

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The Platelet Function Analyzer-100 (PFA-100, Dade Behring AG, Düdingen, Switzerland) is a platelet adhesion-aggregation analyzer that uses disposable cartridges containing a membrane coated with collagen and a platelet agonist: epinephrine (Col/EPI) or ADP (Col/ADP). It was developed as an alternative to the bleeding time and the classical light transmission platelet aggregometry platelet function test. The high shear rates of blood generated by the analyzer and the platelet agonist make platelets plug at the aperture, and the time required to obtain full occlusion of the aperture is termed closure time (CT) [1].
The clinical efficacy of anti-platelet therapy in preventing occlusive vascular events in patients with atherothrombotic disease is well established [2]. Irreversible cyclooxygenase-1 (COX-1) inhibitors, such as aspirin, and ADP receptor antagonists, such as clopidogrel and ticagrelor are most widely used drugs for anti-platelet therapy [3]. The detection rates of PFA-100 with Col/EPI for aspirin-induced platelet dysfunctions range between 60% and 70%, while those of Col/ADP for clopidogrel testing are much lower than for aspirin [4567]. The antiplatelet effect of non-steroidal anti-inflammatory drugs (NSAIDs) remains unclear [89]. Some studies have claimed that NSAIDs increase the risk of bleeding [91011], while others have found that some NSAIDs could increase the risk of atherothrombotic events [812].
Some patients with adequate treatment adherence may exhibit normal platelet activity in laboratory monitoring testing, or normal CTs in PFA-100, a phenomenon termed as high on-treatment platelet reactivity (HTPR). Causes of aspirin- or clopidogrel-related HTPR in PFA-100 tests include younger age, female sex, high body mass index, hyperglycemia, hypercholesterolemia, patient non-adherence, drug malabsorption, and pharmacological interactions [1314151617]. However, except for patient non-adherence or antiplatelet drug pharmacokinetics, the clinical factors contributing to HTPR remain unclear and vary across studies [15].
We retrospectively investigated the effectiveness of PFA-100 for clinical laboratory screening of aspirin-, clopidogrel-, and NSAID-induced platelet dysfunction with practical PFA-100 data for over six years from the 6,957 patients. To our knowledge, this is the largest single-center study to do so. In addition, we compared the clinical and laboratory characteristics of patients with prolonged and normal CTs, to determine potential contributors to HTPR.
Go to : 
METHODS
Patients
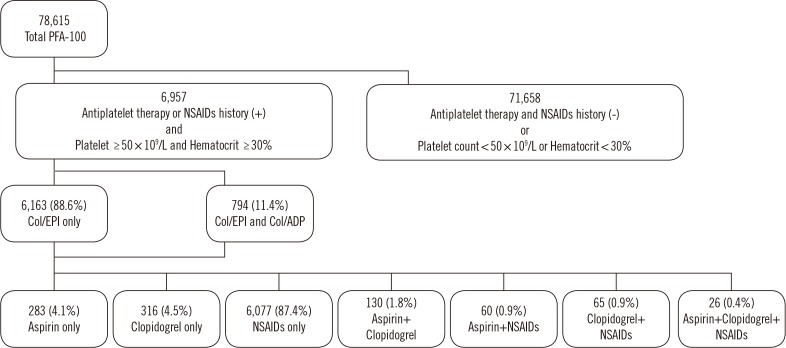
The medical records of 78,615 patients who underwent PFA-100 testing (Col/EPI or Col/EPI+Col/ADP) from March 2010 to April 2016 in Chung-Ang University Hospital, Seoul, Korea, were reviewed. Of these patients, those with Hct <30% or platelet counts <50×109/L were excluded because of the known interference of these factors with PFA-100 results [1819]. Patient medical records were reviewed to determine aspirin and clopidogrel received within a week before PFA-100 testing and NSAIDs received within 24 hours before testing; these cutoffs were determined based on the platelet life span and duration of drug actions [20]. The investigated NSAIDs were acetaminophen, ibuprofen, dexibuprofen, ketorolac, zaltoprofen, ketoprofen, aceclofenac, meloxicam, piroxicam, and mefenamic acid. Patients who had not received such drugs were excluded. After reviewing the medical records, total of 6,957 patients were selected. The median age was 57.0 years (range 1–103 years), and 3,517 were male. Among the patients, 6,163 were tested only with Col/EPI, while 794 were tested with both Col/EPI and Col/ADP (dual test) according to the clinicians' requests. Further, 283, 316, and 6,077 had received only aspirin, clopidogrel, or NSAIDs, respectively, while 281 had received a combination of aspirin, clopidogrel, and NSAIDs (Fig. 1).
