

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sjögren's syndrome (SS) is an autoimmune disease that mainly affects exocrine glands such as salivary and lacrimal glands, which become inflamed because of chronic lymphocyte infiltration. The disease eventually results in xerostomia and keratoconjunctivitis sicca. Exocrinopathy can be observed alone (primary SS) or in the presence of other autoimmune disorders such as rheumatoid arthritis, systemic lupus erythematosus, or progressive systemic sclerosis (secondary SS) [1]. Primary SS tends to occur between 40 and 60 years, with a female to male ratio of 10:1 [1]. In Taiwan, the prevalence rate is 16.0 per 100,000 persons (female:male ratio=7.9), and the incidence rate is 10.6 per 100,000 person-year (female:male ratio=6.3) [2]. Although the detailed etio-pathogenesis is still unclear, SS may be related to viral infection, sex hormones (e.g., estrogen), and genes (e.g., HLA, cytokine genes) [345].
Rheumatoid factor (RF) can be classified into five types: IgA, IgG, IgM, IgE, and IgD [678]. The serum of approximately 40–60% of primary SS patients tests positive for RF-IgM [910]. Interleukin-6 (IL-6), interleukin 17A (IL-17A), and tumor necrosis factor-alpha (TNF-α) are pro-inflammatory cytokines, which are related to inflammation in many autoimmune diseases, including primary SS.
Serum immunoglobulins belong to a domain of the European League Against Rheumatism SS disease activity index [11]. Immunoglobulin levels are related to SS disease activity. Hypergammaglobulinemia also contributes to an elevated erythrocyte sedimentation rate (ESR), which is common in patients with primary SS [1213].
Several studies have explored the pathogenic factors in the serum and saliva of primary SS patients, but their results were contradictory. Some showed increased saliva IL-17A or TNF-α level in SS patients compared with control levels, but a few others reported differently [141516]. We investigated immunological abnormalities in the saliva (which is easy to obtain) of primary SS patients. We aimed to identify saliva indicators of disease activity, by comparing four inflammation-related immune parameters (IL-6, IL-17A, TNF-α, and RF-IgA) between patients and normal controls. We also examined the correlations between these four saliva parameters and clinical parameters (ESR, serum IgG, serum IgA, and serum IgM) in patients.
Go to : 
METHODS
Study population
This prospective study was performed at Kaohsiung Medical University Hospital from January to December 2014. Saliva and peripheral blood were obtained from 138 Taiwanese patients (median age: 56 years; range: 17–83 years; 131 females) diagnosed as having primary SS according to the criteria of the American European Consensus Group [17]. We also recruited 100 Taiwanese normal controls (median age: 55 years; range: 12–84 years; 95 females). No significant differences in age and sex distribution were observed between patients and controls. Written informed consent was obtained from all patients and controls, and the study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUH-IRB-20130249).
Saliva collection, processing, and immune parameters
The patients were asked to avoid eating, smoking, chewing gum, or drinking liquids except for water for one hr before saliva collection. The patients rinsed their mouths twice with warm water and waited for 10 minutes until naturally secreted saliva wetted their mouths. Then, they were asked to spit all the saliva into an empty 40-mL sterile container within 20 minutes. The saliva was placed in a 15-mL centrifuge tube and centrifuged at 1,000×g for 10 minutes. The supernatant was aliquoted into Eppendorf tubes for direct experimental analysis or preserved at −80℃. IL-6, IL-17A, and TNF-α levels were detected using ELISA MAX Deluxe Sets (BioLegend, San Diego, CA, USA). The Phadia 250 automatic analyzer was used to analyze RF-IgA levels, using the fluorescent enzyme-linked immunoassay (FEIA) method with EliA RF IgA test-Specific Reagents (Thermo Scientific, Waltham, MA, USA).
