

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Urinalysis is a major diagnostic screening test in the clinical laboratory, with an important role in diagnosing and monitoring nephrological and urological conditions. Until recently, microscopic urine sediment analysis was the most widely accepted urinalysis methodology. However, this time-consuming methodology is associated with extensive analytical errors [1]. Over the past 25 years, new automated technologies and informatics have greatly reduced the labor intensity of urinalysis and have created new technical possibilities. This review presents the main recent developments in automated urinalysis and future perspectives.
Go to : 
IMAGE TRANSMISSION
Microscopic urine sediment analysis remains the key method for urinalysis; unfortunately, the required expertise is not widely available at any time (night time, weekends). Electronic transmission of images (telemedicine) can therefore be very helpful for obtaining diagnostic information [2], enabling consultation with experts regarding unusual or doubtful findings and the circulation of interesting findings throughout the medical and scientific community.
Go to :
TEST STRIP TECHNOLOGY
Although dry chemistry technology for urinary test strips has made limited progress, advances in electronic detection have considerably improved the analytical sensitivity of test strip readers over the years [3]. In 2002, Penders et al. [4] demonstrated that automated urine test strip reading enables quantitative analysis for red blood cells (RBCs), white blood cells (WBCs), glucose, and urinary protein. According to the reflectance theory formulated by Kubelka and Munk [5], the reciprocal value of reflectance readings is proportional to the concentration of the measured analyte. Applications of these quantitative test strip readings have been described for ketones [6] and albumin [7].
A classical dye-binding based albumin test strip in combination with a complementary metal oxide semiconductor (CMOS) based strip reader could allow quantitative analysis of albuminuria and the determination of the albumin:creatinine ratio. This development enables obtaining quantitative albumin readings in the microalbuminuria range (20–200 mg/L) [8]. The creatinine-specific test pad allows correction for urinary dilution, which is useful in the assessment of albuminuria [9].
Using CMOS technology, very sensitive readings can also be obtained for leukocyte esterase and peroxidase activity [10]. Similar to albuminuria, the reflectance data can be used for quantitative analysis [10]. In parallel, the use of sensitive dyes has improved the sensitivity of albuminuria test strips [11].
An interesting recent evolution is the use of smart phones for reading and interpreting urine test strip results [121314]. Mobile healthcare platforms have been proposed, combining a pocket-sized colorimetric reader and commercially available 10-parameter urinalysis paper strips, capable of sending data via a smart phone [15].
Go to :
AUTOMATED MICROSCOPY
In manual microscopy, several steps, such as centrifugation, decantation, and re-suspension, led to cellular lysis and loss [16]. Progress in informatics and computer technology has enabled the development of automated microscopy based on pattern recognition. Over the past two decades, a number of manufacturers have marketed such instruments (Table 1).
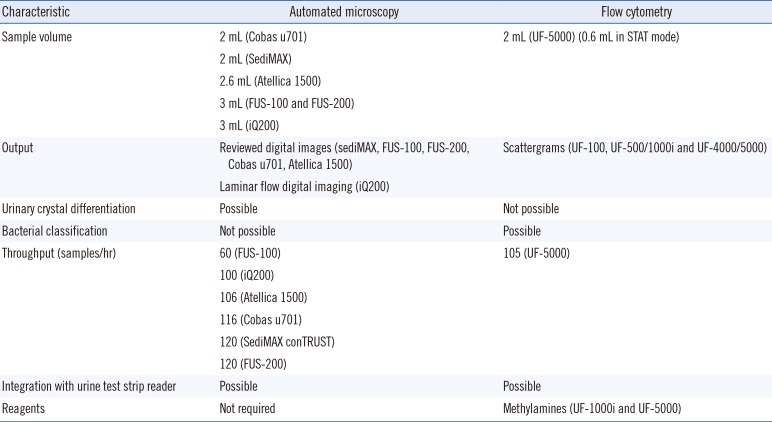
Table 1
Current automated urine analyzers
![]()
In contrast to most other automated urine microscopy analyzers, the iQ200 analyzer (Iris Diagnostics, Chatsworth, CA, USA) uses laminar flow digital imaging technology [1718192021]. Its identification software classifies and quantifies the cells and particles in uncentrifuged urine using a single, laminar flow of the specimen through the lens of a charged coupling device video camera. The hundreds of digital camera captures are evaluated by identification software, and each particle is classified based on characteristics, such as shape, contrast, and texture. After classification by the instrument, the operator has the ability to reclassify or correct the obtained images in the correct categories. Various studies have reported a strong correlation between iQ200 output and manual cell counts for RBCs, WBCs, and epithelial cells [1718192021]. This correlation coefficient has been 0.894 for RBCs when particle recognition