This retrospective study was approved by the Institutional Review Board of Chung-Ang University Hospital (Approval No. 1612-001-16019), and informed consent was waived.
Blood Collection and Analysis
Blood samples for PFA-100 testing were collected in 3.2% sodium citrate anticoagulant. The samples were stored at 24℃ until analysis. All PFA-100 tests were conducted between 10 minutes and four hrs after blood collection. Samples in pneumatic tubes and hemolytic samples were not used. All aspects of PFA-100 testing, including analyzer maintenance and quality control, were performed according to the manufacturer's instructions. Prolonged CTs were defined as CT >192 seconds with Col/EPI or >110 seconds with Col/ADP [21]. We assessed prolongation rates by calculating the percentages of patients with prolonged CTs for aspirin, clopidogrel, and NSAIDs.
We compared the followings between patients with prolonged and normal CTs: sex, age, white blood cell (WBC) counts, red blood cell (RBC) counts, prothrombin time (PT), activated partial thromboplastin time (aPTT), ABO blood type, erythrocyte sedimentation rate (ESR), total protein, albumin, creatinine, triglycerides (TG) level, HDL level, LDL level, total cholesterol, and patient diagnosis.
Statistics
The Kolmogorov–Smirnov test was conducted to test the normality of continuous variables. Normally distributed variables were summarized as mean±SD, and non-normally distributed variables were summarized as median and range. Comparisons were performed using the independent t-test for normally distributed variables, the Mann-Whitney U test for non-normally distributed variables, or the chi-square test with R-by-C cross tab for categorical variables.
All analyses were performed with SPSS version 19 (IBM, Armonk, NY, USA) and Microsoft Excel (Microsoft Corp Inc., New York, NY, USA). P<0.05 was considered significant.
Go to :
RESULTS
All Col/EPI results are listed in Table 1. The prolongation rates for aspirin, clopidogrel, and NSAIDs when received solely were 73.5% (208/283), 70.9% (224/316), and 54.9% (3,333/6,077), respectively. When the drugs were administered in combination, the prolongation rates ranged from 65.0% to 84.6%. Further, 42.9% (2,987/6,957) of the patients had normal CTs in the Col/EPI test.
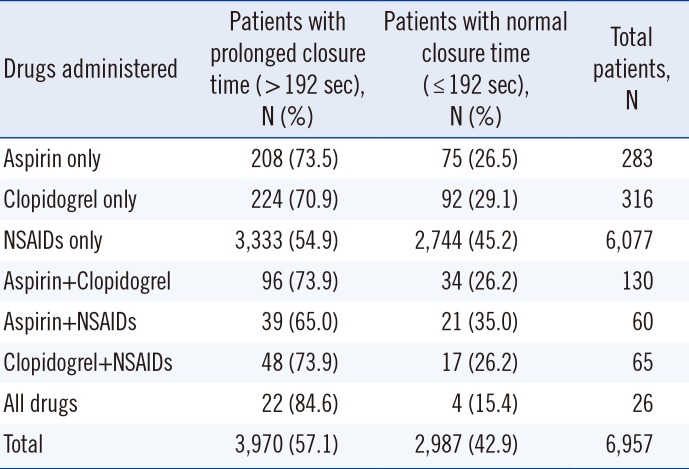
Table 1
PFA-100 Col/EPI closure times
![]()
The PFA-100 results from dual test patients are listed in Table 2; 90.1% (715/794) showed prolonged CTs, while 10.0% (79/794) had normal CTs, all of whome were receiving aspirin, clopidogrel, and NSAIDs solely.
