

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Group B streptococcus (GBS, Streptococcus agalactiae) is a β hemolytic gram-positive diplococcus that can asymptomatically colonize the gastrointestinal and the female genital tracts in healthy individuals [1].
GBS is a major causative pathogen of neonatal sepsis and meningitis and has been associated with preterm labor, prematurely ruptured membranes, chorioamnionitis, and puerperal and fetal infections [23]. Most early-onset neonatal infections are secondary to vertical transmission of infection from the colonized maternal genital tract and the rectum via fetal aspiration of bacteria. Therefore, the detection of GBS colonization in the genital tract of pregnant women and the administration of intrapartum antibiotic prophylaxis is important [4].
GBS has been reported as the leading infectious cause of early-onset neonatal sepsis and meningitis in the United States (US) and Europe since the late 1970s [5]. However, in Korea, GBS was not reported to be a major pathogen causing neonatal sepsis and meningitis until the late 1990s. However, recent concerns regarding GBS colonization are increasing with several reports showing GBS to be a major pathogen accounting for approximately 33% of invasive neonatal infections [67].
Reportedly, the GBS colonization rate in the gastrointestinal or the genital tracts of pregnant women in the US was 18.6–26.5% [8910], whereas this rate in pregnant Korean women was 2.0–11.5%, which was significantly lower than that in pregnant women in the US [11121314151617]. The various colonization rates in Korean women could be attributed to differences in patient characteristics of the study groups, study periods, and the culture methods used for GBS detection (Table 1). Blood agar is widely used to culture hemolytic GBS; however, selective chromogenic media for GBS provide more rapid and sensitive results. Two types of selective chromogenic media for GBS are the Granada (anaerobic) and the chromID Strepto B medium (aerobic) (CHROM-B), which is more convenient and sensitive than the Granada medium [18]. Recently, real-time polymerase chain reaction (PCR) techniques have been used to detect GBS. The PCR technique is highly sensitive and provides rapid results; however, it is expensive.
Table 1
Group B streptococcus colonization rates in Korea using different culture media

| Study | Duration & location | No. of participants | GA (wk) | Culture media | Colonization rate (%) |
|---|---|---|---|---|---|
| Kim et al. [11] | 2002.05–2003.04 | 58 | 35–37 | LIM broth, blood agar | 3.44 (2/58) |
| Pusan National Hospital | |||||
| Park et al. [12] | 1991.04–1992.08 | 153 | 24–42 | Todd-Hewitt broth, tryptose blood agar plates | 2.61 (4/153) |
| Severance Hospital | |||||
| Choi et al. [13] | 2000.01–2001.06 | 204 | 35–37 | Todd-Hewitt broth, sheep blood agar | 1.96 (4/204) |
| Inha Hospital | |||||
| Kim et al. [14] | 2005.03–2005.05 | 273 | >35 | Todd-Hewitt broth, sheep blood agar | 4.8 (13/273) |
| 3 obstetric clinics in Goyang-si and Paju-si | |||||
| Uh et al. [15] | 2008.08–2009.06 | 234 | Before delivery | New Granada Medium, Todd-Hewitt broth, sheep blood agar | 11.5 (27/234) |
| Yonsei University Wonju College of Medicine | |||||
| Oh et al. [16] | 2005.11–2006.04 | 667 | 35–37 | Todd-Hewitt broth, sheep blood agar | 6.3 (42/667) |
| 4 obstetric clinics in Goyang-si | |||||
| Hong et al. [17] | 2006.03–2007.12 | 4,045 (1,216+2,828) | 35–37 | 2006.03–2007.03 | 10.0 (121/1,205) |
| Seoul National University Bundang Hospital | Sheep blood agar | ||||
| 2007.03–2007.12 | 2007.04–12 | 4.0 (114/2,829) | |||
| Bombit Women's Medical Service | Todd-Hewitt broth, sheep blood agar |
The objectives of this study were to investigate the GBS colonization rate in pregnant Korean women using a selective chromogenic medium for GBS to study the characteristics of GBS-colonized pregnant women and their neonates. We analyzed the incidence of GBS-related complications in pregnancy and the incidence of early-onset neonatal sepsis.