Blood collection, processing, and clinical parameters
Four milliliters peripheral blood from primary SS patients was taken into SST sterile vacuum tubes (BD, Franklin Lakes, NJ, USA), which were centrifuged at 1,000×g for 10 minutes to analyze serum IgG, IgA, and IgM using the IMMAGE 800 Immunochemistry System (Beckman Coulter, South Kraemer Boulevard Brea, CA, USA) by nephelometry, using system reagents. Subsequently, 1.28 mL blood was transferred to Monosed GE011-B vacuum tubes (BD) for ESR of whole blood using the MONITOR 20 automated ESR analyzer (JOKOH, Kawasaki, Japan).
Statistical analysis
The data of immune parameters showed a normal distribution. Therefore, the t-test was used to compare IL-6, IL-17A, TNF-α, and RF-IgA levels between primary SS patients and normal controls. Pearson's correlations were calculated between immune parameters and clinical parameters. P<0.05 was considered statistically significant. SPSS version 20 (IBM, New York, NY, USA) was used for statistical analysis.
Go to :
RESULTS
As shown in Table 1, IL-6 level was higher in primary SS patients than in normal controls (P=0.012), but no significant differences were observed in TNF-α, IL-17A, and RF-IgA levels.
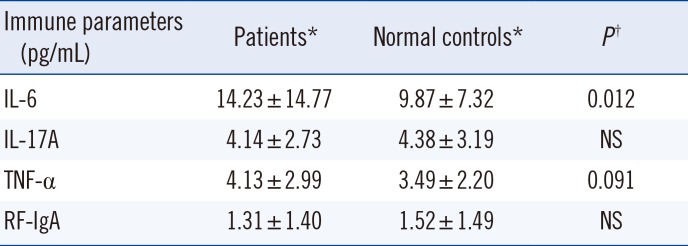
Table 1
Saliva immune parameters of primary Sjögren's syndrome patients (N=138) and normal controls (N=100)
| Immune parameters (pg/mL) | Patients* | Normal controls* | P† |
|---|---|---|---|
| IL-6 | 14.23 ± 14.77 | 9.87 ± 7.32 | 0.012 |
| IL-17A | 4.14 ± 2.73 | 4.38 ± 3.19 | NS |
| TNF-α | 4.13 ± 2.99 | 3.49 ± 2.20 | 0.091 |
| RF-IgA | 1.31 ± 1.40 | 1.52 ± 1.49 | NS |
![]()
In primary SS patients, saliva IL-6 level correlated weakly with ESR and serum IgG level (P=0.015 and 0.017, respectively), while saliva TNF-α level correlated weakly with serum IgG level (P=0.024; Table 2).
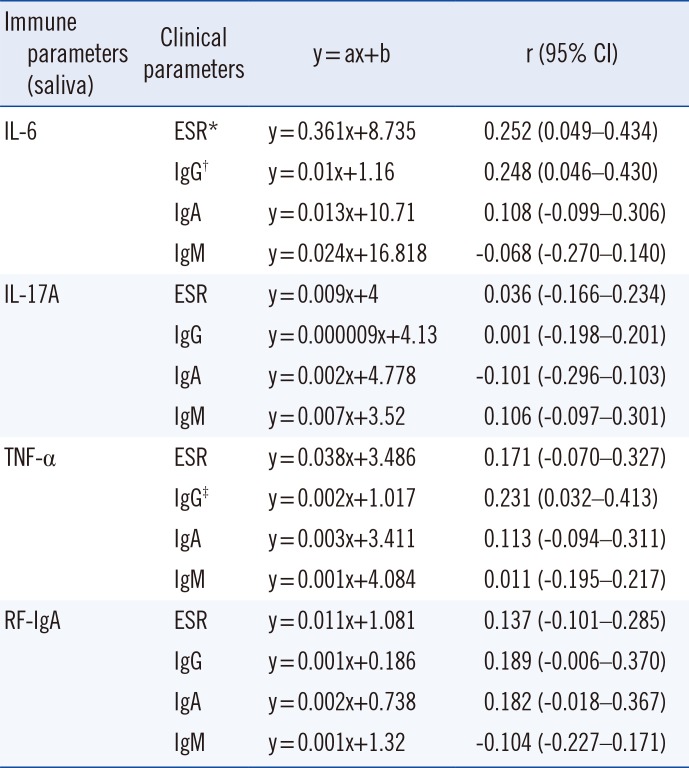
Table 2
Pearson's correlations between immune parameters and clinical parameters in primary Sjögren's syndrome patients
![]()
Go to :
DISCUSSION
Inflammatory cytokines were thought to be involved in the pathogenesis of primary SS by directly interfering with the epithelial cells in the salivary gland [18]. High saliva IL-6 level also correlated with cell infiltration in the gland [19]. Fox et al. [20] showed that the epithelial cells of the salivary glands of primary SS patients showed a high IL-6 level. Thus, IL-6 may be related to the pathogenesis of primary SS. We found that saliva IL-6 level was higher in primary SS patients than in normal controls. Our findings support several previous studies, which showed increased IL-6 levels in the saliva of primary SS patients in comparison with normal controls [1921].
