 years. These patients had been treated previously with the 0.018-inch Roth prescription preadjusted brackets (Dentsply Sirona, York, PA, USA), applied to the maxillary central and lateral incisors, in combination with intrusion mechanics. Intrusion was started when leveling and alignment of the 4 maxillary incisors were completed with 0.016 and 0.016 × 0.016-inch nitinol arch-wires. In Group I, the 0.017 × 0.025-inch titanium molybdenum alloy Burstone-base-arch was applied to the maxillary incisors on a 0.016 × 0.016-inch segmental stainless steel arch-wire and the arch was inserted into the molar tubes with a gable-bend at the posterior segment with cinching-back. The active anterior part of the base-arch was adjusted to apply 100 g, as measured with a force gauge, and was connected to the anterior region between the lateral and central incisors bilaterally. In Group II, 1.4-mm diameter and 8-mm length miniscrews (DEWIMED; Medizintechnik GmbH, Tuttlingen, Germany) were inserted, using a self-drilling method, between the central and lateral incisors, bilaterally. An intrusion force was obtained by using nickel-titanium (Ni-Ti) coil springs from the segmental 0.016 × 0.016-inch stainless steel arch-wire to the miniscrews. In both treatment groups, a total of 100 g intrusion force (50 g to the right and 50 g to the left segment) was applied between the central and lateral incisors. Reactivations were applied every 4 weeks until adequate overbite was achieved.
T0 and T1 CBCT images were used to evaluate changes in the alveolar bone of 50 maxillary central incisors (26 teeth from Group I and 24 teeth from Group II). The intrusion duration was 0.39 ± 0.10 years for Group I, and 0.37 ± 0.07 years for Group II. The T1 CBCT was taken at a minimum of 6 months after the T0 CBCT.
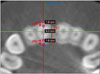
The perpendicular distance from the incisal edge of the maxillary central incisor to the palatal plane (PP) and the maxillary incisor inclination to the PP were measured to calculate the rate of incisor intrusion and proclination, respectively. The labial, palatal, and total alveolar bone thicknesses for each maxillary central incisor were measured in 3 slices, separated by 3 mm, at the widest point of the labiopalatal root along the long axis from the cementoenamel junction (CEJ). These measurements were defined as the labial bone thickness (LBT 3, LBT 6, and LBT 9 mm), palatal bone thickness (PBT 3, PBT 6, and PBT 9 mm), and total bone thickness (TBT 3, TBT 6, and TBT 9 mm) (Figure 1). The alveolar thickness of each side and the level of the maxillary right and left incisors were averaged to obtain the mean thickness. The measurements were made by two authors (E.A. and H.G.C.) in a sectional slice of 0.5-mm thickness (Figure 2), in a darkened room, according to the protocol of Timock et al.12
When the distance from the CEJ to the bone crest was greater than 2 mm, an alveolar bone defect was recorded, and it was classified as alveolar bone dehiscence.20 The prevalence of dehiscence in each treatment group for each incisor was carefully observed by two examiners (E.A. and H.G.C.).
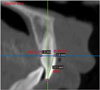
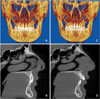
On the sagittal-cross section of the maxillary incisors, labial and palatal aspects were measured as the distance from the most apical portion of the CEJ to the most coronal portion of the marginal alveolar bone crest, defined as the buccal alveolar crestal height (BACH) and the palatal alveolar crestal height (PACH), respectively. Buccal bone height (BBH) measurements were defined as the linear distance between the most incisal point of the tooth's crown to the buccal alveolar crest along the long axis of the tooth (Figure 3). Pre- and post-treatment CBCT images of a representative case from Group II are shown in Figure 4.
Statistical analysis
Statistical calculations were performed with IBM-SPSS for Windows software, version 21 (IBM Co., Armonk, NY, USA). Independent t-tests were used to evaluate the demographic differences (age and intrusion duration) between the groups. Wilcoxon's signed-rank test was used to compare the initial (T0) measurements between the groups. Statistical comparison of alveolar thickness and heights in the different groups were conducted using two-way repeated-measures ANOVA. Bonferroni adjustment was applied to avoid Type I error due to multiple testing. Statistical significance level was set at p < 0.05. The prevalence of dehiscence was defined as frequency-%. Pearson's correlation coefficient analysis was used to assess the relationship between the dental and alveolar measurement changes.
To evaluate reproducibility, 25 teeth from the total sample were randomly selected for remeasurements at T0 and T1 at an interval of 30 days. The intraclass correlation coefficients were between 0.756 and 0.981.
RESULTS
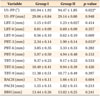
The pretreatment group differences are presented in Table 1. The two groups were generally similar at T0, and there were no statistically significant differences between the groups, except for upper central incisor (U1)-palatal plane (PP)° (p = 0.022), and PBT-3 mm (p = 0.033) (Table 1).