Materials and methods
This study included pregnant women at >20 weeks' gestation who presented to the Inje University Busan Paik Hospital between January 2015 and December 2016. Women aged <20 years and those who were transferred to another hospital and did not deliver at Inje University Busan Paik Hospital were excluded. This study included 1,014 pregnant women and 1,158 neonates including 137 twin and 9 triplet births. Intrapartum antibiotic prophylaxis was administered at the onset of labor or following the rupture of amniotic membranes in women showing GBS-positive cultures or those in whom screening results were not available at the time [19]. Ampicillin-sulbactam (ampicillin 1 g, sulbactam 0.5 g) was administered intravenously every 6 hours as the primary prophylactic antibiotic. Women in whom allergy skin testing showed positive reactions to ampicillin without a history of anaphylaxis following the administration of penicillin or a cephalosporin, received intravenously administered cefazedone (first-generation cephalosporin, 1 g every 12 hours). Antibiotics were administrated until delivery or until cultures showed negative results. This study was approved by the Institutional Review Board (16-0119) of Inje University Busan Paik Hospital.
The specimens for GBS culture were obtained from the pregnant women at 35.0–37.0 weeks of gestation on an outpatient basis or from inpatient pregnant women at risk of threatened preterm labor. Women at risk of threatened preterm labor who did not deliver within 5 weeks underwent re-examination at 35.0–37.0 weeks. This study was performed based on the results of the re-examination. Physicians obtained the specimens from 2 sites: 1) the first specimen was obtained from the lower vagina using a sterile cotton swab without inserting a speculum and 2) another sterile cotton swab was inserted through the anus and gently rotated. Both swabs were transported separately in the Amies gel medium to the microbiology laboratory at Busan Paik Hospital.
Swabs transported in the Amies gel were inoculated directly onto the CHROM-B agar medium (chromID™ StreptoB agar, bioMérieux, Marcy l'Etoile, France) aerobically at 37°C for 18–24 hours. Pale pink-to-red colonies of GBS were confirmed using the VITEK2 system (bioMérieux).
The GBS colonization rate was identified based on GBS culture studies in 1,014 pregnant women. We compared the characteristics between the GBS-positive and negative groups. We analyzed characteristics of the pregnant women including mean age, gestational age at the time of sampling, parity and gravidity, body mass index (BMI), mode of delivery, history of preterm delivery, multifetal pregnancy, and gestational age at the time of delivery. Colonization rates were analyzed based on the site of specimen collection. The incidence of pregnancy-related complications was compared between the GBS-positive and negative groups. We analyzed pregnancy-related complications including preterm labor, preterm premature rupture of membranes (PPROM), preterm delivery, and uterine infection.
Preterm labor was defined as the onset of regular uterine contractions accompanying cervical changes based on the criteria recommended by Cunningham et al. [20]. PPROM was defined as the spontaneous rupture of fetal membranes before 37.0 weeks' gestation and before the onset of labor. Preterm delivery was defined as delivery occurring before 37.0 weeks. Deliveries occurring before 34.0 weeks were defined as early preterm deliveries and those occurring between 34.0–36.6 weeks were defined as late preterm deliveries. Chorioamnionitis and puerperal uterine infection were categorized as uterine infections. Chorioamnionitis was defined as a fever >38.0°C with accompanying leukocytosis, increased C-reactive protein (CRP) levels, uterine tenderness, and increased vaginal discharge with a foul odor. Puerperal uterine infection was defined as fever >38.0°C within 6 weeks after delivery accompanied by abdominal pain, uterine tenderness, and signs of inflammation such as leukocytosis. We assessed birth weight, intrauterine growth restriction (IUGR), neonatal death, 1-minute Apgar score <7, 5-minute Apgar score <7, clinical neonatal sepsis, and neonatal sepsis in all neonates (excluding stillborn neonates). Clinical neonatal sepsis was defined as a decreased neutrophil count, thrombocytopenia, increased CRP levels, and systemic signs of severe infection including fever or hypothermia, hypotension, metabolic acidosis, hypoglycemia, bradycardia or tachycardia, apnea, respiratory distress, lethargy, irritability, seizures, abdominal distention, vomiting, diarrhea, jaundice, petechiae, and/or bleeding. Neonatal sepsis was defined as signs of infection accompanied by proven bacteremia within the first 28 days of life. Early-onset sepsis occurs within 6 days of life and late-onset sepsis occurs between 7 and 28 days of life [521].
