

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary computed tomography angiography (CCTA) has been widely used as a non-invasive assessment in patients with stable coronary artery disease (CAD). Its utility is attributed to intuitive visualization of the coronary artery lumen, which has been deemed highly sensitive for either detecting an obstructive coronary lesion in stable CAD1 or preclusion from acute coronary syndrome in the emergency department setting.2 Advancement in imaging technology and constant clinical validation in recent years have justified the role of CCTA in the diagnostic approach in patients with suspected CAD.3 Although there are some concerns and disputes about the appropriate use and interpretation of CCTA, additional use of CCTA was found to play a positive role in the assessment and management of CAD.3 However, further investigation is needed to ascertain how general physicians or cardiologists can utilize CCTA findings in decision-making in the cardiac catheterization laboratory. A recent consensus document drew recommendations for future strategies according to degrees of maximal coronary stenosis on CCTA.4 However, these recommendations were not based on objective validation. In particular, moderate stenosis on CCTA may be a worrisome and confusing finding for physicians, as it implies obstructive CAD, but not severe anatomical stenosis. Therefore, we sought to investigate the diagnostic accuracy of CCTA in patients with segments with moderate stenosis alone on CCTA. The CCTA results were compared with the results of invasive coronary angiography (ICA), which was utilized as a confirmative study.
MATERIALS AND METHODS
Study population
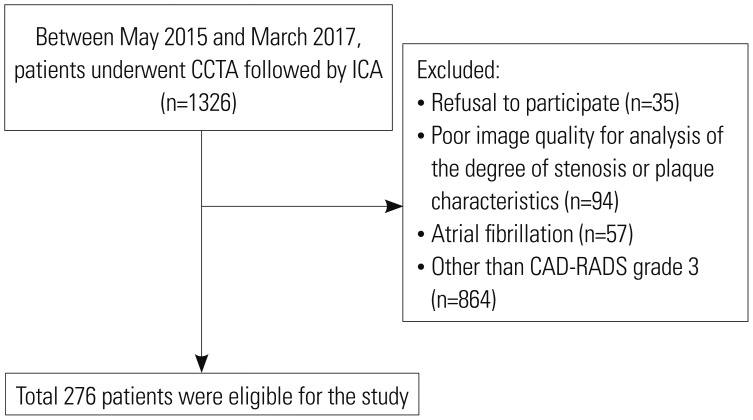
A prospective, real-world registry was used for the consecutive enrollment of all patients with suspicious, stable ischemic heart disease who underwent ICA for the diagnosis of CAD within 3 months after CCTA was performed. Data from 1326 patients were added to the registry between May 2015 and March 2017. We included 276 individuals who were classified as Coronary Artery Disease Reporting and Data System (CAD-RADS) grade 3. Participants had one or more segments with a maximal degree of stenosis of 50–69% in diameter in the epicardial arteries, excluding the left main trunk (Fig. 1).4 Pretest probability was estimated using the Duke Clinical Score.5 The study protocol was approved by the Institutional Review Board of the two institutions (1-2013-0084). Written informed consent was obtained from all patients.
Acquisition and assessment of coronary computed tomographic angiography
CCTA images were acquired with conventional 64-detector-row scanners (SOMATOM Sensation 64, Siemens, Forchheim, Germany; Philips Brilliance 64, Philips Medical System, Best, the Netherlands; LightSpeed VCT and CT750 HD, GE Healthcare, Waukesha, WI, USA) and next generation 128 or 256-detector-row scanners (SOMATOM Definition Flash, Siemens; Revolution CT, GE Healthcare). The protocol recommended by the Society of Cardiovascular Computed Tomography at the time each scan was used as the standard protocol for image acquisition at the two institutions.6 One to two hours before the CCTA examination, oral metoprolol was administered to patients with a baseline heart rate (HR) ≥70 beats/min in the absence of any contraindications. Sublingual nitroglycerin (0.3 mg to 0.6 mg) was administered immediately before contrast injection. Patients with a regular HR underwent CCTA scanning under prospectively electrocardiogram (ECG)-triggered axial mode. Spiral mode, if offered, was utilized if the HR was <60 beats/min. Retrospectively ECG-gated scanning was applied during image acquisition if a patient had frequent irregular beats or a higher HR. A bolus of 60 mL to 80 mL of iopamidol was injected into the antecubital vein using a triple-phase injection method, followed by 30 mL of 30% blended iopamidol and a 20 mL saline flush at a 5 mL/s flow rate. The optimal delay times were determined using automatic evaluation of the enhancement of the ascending aorta.