software alone was used and 0.948 for RBCs after re-classification on iQ200 [18]. In the same study, the correlation for WBCs was 0.885 (vs the reference method), which improved to 0.978 following re-classification. The correlation coefficients for iQ200 output following user re-classification were 0.927 for squamous epithelial cells, 0.856 for casts, and 0.706 for non-squamous epithelial cells. iQ200 shows good linearity and precision, and no carry-over has been detected [1819]. In some cases, falsely elevated RBC counts may occur because of yeast misclassification; that is, yeasts can be confused with RBCs [19]. In addition, the system does not count damaged WBCs and counts fewer RBCs if abnormal RBCs, such as ghosts and dysmorphic cells, are present [22]. Counting results equal or exceed that of routine bright field microscopy or earlier flow cytometric technology. The instrument eliminates manual sample preparation; however, it requires a well-trained technologist for reclassification of findings. The optical system also allows for quantification of urinary bacteria [23]. Owing to the limited ability of the classification software, most problems occur during microorganism analysis [22]. The images of small cocci detected by iQ200 are difficult for the medical technologist to classify as “bacteria.” Better classification results have been obtained for some rod forms [2124]. In addition, detection of malignant/atypical urothelial cells, which may indicate bladder carcinoma diagnosis, has been achieved using automated intelligent microscopy on iQ200 with a sensitivity of identification of 87.5% [25].
FUS-100 (Dirui, Changchun, China) is a similar analyzer. Yüksel et al. [26] determined that the sensitivity of the FUS-100 for RBCs and WBCs is 73% and 68%, respectively; however, the related FUS-200 analyzer (Dirui) has been found to have unsatisfactory analytical sensitivity for bacteria recognition and quantification [27].
sediMAX (77 Elektronika, Budapest, Hungary) is an automated microscopy image-based urine sediment analyzer (which in some countries is also known as Urised). While iQ200 divides the identified particles in in different categories (RBCs and WBCs) [28], sediMAX shows the particles within whole fields of view, similar to microscopic fields seen with manual microscopy [29]. The instrument provides both bright field and phase-contrast images and generates a composite image out of the bright-field and phase-contrast microscopy images to exhibit the features of each image in one view. Its diagnostic performance with respect to visual phase-contrast microscopy has been evaluated [30]. Within-run imprecision was 17.8% and 6.7% at a concentration of 18×106/L and 447×106/L, respectively, for RBCs and 17% and 4.4% at a concentration of 4×106/L and 258×106/L, respectively, for WBCs. The between-run imprecision was 14.7% at a concentration of 30×106/L and 7.2% at a concentration of 283×106/L for RBCs and 5.4% at a concentration of 25×106/L and 3% at 166×106/L for WBCs. The area under the ROC curve (AUC) ranged from 80% to 90% for RBCs, WBCs, squamous epithelial cells, yeasts, and calcium-oxalate crystals. For non-squamous epithelial cells and pathological and hyaline casts, the AUC ranged from 73% to 74%; no carry-over was detected. Thus, sediMAX is well able to count and identify RBCs, WBCs, squamous epithelial cells, yeasts, bacteria, and calcium-oxalate crystals. Recognition of pathological casts and non-squamous epithelial cells is adequate but needs to be improved.
The second generation sediMAX analyzer (sediMAX 2, 77 Elektronika) allows distinction between four types of crystals: calcium oxalate dihydrate, calcium oxalate monohydrate, uric acid, and struvite. sediMAX conTRUST (77 Elektronika), which is the sediMAX 2 analyzer updated with phase-contrast microscopy, can detect other crystals as well; however, it is not able to identify them precisely, leading the software to classify them as unidentified crystals. The distinction between urine crystals using sediMAX conTRUST is specific but lacks sensitivity [31]. In addition, the system is suitable for parasite recognition [32].
The automated analyzers Cobas u701 (Roche Diagnostics, Mannheim, Germany) [3334] and Atellica 1500 (Siemens Healthineers, Eschborn, Germany) have been recently introduced in the market [35]. These analyzers are based on similar pattern recognition principles.