Data are presented as the incidence or mean±standard deviation. Statistical comparisons were performed using the independent Student's t-test, the χ2 test, and the Fisher's exact test. A P-value <0.05 was considered statistically significant. All statistical analyses were performed using the MedCalc® software (v 15.6.1, Frank Schoonjans, Ghent University, Gent, Belgium).
Results
1. Maternal clinical characteristics
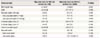
Among the 1,014 pregnant women studied, 117 were GBS positive; therefore, the GBS colonization rate was 11.6%. No statistically significant difference was observed between the GBS-positive and negative groups with respect to age, rate of nullipara or primigravida, BMI, multifetal pregnancy, and the rate of cesarean delivery (Table 2).
Table 2
Association between maternal clinical characteristics and group B streptococcus colonization

Gestational age at the time of sampling in the GBS-negative group (34.3±4.2 weeks) was lower than that in the GBS-positive group (35.2±3.6 weeks); however, this difference was statistically non-significant (P=0.059). Gestational age at the time of delivery in the GBS-negative group (36.1±3.7 weeks) was lower than that in the GBS-positive group (37.1±3.3 weeks, P=0.013).
No statistically significant difference was observed in the rate of prior preterm births between the GBS-positive and negative groups (12.8 vs. 7.6%, P=0.052). Additionally, no statistically significant difference was observed in the rate of positive GBS colonization between women with and without history of preterm births—18.1% of women with a history of preterm birth (15/83) were GBS-positive (P=0.052).
2. Group B streptococcus colonization sites in the group B streptococcus-positive group
Among the 1,014 pregnant women evaluated, in 44 patients, we obtained a single vagina-rectum swab for GBS culture during the early study period. In the remaining 970 women, we obtained both, a lower vaginal and a rectal swab. Among these 970 women, 110 showed positive culture results—in 16 (14.5%) only the lower vaginal swab showed positive results and in 47 (42.7%), both, the lower vaginal and the rectal swabs showed positive results (Table 3).

3. Maternal complications
The rate of preterm labor was 21.4% in the GBS-positive and 30.9% in the GBS-negative group (P=0.034). The rate of PPROM was 12.8% in the GBS-positive and 17.8% in the GBS-negative group (P=0.177) (Table 4). Of note, in the GBS-positive group, 8.3% of pregnant women developed preterm labor (25/297) and 8.6% showed PPROM (15/175). These rates were lower than the overall GBS-positive rate.
Table 4
Association between maternal complications and group B streptococcus colonization
The rate of preterm delivery in the GBS-negative group was higher than that in the GBS-positive group (43.6 vs. 33.3%, P=0.044). The rate of late preterm delivery in the GBS-negative group was lower than that in the GBS-positive group (21.4 vs. 21.9%, P=0.905). However, the rate of early preterm delivery in the GBS-negative group was higher than that in the GBS-positive group (21.7 vs. 12.0%, P=0.014).
No statistically significant intergroup difference was observed in the rate of chorioamnionitis and puerperal infection. Of note, in the GBS-positive group, 6% of pregnant women showed chorioamnionitis (4/67) and 11.1% showed a puerperal infection (1/9); however, these rates were lower than the overall GBS-positive rate.
4. Neonatal clinical characteristics
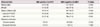
Among the 1,158 neonates studied, including 137 twin and 9 triplet births, 134 were born to GBS-positive women and 1,024 to GBS-negative women (Table 5). Neonates born to GBS-positive women showed a significantly greater mean weight (2.7±0.8 kg) than those born to GBS-negative women (2.5±0.8 kg) (P=0.002).
Table 5
Association between neonatal complications and group B streptococcus colonization
GBS, group B streptococcus; IUGR, intrauterine growth retardation.
a)Clinical neonatal sepsis indicated by abnormal laboratory parameters including elevated C-reactive protein, leukocytosis, leukopenia and thrombocytopenia combined with abnormal clinical parameters suspicious for severe systemic infection
No significant intergroup differences were observed with regard to neonatal deaths, IUGR, clinical neonatal sepsis, and neonatal sepsis. The occurrence of the 1-minute Apgar score <7 in neonates born to GBS-positive women was significantly lower (11.2%, 15/134) than in neonates born to GBS-negative women (21.5%, 220/1,024, P=0.004). There was no significant difference in the rate of neonates with the 5-minute Apgar score <7 between the groups (P=0.792).