The coronary arteries were divided into 15 segments following the defined tree model.7 Segments with a >2.0 mm diameter were visually evaluated at a core laboratory (Severance Cardiovascular Hospital, Seoul, Korea) by a single experienced radiologist (BWC, 17 years of experience) who was blinded to patient and coronary angiographic information. A cardiologist (CK, 4 years of experience) assessed reliability and reproducibility in 30 randomly chosen patients (55 lesions). Any of the following available post-processed reconstructed images were used for the assessment of coronary artery stenosis: two-dimensional axial, three-dimensional maximal intensity projection, multi-planar reformat, cross-sectional analysis, or the volume-rendered technique using a three-dimensional computed tomography (CT) workstation (Wizard, Siemens Medical Solutions, Erlangen, Germany).8
The degree of stenosis was classified by a quantitative stenosis grading system.4 CAD-RADS recommends reporting stenosis from grade 0 (absence of atherosclerosis) to 5 (presence of at least one total occlusion) based on the maximal coronary stenosis. All coronary plaques with maximal stenosis at each segment were classified into one of three categories: calcified (plaque with high CT attenuation compared to the contrast-enhanced lumen), mixed (non-calcified and calcified elements in a single plaque), or non-calcified plaque (plaque with lower CT attenuation compared to the contrast-enhanced lumen without any evidence of calcification).910 Overall imaging quality was also qualitatively assessed as follows: 1) optimal images, clear delineation without motion artifact, minor motion artifacts, or blurring, but diagnostic in quality, without phase change; 2) suboptimal images, moderate to severe artifact or blurring, but evaluable, using different phase or additional manual reconstruction; and 3) unevaluable images, which were excluded in the current study.11 We used the segment involvement score (SIS), which indicates the number of segments (per patient) with any coronary plaque. We calculated calcified and non-calcified SISs separately by counting the numbers of calcified and non-calcified plaques, respectively.12
Invasive coronary angiography and revascularization
All eligible patients underwent ICA a median of 17 days (interquartile range 8–41 days) after the initial CCTA examination. The degree of coronary stenosis at each segment was visually assessed by interventional cardiologists in the catheterization laboratory. Analysts at an independent core laboratory (Cardiovascular Research Center, Seoul, Korea), who were blinded to the findings of the initial assessment and patient information, reviewed the ICA findings. Comparing the findings of ICA and CCTA, the analysts verified stenosis of any corresponding lesion identifiable on CCTA. Discrepant results were evaluated by the investigators (CK, SJH, and MKH) who reached a consensus concerning the degree of stenosis while continuing to be blinded to patient information. Quantitative coronary angiography analysis was also performed in 30 randomly chosen patients using an offline computerized quantitative coronary angiographic system (CASS system, Pie Medical Instruments, Maastricht, the Netherlands) for assessment of agreement with visual estimation. The minimal lumen diameter and reference diameters of coronary lesions were measured in the view with the narrowest lumen and the least amount of foreshortening by comparison to the diameter of a guidance catheter from diastolic frames in a single, matched view. We compared the CCTA- and ICA-derived diagnoses for each patient. The diagnoses were analyzed and confirmed as concordant at the patient level if the degree of stenosis was matched for all major epicardial arteries. The CCTA-derived diagnosis was defined as under-diagnosis if the maximal stenosis of a vessel or segment determined by ICA was ≥70% of the diameter stenosis at the same location on CCTA. Correspondingly, the CCTAderived diagnosis was defined as over-diagnosis if the maximal stenosis was less than 50% of the diameter stenosis determined by ICA. At the patient-level, under-diagnosis of CCTA was defined as greater numbers of vessels with stenosis ≥50% or the presence of stenosis ≥70% in any vessels; over-diagnosis was defined as fewer numbers of vessels with stenosis ≥50% or no stenosis ≥50% in any vessels.