Dental and alveolar bone changes between T0 and T1 and comparison of these changes between the groups are presented in Table 2.
Dental measurements
Overbite significantly decreased with treatment in both groups (p < 0.05). The upper incisor inclination in relation to the palatal plane (U1-PP°) significantly increased with treatment in both groups (p < 0.05). There was a statistically significant decrease in the U1 to PP distance in Groups I and II of −2.58 mm and −3.40 mm, respectively (p < 0.05). The treatment-induced increase in U1-PP° and the decrease in U1-PP distance measurements were significantly greater in Group II than in Group I (p < 0.05) (Table 2).
Bone thickness measurements
LBT at 3 mm and 6 mm decreased significantly in Group II from T0 to T1 (−1.12 ± 0.12 and −0.47 ± 0.09 mm, respectively; both p < 0.001) and the decreases were significantly greater than those observed in Group I (both p < 0.05). In Group I, LBT at 9 mm significantly increased with treatment (0.48 ± 0.17; p = 0.009); however, this increase did not differ from that seen in Group II. The TBT values did not show significant changes in either of the groups after treatment (Table 2).
Bone height measurements
BACH and BBH significantly increased in Group II from T0 to T1 (5.77 ± 0.62 and 5.92 ± 0.57 mm, respectively; both p < 0.001) and these changes were significantly greater in Group II than in Group I (both p < 0.05). Changes in PACH measurement were not significant in the treatment groups, and no differences were found in these changes between the groups (Table 2).
Prevalence of dehiscence
The frequency of dehiscence around the maxillary incisors is shown in Table 3. Twenty-four maxillary incisors from Group I and twenty-six maxillary incisors from Group II were evaluated. The prevalence of dehiscence at T1 (with no dehiscence at T0) for the maxillary right and left central incisors were, respectively, 16.7% and 25% in Group I and 100% and 84.6% in Group II. In Group II, only 1 tooth showed dehiscence at both T0 and T1.
Correlation coefficients (r) between dental alveolar changes/initial bone thickness and alveolar bone measurement changes are presented in Table 4. The LBT change at 3 mm was strongly and positively correlated with the amount of upper incisor intrusion (r = 0.539; p = 0.005). The change in TBT at 9 mm was negatively correlated with the change in the upper incisor inclination (r = −0.436; p = 0.029) and with the initial TBT at 9 mm (r = −0.507, p = 0.010).
DISCUSSION
In orthodontics, the main treatment goals are to maximize the desired tooth movement and to minimize the undesirable side effects on the periodontal structure surrounding the teeth. For optimal stability of the teeth and periodontal health, alveolar bone support is an important factor to consider in orthodontic treatment. Currently, using CBCT images is a highly accurate measuring method for evaluating the alveolar bone dimensions with a high degree of accuracy between direct measurements and CBCT.1221 This retrospective CBCT study was performed to evaluate the alveolar bone loss around the maxillary central incisors that is induced by two different intrusion mechanics (base-arch or miniscrew), after the leveling and aligning stage.
We found a statistically significant decrease in labial alveolar bone thickness at the crestal and midroot levels in the miniscrew group (Group II). Significantly greater changes were observed in the miniscrew group than in the base-arch group (Group I), which might be related to greater changes in inclination and intrusion of the maxillary incisors. In the base-arch group, the arch-wire was extended into the molar tube with cinching-back and a gable bend, and these mechanics may play a role in limiting the excessive labial tipping of the anterior teeth. However, in the miniscrew group, segmental archwire, including only the 4 maxillary incisors, was used, which may be the reason for the greater labial tipping of incisors in the miniscrew group. The biomechanical explanation for the different amounts of incisor intrusion may be related to the use of continuous force (Ni-Ti coil in the miniscrew group) vs. a linear decrease of force in the base-arch group. Tian et al.22 showed that lingual-inclined maxillary central incisors had less bony support and a greater frequency of alveolar bone defects than normally inclined maxillary incisors. In the present study, the lingual inclination of the maxillary incisors at the T0 was greater in the miniscrew group, which might be a factor in the greater labial alveolar bone loss in this group.
However, our results showed that total alveolar bone thickness did not change, but was maintained in both treatment groups. This suggests that the rate of labial alveolar bone resorption was relatively higher than the rate of apposition on the lingual aspect in the miniscrew group, which may lead to a decrease in the LBT at the crestal level. Similarly, the findings of different studies19232425 showed a significant decrease in bone thickness in the direction of tooth movement. However, Thongudomporn et al.10 investigated changes in maxillary alveolar bone thickness after maxillary incisor extrusion and proclination and did not find significant changes in LBT in the direction of tooth movement. In contrast, they found significant changes in palatal and total alveolar bone thicknesses at the mid and apical levels of the root. Kaied and Tanielian11 evaluated the effects of incisor intrusion using segmented and utility arches and found significant decreases in alveolar bone thickness in both treatment groups. However, in the present study, the base-arch group did not show a significant decrease in alveolar bone thickness. The differences between the studies may arise from the different type of biomechanics used, different force magnitudes, and individual response differences in terms of the bone remodeling rate.