We observed 358 clinical episodes of neonatal sepsis among 1,158 neonates. No significant differences were observed between neonates born to GBS-positive and GBS-negative women with respect to the incidence of clinical neonatal sepsis (29.9 vs. 31.1%, P=0.854). Neonatal sepsis with proven bacteremia was diagnosed in 21 (1.81%) neonates; however, no significant intergroup difference was observed in the incidence of neonatal sepsis (P=0.726). Neonatal sepsis caused by GBS bacteremia occurred in 1 neonate. However, this was a case of late GBS-induced neonatal sepsis with positive blood cultures observed on the 28th day of birth, and the neonate was born to a GBS-negative woman (Fig. 1).

Discussion
In the 1970s, GBS was reported to be the leading infectious cause of early neonatal morbidity and mortality in the US. Since then, significant efforts have been made to reduce neonatal morbidity and mortality, and guidelines have been established by the American College of Obstetricians and Gynecologists and the Centers for Disease Control and Prevention (CDC) in 1996 and by the American Academy of Pediatrics in 1997 for the use of intrapartum antibiotic prophylaxis to prevent perinatal GBS disease. The CDC recently published revised guidelines for the perinatal prevention of GBS disease, which recommend screening rectovaginal cultures for GBS at 35–37 weeks' gestation, or at <37 weeks' gestation in women with threatened preterm labor. The guidelines also recommend intrapartum antibiotic prophylaxis for women identified as GBS carriers or pregnant women with an unknown GBS status at the onset of labor. Risk factors necessitating antibiotic prophylaxis are: delivery at <37 weeks' gestation, intrapartum body temperature ≥38.0°C, or rupture of membranes for ≥18 hours. Owing to these preventive measures, the incidence of GBS-induced early-onset neonatal sepsis has markedly declined over the past 15 years from 1.7 cases per 1,000 live births in the early 1990s to 0.34–0.37 cases per 1,000 live births in recent years [19]. A Korean nationwide survey investigating the causative organisms of neonatal sepsis determined that GBS accounted for only 0.5% of all cases of neonatal sepsis [6]. However, reports have shown that the occurrence of GBS-induced neonatal disease has increased after 2000. Lee et al. [7] also reported that GBS was a major causative pathogen in invasive neonatal infections among infants aged <3 months. Following an increase in the occurrence of neonatal GBS disease in Korea, there is growing concern regarding GBS colonization in pregnant Korean women, and updated information is needed regarding the maternal GBS colonization rate among pregnant Korean women.
Reportedly, the GBS colonization rate in pregnant Korean women was 2.0–3.4% [111213]. However, several studies have noted an increase in this rate after 2005. Kim et al. [14] reported a study in which 13 of 273 pregnant women were positive for GBS, indicating a GBS colonization rate of 4.8%. Uh et al. [15] reported a study in which 27 of 234 pregnant women were positive for GBS, indicating a GBS colonization rate of 11.5%. Oh et al. [16] studied 667 pregnant women and reported a GBS colonization rate of 6.3% (42/667). Hong et al. [17] performed a large-scale study at 2 centers and reported a difference in results between the 2 locations in that 121 of 1,205 pregnant women at 1 center were positive for GBS (colonization rate 10.0%) and 114 of 2,829 pregnant women at the other center were positive for GBS (colonization rate 4.0%). In the present study, the GBS colonization rate with universal prenatal GBS screening was 11.6% (117/1,014). This rate is higher than that reported by previous studies in Korea. Owing to the low GBS colonization rate previously reported in pregnant Korean women, universal prenatal GBS screening was not considered obligatory. Based on the results of this and a few recent Korean studies, further discussions are needed regarding the introduction of a system in Korea for the identification of prenatal GBS colonization and the administration of intrapartum antibiotic prophylaxis based on CDC guidelines.