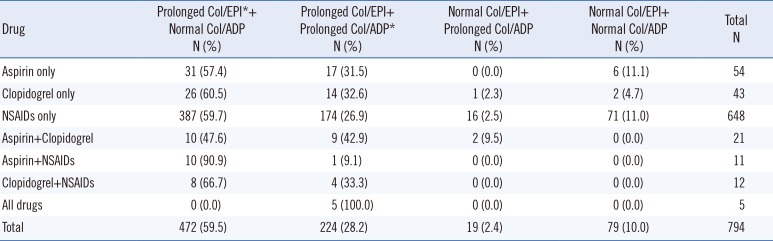
Table 2
PFA-100 results for patients tested with both Col/EPI and Col/ADP
![]()
Of the dual test patients, 2.4% (19/794) showed an atypical pattern for PFA-100 results: normal CTs with Col/EPI and prolonged CTs with Col/ADP. This atypical pattern was observed in a higher percentage of patients receiving both aspirin and clopidogrel (9.5%, 2/21) than those receiving any other drug combinations.
Among patients undergoing the Col/ADP test alone (Table 2), the prolongation rates for aspirin, clopidogrel, and NSAIDs, regardless of their combination with other drugs, were 37.4% (34/91), 43.2% (35/81), and 29.6% (200/676), respectively. Approximately 65.1% (28/43) of patients receiving only clopidogrel had normal CTs.
Table 3 shows a comparison of clinical and laboratory characteristics between patients with prolonged and normal CTs. Among patients receiving only aspirin in the Col/EPI group, median WBC counts were higher in the normal CT group than in the prolonged CT group (6.980 vs 6.580×109/L, P=0.031), and TG levels were lower in the normal CT group than in the prolonged CT group (0.97 vs 1.60 mmol/L, P=0.027).
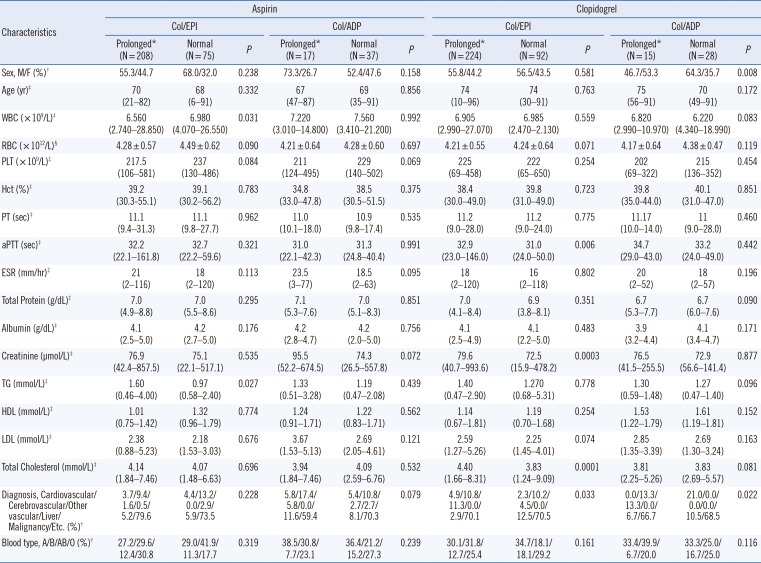
Table 3
Clinical and characteristics of patients with normal and prolonged PFA-100 closure times
*Prolonged CTs were defined as >192 seconds with Col/EPI or >110 seconds with Col/ADP; †P values were calculated using the chi-square test with R-by-C cross tab; ‡Data are displayed as median value (range), and P values were calculated using the Mann-Whitney U test; §Data are displayed as mean±SD, and P values were calculated using the independent t-test.