Go to :
FLOW CYTOMETRY
Urine particle flow cytometers (UFCs) have improved count precision and accuracy compared with visual microscopy and offer significant labor reduction. The first such UFC, the UF-100 (Sysmex, Kobe, Japan), could identify RBCs, WBCs, squamous epithelial cells, transitional epithelial and renal tubular cells, bacteria, hyaline and inclusional casts, yeast-like cells, crystals, and spermatozoa, using argon laser flow cytometry. Analytic and diagnostic evaluations have demonstrated acceptable linearity over clinically useful working ranges, with an imprecision that is consistently and significantly less than that of microscopy and with negligible carry-over. Studies have compared UFCs with chamber counts, quantitative urine microscopy, sediment counts, test strips, bacterial culture, and urine density [363738]. Clinical studies using UFCs have focused on diagnosis and monitoring of urinary tract infection; localization of the sites of hematuria; and diagnosis, monitoring, and exclusion of renal disease [36].
The classical argon lasers in UFCs have been replaced by semiconductor lasers, which have a much longer lifetime and hence are more economical. The introduction of semiconductor lasers (operating at another blue wavelength) has forced developers to completely redesign the system and adapt the dyes. The newer UF-5000 and UF-4000 (Sysmex) analyzers are able to recognize, count, and classify cells by analyzing forward scatter light (FSC), side scatter light (SSL), side fluorescent light (SFL), and depolarized side scattered light (DSS). DSS was introduced to improve crystal sensitivity and to better discriminate between RBCs and crystals [39]; however, in contrast to microscopy-based readers, differentiation of crystals is not possible.
The most popular approach is to combine test strips with UFCs for primary screening either using both methods (i.e., UFC and strips) or by utilizing the test strips for analytes unrelated to the UFC-analyzed particles. As mechanical coupling of UFCs and test strip readers has been realized [40], expert systems now exist combining both test modalities based on user-definable decision rules. The implementation of such a strategy significantly reduces microscopy review and saves time and cost without diminishing clinical utility.
With UF-1000i (Sysmex), bacteria forward scatter (B_FSC) and fluorescent light scatter (B_FLH) can be used for preliminary discrimination of urinary tract infections (UTIs) caused by gram-positive or gram-negative bacteria [41]. Evaluation of B_FSC and B_FLH parameters from bacteria histograms seems to be useful in distinguishing between gram-negative and gram-positive bacterial strains [42]. B_FSC data could be useful in presumptive exclusion of UTIs caused by gram-positive bacteria [41].
Urinary flow cytometry and UTIs
Urine culture is considered the gold standard for UTI diagnosis. It can determine the level of bacteriuria and antimicrobial susceptibility. However, there is no standardized bacterial count indicating significant bacteriuria, applicable for all types of UTIs. Scientific evidence supporting current urine culture guidelines is often incomplete, and in some cases, the guidelines do not indicate a clear choice [43].
Because of the high percentage of negative results (up to 60% depending on the setting [4445]), there is a need for an efficient screening method, reducing the number of unnecessary culture tests. Several methods for screening-out culture-negative samples have been developed, including dipstick chemical tests (nitrite, leukocyte esterase, urinary protein, and urinary hemoglobin) and manual or automatic microscopic examination of urine sediment (detection of particles, WBCs, and microorganisms). Although these screening methods are primarily used in general practice and microbiology laboratories, they are subjective and time-consuming and demonstrate poor sensitivity and negative predictive value [46].
Many authors have reported using flow cytometry to detect bacteria and WBCs in urinary samples. Flow cytometry can reduce the number of samples cultured, with a substantial decrease in workload, time, and costs, especially in clinical laboratories [464748]. Using flow cytometry, negative results could be reported earlier, substantially reducing unnecessary empirical antibiotic prescriptions. The use of flow cytometry can reduce the number of urinary samples processed in the clinical laboratory by 28–60% [4142444950515253545556]. However, there is a wide variation in the applied cut-offs, as well as in the sensitivity and specificity of the obtained results in the literature. These variations are mainly owing to the spectrum of clinical conditions of the patient populations enrolled in these different studies. These differences can be attributed to the different definitions used to classify UTIs, which depend on the guidelines applied in a specific setting. Therefore, we conclude that the applicability of flow cytometry to screen for negative urine samples strongly depends on population characteristics and the definition of a negative urine culture [44]. In addition, a limitation of automated urine analyzers compared with culture is that they count both live and dead bacterial particles, yielding higher particle counts [57].
Integrated urinalysis
To streamline the laboratory workflow, automated test strip readers and particle analyzers have been successfully mechanically integrated. In addition to mechanical integration, the development of expert systems has enabled the comparison and identification of cases that need manual review, which improves the quality of the test results [36].