Statistical analysis
Categorical data are expressed as numbers (%) and were analyzed with chi-square statistics or Fisher's exact test. Continuous variables are expressed as medians (interquartile range) because of a skewed distribution. To compare differences in diagnostic concordance, patients were categorized by quartiles of calcified or non-calcified SIS and Agatston calcium score. A generalized linear mixed model was used to determine under- or over-diagnosis of moderate stenosis found on CCTA, considering the random effect of vessel-level and patient-level clustering. All variables with a p value <0.10 were entered into the multivariate model, and backward elimination was applied as sequentially deleted non-significant interactions with the largest p values one at a time to obtain a parsimonious final model. Cohen's kappa13 and intraclass correlation coefficient14 were used for assessment of the agreement between CCTA interpreters and between visual and quantitative coronary angiography-derived assessment of coronary stenosis, respectively. All statistical analyses were performed using R statistical software (version 3.3.2; R Foundation for Statistical Computing, Vienna, Austria). All statistical analyses were conducted as two-sided. p values <0.05 were considered indicative of statistical significance.
RESULTS
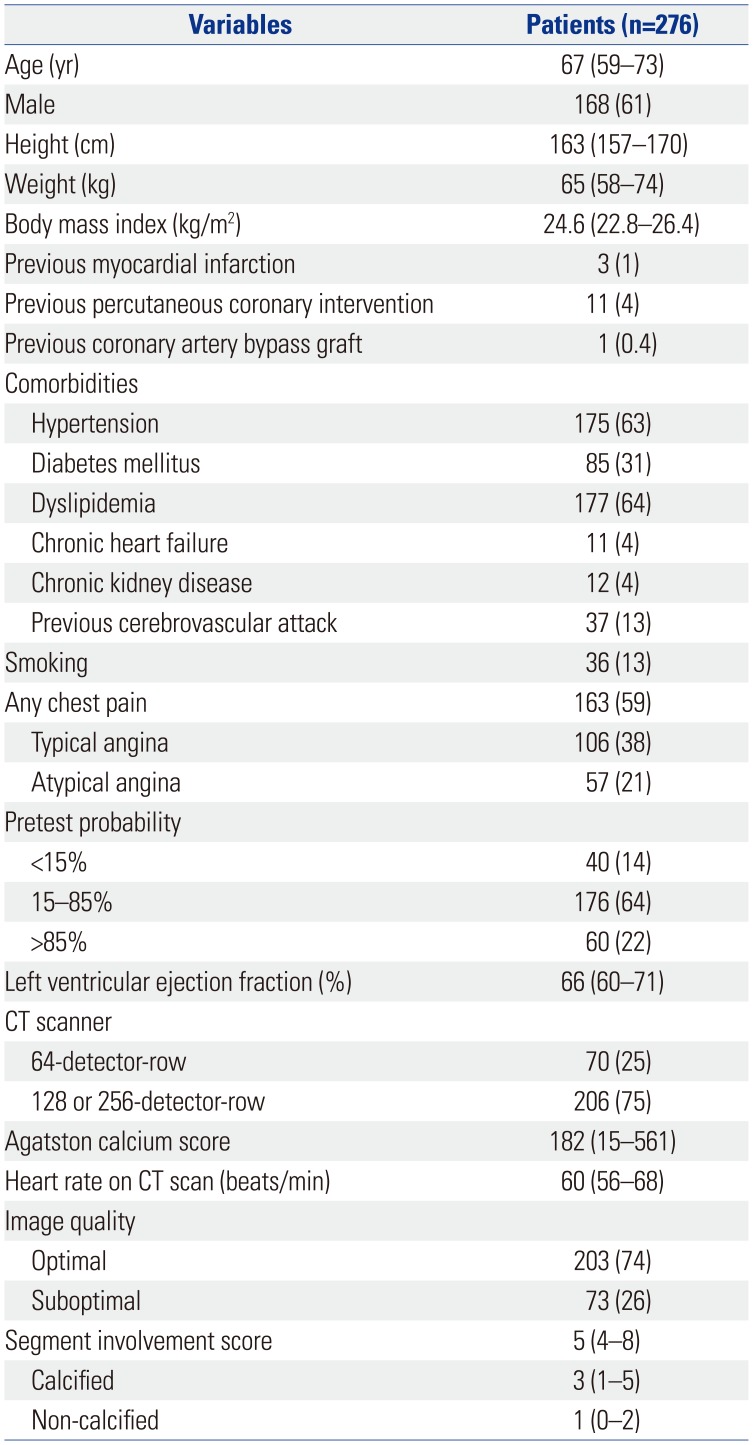
Baseline characteristics of the 276 enrolled patients are described in Table 1. Three-fourths of the patients underwent evaluation in next generation CT scanners and obtained optimal quality CCTA imaging.