Abbreviations: PFA-100, Platelet Function Analyzer-100; Col/EPI, collagen/epinephrine cartridge; Col/ADP, collagen/ADP cartridge; M/F, male/female; WBC, white blood cells; RBC, red blood cells; PLT, platelet; PT, prothrombin time; aPTT, activated partial thromboplastin time; ESR, erythrocyte sedimentation rate; TG, triglyceride.
![]()
In the Col/EPI test for patients receiving only clopidogrel, the normal CT group showed lower aPTT, creatinine, and total cholesterol than the prolonged CT group (31.0 vs 32.9 seconds, 0.021 vs 0.023 mmol/L, and 13,083.2 vs 15,028.0 µmol/L, respectively; P=0.006, <0.001, and <0.001, respectively). There was a higher percentage of patients with malignancies in the normal CT group than in the prolonged CT group (12.5 vs 2.9%, P=0.033).
In the Col/ADP tests for patients receiving only clopidogrel, the normal CT group had a higher percentage of males than females, whereas the prolonged CT group had a lower percentage of males than females (male–female, 64.3%/35.7% vs 46.7%/53.3%, P=0.008). The normal CT group had a higher percentage patients with malignancies (10.5 vs 6.7%, P=0.022) than the prolonged CT group.
Go to :
DISCUSSION
We investigated the detection rates of PFA-100 for laboratory screening of drug-induced platelet dysfunction and analyzed potential contributors to HTPR in a large number of patients over a period of six years. In the present study, the laboratory detection rate of Col/EPI for aspirin-induced platelet dysfunction was 73.5%, which accords with other studies [122]. The incidence of aspirin-related HTPR in patients with good compliance for aspirin is known to be extremely low (probably<1%) when specific methods, such as arachidonic acid stimulation in light transmission aggregometry (LTA), are used [523]. In contrast, PFA-100 yields much higher frequencies of aspirin-related HTPR, approximately 20–30% [523]. We found that 11.0–26.5% of patients had normal CTs, according to the tested cartridges. A study comparing LTA, VerifyNow (Accriva Diagnostics, San Diego, CA, USA), and PFA-100 revealed that the frequency of aspirin-related HTPR was higher in both VerifyNow and PFA-100, and that the agreement between tests was also poor, with a few patients showing aspirin-related HTPR in all tests [24]. Thus, the high frequency of aspirin-related HTPR in PFA-100 tests does not appear to reflect a truly poor response to aspirin.
In contrast to aspirin, clopidogrel-related HTPR in PFA-100 tests appear to reflect true resistance. Studies that used specific tests, including LTA to measure the pharmacological effect of clopidogrel, showed that a significant proportion of patients (15–30%) were very poor responders [52225]. In our study, 4.7–29.1% of patients receiving only clopidogrel showed normal results according to the tested PFA-100 cartridges. Inter-individual differences in the extent of clopidogrel metabolism to its active metabolites are the most plausible explanation for the variable responses observed in clopidogrel platelet inhibition. Multiple factors may contribute to clopidogrel metabolism. Genetic factors, including polymorphisms of the ABCB1 gene and polymorphisms of hepatic cytochrome P450 enzymes, can affect intestinal absorption and generation of the clopidogrel active metabolite. Body mass index, sex, ethnicity, and comorbidities such as liver diseases can also influence the antiplatelet effect of clopidogrel [2627282930].
The antiplatelet effect of NSAIDs is controversial. Some researchers have argued that NSAIDs cause platelet dysfunction [9101131]. In this context, many clinicians have utilized PFA-100 for laboratory detection of possible NSAID-induced platelet dysfunctions. In contrast, there are several reports that NSAIDs, especially COX-2 inhibitors, may be associated with an increased risk of thrombotic events [812]. We found that 54.9% of patients receiving only NSAIDs showed prolonged CTs on the Col/EPI test. These findings suggest that NSAIDs have anti-platelet effects. However, the proportion of patients showing normal CTs was higher in patients receiving both aspirin and NSAIDs than in patients receiving aspirin only. This finding indicates a competitive effect of NSAIDs with aspirin, as suggested in other studies arguing that NSAIDs may increase the risk of thrombotic events [812].
