

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Hepatitis B virus (HBV) infection is one of the most common chronic viral infections [1], and HBV-infected patients carrying different HBV genotypes could have diverse outcomes. Genotype C, which is the most prevalent HBV genotype in Korea, has a higher incidence of natural antiviral-resistant mutation than genotypes B and D and thus could lead to poorer therapeutic response and outcome [2]. The detection and quantification of HBV DNA are essential for diagnosis, establishing the prognosis of HBV infection, and monitoring the virologic response to antiviral therapy [34]. International clinical practice guidelines recommend the use of sensitive nucleic acid amplification technologies for HBV DNA detection [35]. These methods meet the current clinical criteria for detection of a dynamic range of up to 109 IU/mL with linear quantification and a limit of detection (LOD) of 10–20 IU/mL [6789]. However, the available automated HBV DNA assays with nucleic acid amplification technologies are generally designed for batch testing of multiple samples; thus, it is difficult to provide results to clinicians on a priority basis.
The DxN VERIS Molecular Diagnostics System (Beckman Coulter, Brea, CA, USA) is a fully automated system for quantitative molecular assay that combines sample loading, nucleic acid extraction, reaction preparation, real-time PCR assay using TaqMan probes, and result interpretation [10]. The VERIS HBV assay uses a quantitative nucleic acid-based amplification technology and is calibrated to the third WHO International Standard for HBV (National Institute for Biological Standards and Control 10/164) [11]. All analytical processes are integrated within a fully streamlined workflow and random access system, enabling rapid quantification of HBV DNA. The system allows samples to be assayed as soon as they arrive in the laboratory, throughout the day. This reduces the turnaround time and decreases the hands-on time of medical technicians.
We evaluated the analytical performance of the DxN VERIS HBV assay in comparison with the Abbott RealTime HBV assay (Abbott Laboratories, Des Plaines, IL, USA) in Korean HBV patients with genotype C. This study was approved by the Institutional Review Board of The Catholic University of Korea (KC17TISI0041).
Plasma samples were collected for routine HBV DNA quantification in cases of chronic HBV infection at Seoul St. Mary Hospital, Seoul, Korea, between November 2016 and May 2017 using BD PPT EDTA gel tubes (Becton, Dickinson and Company, Franklin Lakes, NJ, USA). Samples left over after the assay were aliquoted into 6–10 microtubes and stored immediately at −20℃ until analysis.
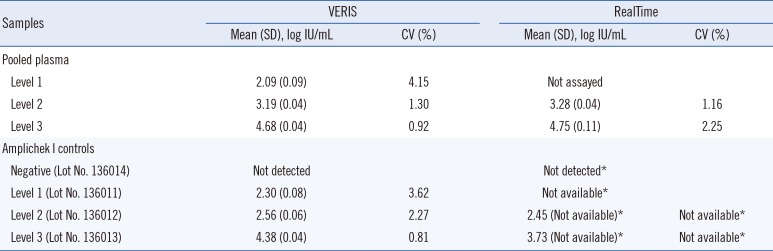
To assess precision, pooled plasma samples containing three different levels (2, 3, and 4 log IU/mL) of HBV DNA and a set of four commercial controls consisting of one negative and three different levels of HBV DNA as positive controls (Amplichek I, Bio-Rad Laboratories, Inc., Hercules, CA, USA) were assayed in duplicate, twice a day for five consecutive days. MedCalc version 17.6 (MedCalc, Ostend, Belgium) was used for statistical analyses, and P<0.05 was considered statistically significant.
The intra-assay CV of the VERIS assay ranged from 0.46% to 5.66% and 0.36% to 6.33% for pooled plasma and the Amplichek I HBV DNA positive controls, respectively. The inter-assay between-day precision CV ranged from 0.92% to 4.15% and 0.81% to 3.62% for pooled plasma and Amplichek I controls, respectively, suggesting good and similar precision at clinically meaningful levels of <100 IU/mL at the end of anti-viral therapy and >2,000 IU/mL at the time of diagnosis (Table 1).
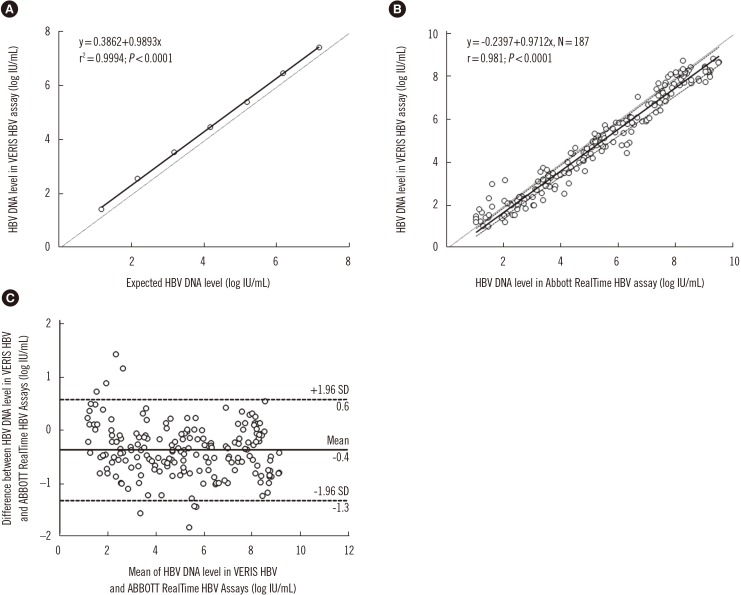
To evaluate linearity, seven serially diluted pooled plasma samples ranging from 7.18 to 1.18 log IU/mL were measured in triplicate. The levels of difference varied between 0.28 and 0.43 log IU/mL (Fig. 1A).