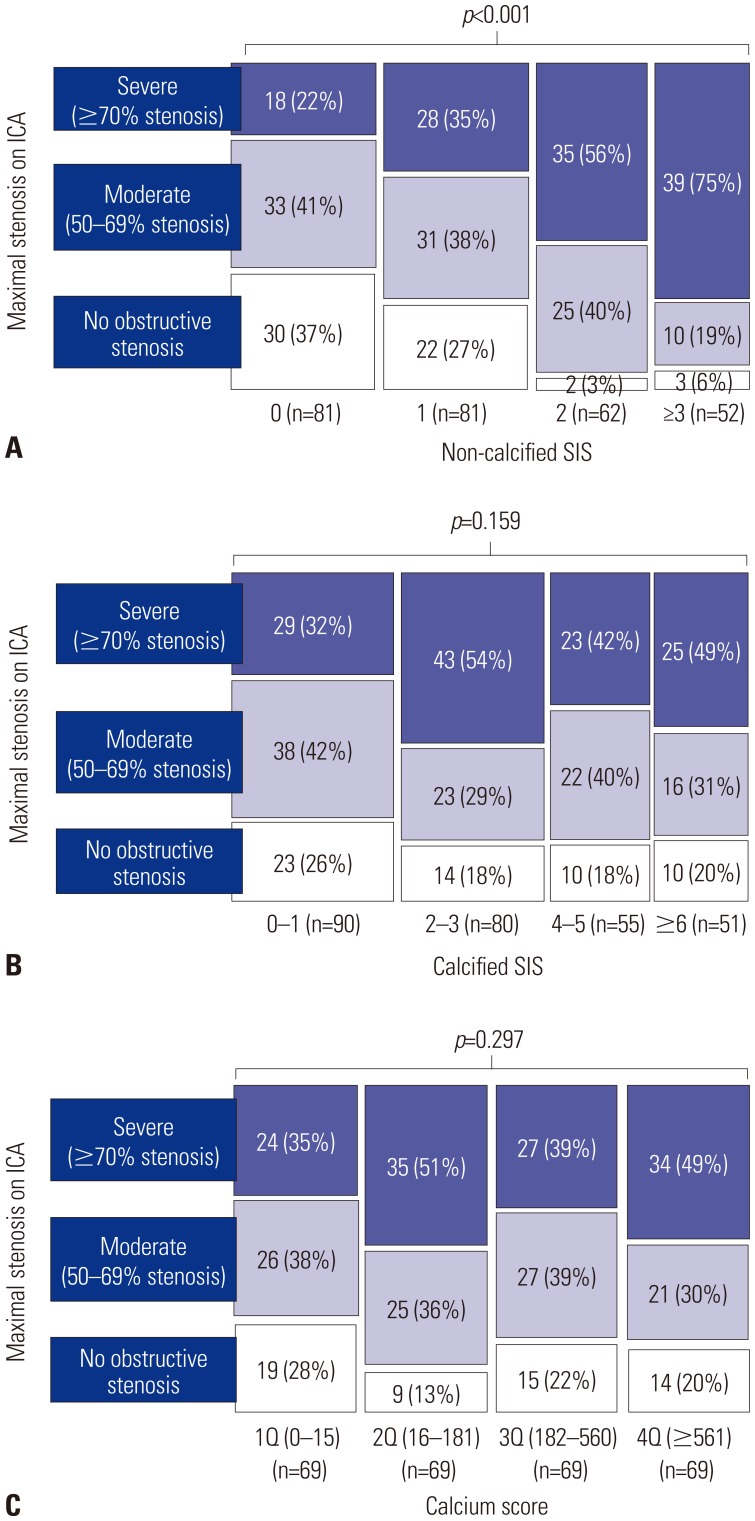
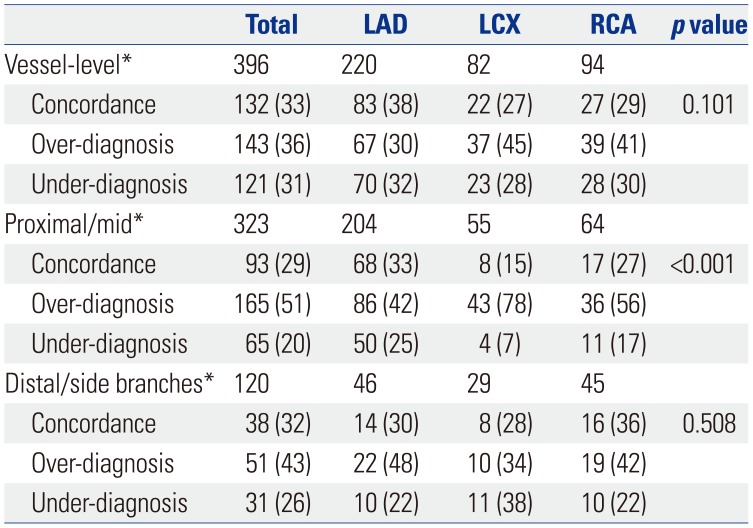
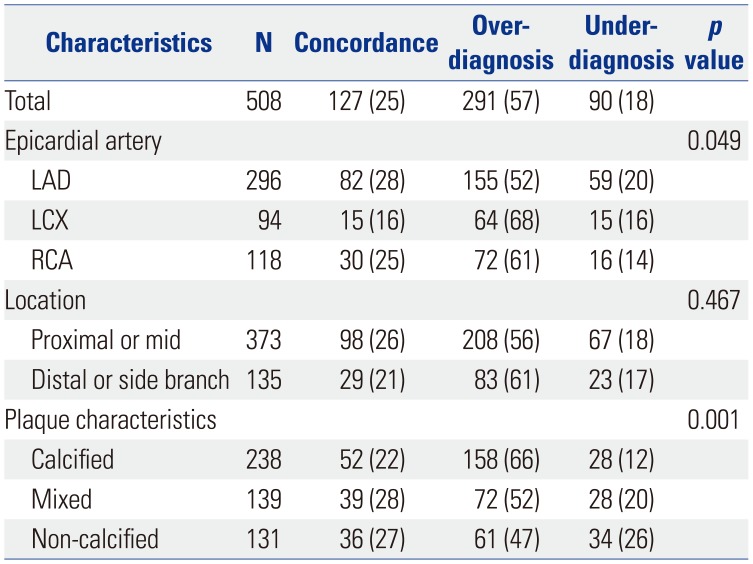
The intra- (κ=0.86) and inter-observer (κ=0.75) agreements for CCTA grading was good, and visual estimation of coronary stenosis was highly reliable, compared with quantitative coronary angiography [intraclass correlation coefficient 0.94, 95% confidence interval (CI) 0.89–0.96]. Patient-level analysis revealed that diagnostic concordance, which indicates the correct diagnosis of the presence of moderate stenosis in all three vessels, was found in only 50 (18%) patients. Among the 174 patients who were diagnosed with single-vessel disease on CCTA, 46 (26%) patients had a confirmed concordant diagnosis by ICA and 44 (25%) patients had no obstructive CAD (Table 2). In 102 patients suspected to have stenosis in two or more vessels on CCTA, only 4 (4%) patients had a confirmed concordant diagnosis by ICA. Furthermore, more than half of the patients who were assumed to have multi-vessel disease by CCTA had a confirmed under-diagnosis by CCTA, compared to the ICA findings. The proportions of under-diagnosis or severe stenosis by ICA were significantly higher as the number of diseased vessels with CCTA-identified stenosis increased (p<0.001) (Fig. 2). Per-vessel analysis showed that one-third of the vessels that were suspected to have moderate stenosis on CCTA had a similar degree of stenosis on ICA, and 36% and 31% of the vessels were at the risk of over-diagnosis and under-diagnosis, respectively (Table 3). Per-segment analysis showed that the overall diagnostic concordance was 25% among segments with moderate stenosis on CCTA (Table 4). Over-diagnosis of CCTA was more frequently found in the left circumflex artery (68%) than other vessels (52% in the left anterior descending artery and 61% in the right coronary artery, p=0.049). Compared to mixed (28%) or non-calcified (27%) plaque, calcified plaque had lower diagnostic concordance (22%, p=0.001), which was mainly attributed to a higher incidence of over-diagnosis. Also, the degree of stenosis of non-calcified plaques (26%) was more frequently underestimated than that of calcified (12%) or mixed plaque (20%) (Table 4). A higher burden of non-calcified plaque, assessed by SIS, was correlated with an increased risk of severe stenosis by ICA (Fig. 3). At least one segment with severe stenosis was found by ICA in 75% of patients who had ≥3 non-calcified SIS and in 22% of patients who lacked noncalcified plaque on the coronary tree (p<0.001). While assessment of calcified plaque burden, such as calcified SIS or calcium score, did not have an influence on diagnostic accuracy.