Usually, there is no need to perform a Col/ADP test if the Col/EPI CT is not prolonged, as the Col/ADP results can be predicted to be normal in >99.0% of test cases [32]. However, at our institution, many clinicians prefer running Col/EPI and Col/ADP tests simultaneously to promptly obtain the Col/ADP results when the Col/EPI CT is prolonged. The combination of a normal Col/EPI CT and prolonged Col/ADP CT is a rare phenomenon; therefore, precise clinical scenarios have not been clearly identified [32]. In our study, 2.4% of patients tested with both Col/EPI and Col/ADP showed this atypical combination. In particular, patients receiving both aspirin and clopidogrel showed a high frequency (9.5%; 2/21) of this pattern, followed by 2.5% (16/648) of patients receiving only NSAIDs, and 2.3% (1/43) of those receiving only clopidogrel; none of the patients receiving only aspirin showed this atypical pattern. Further investigations are needed to determine the underlying causes or mechanisms of this result.
We also found a higher frequency of malignancies in the normal CT group than in the prolonged CT group (for both Col/EPI and Col/ADP tests) for clopidogrel, but not for aspirin. Cancer-related thrombosis is a well-known complication of malignancies [3334]. Patient-related characteristics, such as advanced age, prolonged immobility, prior history of thrombosis, and anti-cancer therapies, are known to induce coagulation abnormalities [333536]. The biological mechanisms of increased platelet activation in malignancies include expression of procoagulant proteins (such as tissue factor), exposure to procoagulant lipids, release of inflammatory cytokines, ADP production by tumor cells, and increased levels of von Willebrand factor [3536373839]. The hypercoagulable state of malignancy may interfere with the drug effects of anticoagulants, leading to resistance [35].
TG, total cholesterol, and creatinine levels and female sex have been associated with increased thrombotic tendency or the cause of HTPR [131416]. In our study, TG, creatinine, and total cholesterol levels and proportion of females differed between groups; however, their values were lower in the normal CT group than in the prolonged CT group, and there was no consistency between the aspirin-Col/EPI, aspirin-Col/ADP, clopidogrel-Col/EPI, and clopidogrel-Col/ADP groups. Age, ABO blood type, Hct, and platelet counts are known to affect PFA-100 CT results and to contribute to HTPR [151632]; however, they did not significantly differ between the normal and prolonged CT groups in our study.
Our study had several limitations: First, we did not perform LTA to determine the true absence or presence of an antiplatelet effect. As described above, particularly in the case of aspirin, the correlation between LTA and PFA-100 is poor. Second, we did not assess the relationship between PFA-100 results and clinical outcomes, such as frequency or severity of bleeding complications. Third, we could determine only the time at which our pharmacy instructed the drugs to be taken, rather than the actual time at which the drugs were taken. Fourth, we did not assess the baseline PFA-100 results of the patients, owing to lack of data. However, this would have little effect on our findings because the prevalence of platelet dysfunction disorder is far lower in Korea than that in Western countries [40]. Fifth, we did not include glycoprotein IIb/IIIa receptor antagonists as one of NSAIDs, because of the limited number of patients who had received those drugs. Finally, as this was a retrospective study, we depended on medical records and could not confirm outpatients' adherence to drug regimens.
In conclusion, PFA-100 is not sufficiently effective for laboratory detection of drug-induced platelet dysfunction, and malignancy may contribute to HTPR. Further investigations are warranted to determine other contributing factors to clopidogrel-related HTPR in PFA-100 testing.
Go to :
 XML Download
XML Download