Go to :
DILUTION PARAMETERS
Because assay imprecision can increase considerably over time, correcting urinary dilution has become increasingly necessary. As hydration is a major pre-analytical confounder in urinalysis, many reference parameters have been introduced to assess urinary dilution and hydration. The most commonly used reference analytes are specific gravity, conductivity, and urinary creatinine determinations [585960]. Conductivity measurement has been integrated in flow cytometry instruments. Specific gravity can be measured using either refractometry or test strips. Table 2 summarizes the most important dilution parameters used in automated urinalysis.

Table 2
Currently used urinary dilution parameters in automated urinalysis
![]()
Go to :
MATRIX-ASSISTED LASER DESORPTION IONIZATION-TIME OF FLIGHT (MALDI-TOF) MASS SPECTROMETRY
MALDI-TOF mass spectrometry (MS) has been recently introduced in routine clinical microbiology laboratories. As the time needed for culture continues to hinder decision-making and the laboratory workflow, direct-from-sample characterization of the bacterial load constitutes a major advance. Several studies have explored direct analysis of urine samples using MALDI-TOF MS, thereby eliminating the time lag needed for pathogen identification [6162636465666768]. This technique has been suggested as a fast and reliable method for bacterial identification [69].
Initial studies combining urinary tract screening methods with direct application of MALDI-TOF MS in bacteriuria-positive samples have demonstrated direct pathogen identification sensitivity ranging from 67% to 86% [61647071]. These results mirror those of similar studies showing successful pathogen identification from pathogen-positive blood cultures [6172].
It is unclear whether MALDI-TOF MS can meet the demands of UTI diagnosis, given the need for screening to improve the yield of positive samples. For direct analysis of urine, initial sample preparation steps are necessary to remove cellular debris, WBCs, and mucus and to collect bacteria. In its current iteration, analysis of MALDI-TOF MS results is hampered by poly-microbial samples. Up to 77% of the catheter-associated UTIs are poly-microbial; therefore, improved algorithms for interpreting the spectra of bacterial combinations are needed for direct-from-urine testing of these samples [7374]. Additionally, the technique does not provide reliable information on antimicrobial susceptibility for frequently used antibiotics in UTI treatment [75]. Indirect approaches for antimicrobial susceptibility testing are under development and include the measurement of bacterial metabolic by-products in the presence of antibiotics to assess susceptibility.
Oviaño et al. [76] developed an automated MALDI-TOF MS-based assay for rapid, direct detection of carbapenemase-producing Enterobacteriaceae in clinical urine samples within 90 min of sample reception; carbapenemase activity is detected by MALDI-TOF MS analysis following reliable direct identification of gram-negative bacilli. In their study, bacteria were extracted from urine samples, carbapenem resistance was detected using imipenem as an antibiotic marker, and the results were automatically interpreted. Their assay yielded direct reliable identification in 91% of the samples and showed 100% sensitivity and specificity for detecting carbapenemase activity within 90 min of sample reception.
Go to :
LABORATORY-ON-A-CHIP
In view of the great need for the development of portable and cost-effective readers, pocket-sized colorimetric readers can be combined with dipsticks in a device that is able to transmit digital information via a smart phone, offering an integrated solution for detecting disease in areas with limited access to trained experts [77]. Advances in microfluidics have enabled the development of new chip-based assays, which will alter the field of automated urinalysis in the near future [78]. Alongside conventional urinalysis applications [79], integrated microfluidic chips have been described as a promising tool for measuring the concentration of bladder cancer cells in urine samples [80]. Similarly, microfluidic paper analytical devices have been designed and fabricated for evaluating bacteria known to cause UTIs (Escherichia coli) and sexually transmitted diseases (Neisseria gonorrhoeae) in human urine samples [81].
Go to :
CONCLUSIONS AND FURTHER PERSPECTIVES
Over the past two decades, automated urinalysis has undergone remarkable technical progress. Both microscopy- and flow cytometric-based instruments generate reliable results that are clinically useful, and automated test strip reading provides added value. Additional integration of existing technologies may further reduce turn-around times.
In the meantime, the consolidation of laboratories has led to a reduction in the number of laboratories and has thereby increased the physical distance between patient and laboratory; this trend creates a major pre-analytical challenge. Despite improvements in standardization [82], most of errors in urinalysis occurs outside of the analytical phase; pre-analytical steps, in particular, are much more vulnerable [83]. As analytical variation has been greatly reduced, more efforts need to be focused on the pre-analytical phase.
Go to :
 XML Download
XML Download