IL-17 may impair salivary tight junction integrity and play a role in salivary gland dysfunction [22]. IL-17A can also induce the pathological changes of SS-like disease in SS-non-susceptible mice [23]. Lin et al. [24] showed that T helper-17 (Th17), IL-17-secreting cells, play an important role in the development of experimental SS. These findings demonstrated that IL-17A may be related to the pathogenesis of primary SS. Several studies showed that IL-17A levels were significantly higher in primary SS patients than in normal controls [1925]. However, there was no significant difference in saliva IL-17A level between primary SS patients and controls in our study. Our results support those of Nguyen et al. [15]. The discrepancy may be caused by lower disease activity in our patient group.
TNF-α is a pro-inflammatory cytokine, which is related to inflammation and apoptosis. TNF-α may induce activation of matrix metalloproteinase-9, and results in destruction of the salivary gland [26]. Zhou et al. [27] showed that endogenous TNF-α was involved in the pathogenesis of SS in non-obese diabetic mice. Some studies showed increased saliva TNF-α levels in primary SS patients compared with controls [1428]. However, Moriyama et al. [16] found no significant difference in saliva TNF-α level between primary SS patients and controls. In our study, saliva TNF-α level tended to be higher in patients than in controls, but this difference was not statistically significant. Targeting TNF-α with an anti-TNF monoclonal antibody (mAb) showed a therapeutic effect in a cell line [29]. However, a randomized controlled trial found no evidence of the efficacy of infliximab, a type of anti-TNF mAb, in primary SS patients [30]. Therefore, the role of TNF-α in the pathogenesis of primary SS still needs investigation.
We also showed that saliva IL-6 level in primary SS patients correlated weakly with ESR and serum IgG level, and that saliva TNF-α level correlated weakly with serum IgG level. Immunoglobulin levels are related to disease activity of primary SS, and hypergammaglobulinemia reflects lymphocyte hyperactivity in peripheral blood [13]. Several studies have demonstrated relationships between hypergammaglobulinemia and extra-glandular manifestations of primary SS, especially cutaneous vasculitis and articular, pulmonary, and renal involvements [931]. Hypergammaglobulinemia also contributes to elevated ESR, which is common in patients with primary SS [12]. As serum immunoglobulin levels may be associated with the disease activity of primary SS, saliva IL-6 and TNF-α levels may be related to disease activity in primary SS patients.
Markusse et al. [32] showed that RF-IgA levels in the saliva and serum of primary SS patients increased significantly. However, we did not observe a significant difference in saliva RF-IgA level.
A limitation of this study is that we did not examine immune parameters in salivary gland tissue. We also did not investigate the correlations between saliva immune parameters and clinical manifestations, especially extra-glandular involvement. Further research is needed on the relationship between immune parameters in saliva and salivary gland tissue. Our results show that IL-6 may play a role in the pathogenesis of primary SS. Saliva IL-6 level could serve as an indicator of disease activity in primary SS patients.
Go to :
 XML Download
XML Download