The results of this study showed that the percentage of dehiscence at the maxillary right and left incisors was significantly greater in the miniscrew group than in the base-arch group; in accordance with this result, the loss of the alveolar crestal height and bone height on the labial side in the miniscrew group was significantly greater than those in the other treatment group. However, clinically, no occurrence of gingival recession was encountered in the miniscrew group.
Tooth movements, which decentralize the teeth from the alveolar ridge, may be a critical factor for developing bone dehiscence.26 In the present study, the upper anterior alveolar bone was subjected to an intrusion force with upward and forward direction, which might lead to concentration of stress and deformation on the labial alveolar ridge crest.27 Similarly, Bimstein et al.28 indicated that the change in alveolar bone height of protruded mandibular incisors may be influenced by the change in both the inclination and intrusion of the central incisors. However, there is no direct association between buccal movement of the incisors and the occurrence of gingival recession.29 The periodontal status, such as the amount of keratinized gingiva, mucogingival problems, and harmful habits of the patients are other factors that must be considered at the pretreatment phase as risk factors of gingival recession.30
The extent of intrusion and the inclination of the maxillary incisors showed positive and negative correlation with changes in LBT at 3 mm and TBT at 9 mm, respectively. This may be because increased intrusion and decreased inclination can be expected to trigger increased labial alveolar bone changes at the crestal level and decreased total alveolar bone changes at the apical level, respectively, during upper incisor intrusion.
The pretreatment total alveolar bone thickness was negatively correlated with the change in the TBT at 9 mm. This suggests that a greater decrease in bone thickness may occur if the TBT at the level of the maxillary incisor apex is thinner. Garlock et al.3 also found that there was a weak negative correlation between facial vertical bone recession and the pretreatment cortical bone thickness at the apex level of the mandibular anterior teeth.
Some caution should be taken while intruding the upper incisors. For example, miniscrews can be placed distally to the canines to reduce the degree of labial tilting of the upper incisors, in order to minimize the possible stress at the alveolar ridge. Cho et al.31 recently performed a three-dimensional finite element study, and reported that, when an intrusion force was applied distal to the lateral incisors, the amount of displacement of the anterior teeth was low and stresses were distributed across all anterior teeth, regardless of the alveolar bone loss.
Considering our findings, it would be beneficial to assess the prerequisite bone morphology prior to initiating orthodontic treatment. Careful analysis of the bone structure around the maxillary upper incisors, particularly in adult deep-bite patients who require both incisor proclination and intrusion, could be considered as an important pretreatment assessment step before planning the treatment protocol. The current study showed that the decrease in bone thickness and bone height and the prevalence of dehiscence after labialization and intrusion were significantly greater in the miniscrew group than in the base-arch group. This suggests that conventional intrusion mechanics, such as an intrusion utility arch or base-arch in which cinching-back of the arch-wire can be incorporated or miniscrew-assisted intrusion (with the miniscrew placed more distally) on a continuous arch-wire, rather than a segmental anterior wire, should be considered. This is particularly true for patients who have less favorable periodontal structure around the incisors at the beginning of the intrusion. Therefore, from a clinical perspective, the clinician should take cognizance of the individual's biological characteristics before choosing the type of the biomechanics used during the orthodontic treatment. Furthermore, light forces and long-term activations during orthodontic treatment would be useful to eliminate or reduce marginal alveolar bone loss by providing more time for alveolar bone remodeling.
It has been indicated that, when alveolar bone thickness is larger than the voxel size, measurements might be overestimated; in contrast, when it is smaller than voxel size, measurements may be underestimated.32 In the present study, statistically significant alveolar bone changes were greater than the voxel size of the CBCT images, which may be a limitation of the current study. This study was also limited by its retrospective study design. Further longitudinal follow-up investigations are necessary to reveal the exact alveolar bone response once treatment is completed. This would reveal the course of bone remodeling over time. Another limitation of this study is that CBCT images at T0 were taken before leveling and aligning of the incisors; thus, this study showed the effect of both proclination and intrusion, rather than purely the effect of intrusion.
CONCLUSION
The null hypothesis of the study was rejected. When the same intrusion force was applied with the 4 maxillary anterior teeth being intruded as a segment either with a base-arch or miniscrews, the degree of labial tilting and intrusion of the anterior teeth increased in both treatment groups, and to a greater extent in the miniscrew group. The degree of labial alveolar bone thickness and bone height decrease were also greater in the miniscrew group. The degree of change in labial inclination and intrusion should be taken into account during upper incisor intrusion, as these factors may increase the risk of alveolar bone loss. The data on morphology of the alveolar bone as analyzed by means of CBCT can guide the orthodontic treatment plan and indicate the limits of tooth movement.




 XML Download
XML Download