The lower limit of quantification (LLoQ) was estimated as 8.76 IU/mL (95% confidence interval [CI]: 7.32–12 IU/mL) by Probit analysis using 10 replicates of five levels of pooled plasma samples (approximately 40, 20, 10, 5, and 2.5 IU/mL) in the same experiment. This was equivalent to an LOD of 10 IU/mL (1.00 log IU/mL), according to the manufacturer. Specificity was assessed with eight samples collected from patients with other viral infections (cytomegalovirus, Epstein-Barr virus, hepatitis C virus, and HIV); these were all determined to be negative using the VERIS HBV assay.
For comparative evaluation between the VERIS and RealTime assays, 187 samples ranging from 1.04 to 9.51 log IU/mL (determined using the RealTime assay) were sequentially chosen at random and stored at −20℃ for up to three days before re-analysis. Of these, 57.2% (107/187) and 36.4% (68/187) showed delta differences of <0.5 log IU/mL and 0.5–1.0 log IU/mL, respectively. This result was superior to that of Braun et al. [11] who found that concordance between the two assays was 76% (47.8% and 36.7% of their samples showed delta differences of <0.5 log IU/mL and 0.5–1.0 log IU/mL, respectively). Passing-Bablok regression analysis did not reveal any significant deviation from linearity between the VERIS and RealTime assays (r=0.981; P<0.0001 by Spearman's rank correlation coefficient; linear regression equation, y=−0.2397+0.9712x; P=0.64 by the cumulative sum control chart [CUSUM] test for linearity; Fig. 1B). The mean difference in HBV DNA levels between these two assays was −0.3674 log IU/mL (95% CI, −0.4373 to −0.2974) in the Bland-Altman plot (Fig. 1C). Braun et al. [11] also demonstrated a strong correlation between the VERIS and RealTime assays (r=0.933).
To assess the influence of HBV drug resistance mutations on HBV DNA quantification, plasma samples from 20 patients with drug-resistant HBV genotype C infection were assayed in parallel using the VERIS and RealTime assays. Both assays showed a strong correlation (r=0.961; P<0.0001; linear regression equation, y=−0.5415+0.9954x; P=0.36) for the 20 drug-resistant HBV DNA samples, with a mean difference of −0.4425 log IU/mL (95% CI, −1.3985 to 0.5135). We confirmed good concordance between the VERIS and RealTime assays in Korean patients with HBV genotype C. In contrast, in Braun et al.'s study [11], the readings obtained from the Roche COBAS TaqMan HBV test (Roche Molecular Systems, Pleasanton, CA, USA) and VERIS were higher than expected for genotype D and lower than expected for genotype A (to a lesser extent), with genotypes D and A being the most prevalent genotypes in Europe.
Although several factors, including quality and stability of reference standards, quality and stability of reagents, and statistical validity of the calibration curve may lead to assay discrepancies, the negative bias was consistent across the dynamic range of DNA quantification for the VERIS assay compared with the RealTime assay, which is similar to the results (−0.39 log IU/mL) of Braun et al. [11]. This finding could influence treatment decisions at HBV DNA levels of <2,000 IU/mL according to the Korean Association for the Study of the Liver guidelines for immune-active phase chronic hepatitis B [12] because of the underestimation of DNA quantification. However, treatment decisions are based on various factors, such as patient age, liver enzyme levels, liver histopathology, previous treatment history, and family history [5]. This consideration of multiple factors lessens the impact of the negative bias observed with the VERIS HBV assay.
We showed that the VERIS assay has good precision and excellent analytic sensitivity, with an estimated LLoQ equivalent to that claimed by the manufacturer. Furthermore, we demonstrated that it accurately quantifies HBV DNA levels in clinical samples. Its performance appears to be similar to that of the RealTime assay, a real-time PCR platform widely used in clinical practice in HBV genotype C. Although the VERIS assay will not be available in the future in the automated assay market, many laboratories worldwide, including those in Korea, still use this assay for clinical samples. Our performance data can also serve as a future benchmark for random access, automated viral nucleic acid detection assays, as well as for HBV DNA assays [4131415].
One limitation of our study is that the influence of the different HBV genotypes on HBV DNA quantification was not assessed. We assayed only 20 drug-resistant HBV genotype C positive samples and confirmed the previous results by Fourati et al. [10], who demonstrated a median difference of −0.32 log IU/mL between the VERIS HBV and Cobas AmpliPrep/Cobas TaqMan 96 HBV v2.0 assays for genotype C. The prevailing HBV genotypes in Korea are genotype C2 or a mixed pattern of genotypes B and C, while other genotypes rarely occur [16]. Therefore, our performance data are not applicable for detecting HBV DNA with different genotypes. In conclusion, the VERIS assay demonstrated performance similar to the RealTime assay and is suitable for high-throughput HBV DNA monitoring in large hospital laboratories.
 XML Download
XML Download