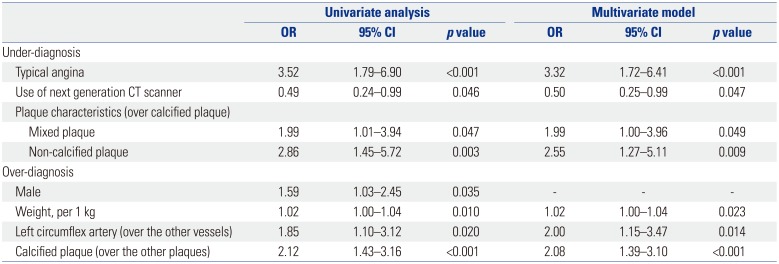
Risk factors for under-diagnosis or over-diagnosis of CCTA at the segment of moderate stenosis on CCTA are shown in Table 5. The presence of the typical symptoms of angina [odds ratio (OR) 3.32, 95% CI 1.72–6.41, p<0.001] and mixed (OR 1.99, 95% CI 1.00–3.96, p=0.049) or non-calcified plaque (OR 2.55, 95% CI 1.27–5.11, p=0.009) were independently correlated with a higher incidence of under-diagnosis. Use of a next generation CT scanner lowered the incidence of under-diagnosis (OR 0.50, 95% CI 0.25–0.99, p=0.047). Increased body weight (OR 1.02, 95% CI 1.00–1.04, p=0.023), left circumflex artery (OR 2.00, 95% CI 1.15–3.47, p=0.014), and calcified plaque (OR 2.08, 95% CI 1.39–3.10, p<0.001) were identified as independent factors affecting the possibility of over-diagnosis of CCTA in multivariable analysis.
DISCUSSION
This study investigated the clinical implications of moderate stenosis on CCTA. Current guidelines recommend functional assessment for moderate stenosis in patients with stable ischemic heart disease.4 Moreover, a CCTA diagnosis of moderate stenosis would be provisional and require further investigation using another non-invasive, functional assessment before coronary catheterization. When considering cardiac catheterization, physicians may have difficulty interpreting CCTA findings. For example, there could be confusion as to whether CCTA-identified moderate stenosis would reliably reflect moderate risk and underestimate the actual risk of severe stenosis in need of revascularization, or vice versa. This has been a gray zone in the diagnostic decision process for ischemic heart disease until now.