GBS can colonize both, the gastrointestinal and the genital tracts. Among the 110 GBS-positive pregnant women (based on vaginal or rectal cultures), 94 (85.5%) showed positive rectal and 63 (57.3%) showed positive vaginal cultures. Although the gastrointestinal tract is the primary site of GBS colonization, vaginal cultures are also important because obtaining only vaginal cultures can result in an underestimation of the GBS colonization rate. Therefore, obtaining both, vaginal and rectal cultures is strongly recommended [1719]. In this study, 47 (42.7%) pregnant women showed positive rectal and negative vaginal cultures (Table 4).
The selection of appropriate GBS culture media is important for the rapid and accurate detection of GBS colonization. CHROM-B is a selective chromogenic GBS screening medium. Using CHROM-B, GBS colonies appear pink-to-red, whereas other bacteria are inhibited or appear as blue or colorless colonies. CHROM-B shows a higher sensitivity than blood agar (90.0 vs. 66.7%) under the same conditions (timing of culture and similarity of culture specimens) [1822]. The study by Uh et al. [15], which reported a high GBS colonization rate (11.5%), used the New Granada Medium (NGM), a selective chromogenic medium for GBS. In that study, 1 swab specimen was inoculated on self-produced or commercially obtained NGM agar for 24 hours anaerobically. Subsequently, orange colonies were subcultured to Todd–Hewitt broth for 18–24 hours and then subcultured to sheep blood agar. Subsequently, the growth of γ or β hemolytic colonies was confirmed using the Christie-Atkins-Munch-Petersen and latex agglutination tests. Another swab specimen was inoculated in a self-produced NGM tube for 24 hours anaerobically. In our study, the culture specimen was inoculated directly onto commercial CHROM-B aerobically at 37°C for 18–24 hours. Subsequently, pale pink-to-red colonies were confirmed as GBS. The specimen was inoculated directly onto CHROM-B and a single-step culture was performed; thus, the culture results were available more rapidly and were more sensitive than those using NGM. Thus, GBS-selective culture media should be used for GBS screening. However, it is unclear whether our results reflect a true increase in the colonization rate of all pregnant Korean women or whether the high rates reflect a higher GBS detection rate owing to the use of GBS-selective media. Additional studies are needed to clarify this observation.
A previous study suggested that a first pregnancy was a significant risk factor (odds ratio 2.32, 95% confidence interval 1.12–4.81) for GBS colonization among pregnant women in Korea [23]; however, we were unable to demonstrate an association between a first pregnancy and the GBS colonization rate.
Several studies have reported significantly higher rates of preterm labor, PPROM, and preterm birth in GBS colonized pregnant women [242526]. In contrast, Kubota [27] reported no statistically significant association between vaginal GBS colonization and preterm labor or PPROM. A recent systemic review reported no significant association between GBS colonization in pregnant women and preterm labor [28]. This issue remains controversial, and there is currently no consensus regarding the effect of GBS colonization on preterm labor and PPROM. In the present study, no statistically significant association was observed between the GBS colonization status and PPROM in 1,014 pregnant women. However, the rate of preterm labor in the GBS-positive group was significantly lower than that in the GBS-negative group (21.4 vs. 30.9%, P=0.034). The gestational age at delivery in the GBS-positive group was not lower than that in the GBS-negative group. No significant intergroup difference was observed in the incidence of chorioamnionitis and puerperal infection. In this study, the rate of preterm delivery before 34 gestational weeks was significantly lower in the GBS-positive group. We suspect that various biases might have affected preterm delivery rates because a greater number of preterm women were included in the GBS-negative group.
Among the 1,158 neonates born to the pregnant women in this study, 358 showed symptoms of clinical sepsis, although only 21 showed positive blood cultures. Moreover, no GBS-induced early-onset neonatal sepsis was reported in either group. We could not definitively conclude whether the absence of GBS-induced early-neonatal sepsis was secondary to the administration of intrapartum prophylactic antibiotics or other effects. Additionally, we could not analyze GBS-related neonatal complications in this study.
In conclusion, a long-term multicenter study including even primary clinics is needed for evaluation of an accurate GBS colonization rate in pregnant Korean women. We suggest close monitoring of GBS-related neonatal disease in Korea. Additionally, it is important to establish guidelines for the screening of pregnant women for GBS and the use of intrapartum antibiotic prophylaxis in GBS-positive pregnant Korean women.
 XML Download
XML Download