Our findings highlighted the aforementioned concerns about the indeterminacy of CCTA-identified moderate stenosis, which poorly matched with the degree of anatomical stenosis determined by ICA. Only 18% of patients had diagnostic concordance in regards to the degree of stenosis and extent of diseased vessel between CCTA and ICA. More than 50% of patients had a more severe degree of stenosis or more vessels with obstructive lesions on ICA, compared with CCTA findings. The limited capabilities of CCTA for delineation of coronary lumen and for prediction of the need for revascularization were previously demonstrated.81516
Other studies, on the other hand, have insisted that CCTA may provide sufficient specificity and sensitivity for the diagnosis of obstructive CAD.11718 These trials demonstrated positive predictive value of stenosis >50% in vessel-level analysis ranging between 51%17 and 83%,1 which was widely dispersed across to the trials. Another study using a dual-source CT scanner demonstrated that 39–50% of segments suspected to have moderate stenosis on CCTA had a similar degree of stenosis on ICA.19 The authors insisted that most segments were categorized within a 1-grade discrepancy, which contained a wide range of stenosis between 25% to 89%. In addition, their study included a small number of patients (n=84), included all severities of stenosis, and did not demonstrate how the diagnostic discordance at each segment would impact the diagnosis at the patient-level. Meanwhile, another compelling diagnostic tool, CCTA-derived fractional flow reserve has been shown to have clinical utility for diagnosis of myocardial ischemia in intermediate stenosis without noticeably altering the sensitivity of CCTA.20
If diagnosis is not highly accurate at each segment level, the possibility of diagnostic discordance may be exponentially increased at the patient level as the number of plaques to be evaluated was increased on CCTA. In the present study, only 4% of patients who were diagnosed with multi-vessel disease on CCTA had CCTA findings that were completely concordant with ICA findings. Furthermore, the presence of any severe stenosis was found more frequently as the number of vessels with moderate stenosis or non-calcified plaques increased.
Although the ability of CCTA to determine the exact degree of stenosis per segment is limited, CCTA may have a benefit in the estimation of overall atherosclerotic burden of the coronary tree, even when compared with functional assessment and ICA. Total plaque burden, especially non-calcified plaque, on the coronary tree may have clinical implications for risk stratification of patients with the possibility of severe stenosis. CCTA-identified overall plaque burden was revealed to have independent value for prediction of future cardiac events.21 Calcium scoring is a surrogate for plaque burden and has been well established to estimate the risk of future cardiac events.2223 Calcification is associated with advanced stage atherosclerosis, and it is most commonly found on fibrocalcific plaques, which are at low risk for rapid progression.24 However, non-calcified plaque burden, which was found to have more influence on the possibility of severe stenosis in our study, was proposed to be a better predictor for myocardial ischemia than calcium score or stenosis severity.25 Because CCTA tends to underestimate the size of non-calcified plaques and overestimate that of calcified plaques due to calcification-caused artifacts, a higher burden of non-calcified plaques may be interpreted as a high risk finding for the presence of more severely stenotic lesions.26 The CAD-RADS4 consensus mentioned only the degree of maximal coronary stenosis, but not overall plaque burden, in consideration of the diagnostic process for patients presenting with chest pain. Considering the limited reliability of CCTA-identified stenosis severity, physicians should be cautious when applying the suggested recommendations to daily clinical practice. Instead, the interpretation of CCTA findings should be individualized, and physicians should use clinical risk factors or another non-invasive assessment, or proceed to cardiac catheterization for treatment decisions.
Our study had several limitations. First, we validated CCTA-identified moderate stenosis in comparison with the degree of anatomical stenosis assessed by ICA. Because the functional significance of coronary stenosis may not be determined solely by ICA, further functional evaluation is required for the decision of revascularization in some cases. However, our study focused on the diagnostic reliability of the anatomical assessment of CCTA. The degree of maximal stenosis assessed by CCTA may be an insufficient evaluation to differentiate patient risk and to direct future investigation in clinical practice. Another functional test may be required for the decision of revascularization. However, its actual utility in clinical practice should be addressed in another study. Second, we used visual estimation to assess the degree of stenosis in both ICA and CCTA. Visual estimation is a common and comparable method for evaluation of stenosis severity in both ICA27 and CCTA19 in clinical practice. We found that visual assessment of ICA was also reliable compared with quantitative coronary angiography in randomly selected patients. Third, the diagnostic accuracy of CCTA may not be interpreted as the result in the overall patients who used CCTA as a non-diagnostic assessment because our prospective registry only enrolled the patients whose ICA information was available. The clinical reasons for cardiac catheterization, such as clinical suspicion or high probability of CAD, may reflect a higher prevalence of severe CAD in selected patients. However, 22% of the patients in our study had a high pretest probability, which did not impact the diagnostic concordance.
In conclusion, CCTA-identified moderate stenosis may be limited in estimating the exact degree of anatomical stenosis assessed by ICA. CCTA-identified stenosis per se may not be appropriate for predicting exact degree of coronary stenosis, although a high burden of non-calcified plaque on a coronary tree may increase the risk of significant coronary stenosis.


 XML Download
XML Download