

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence and mortality of epithelial ovarian cancer have continuously increased in Korea.123 Epithelial ovarian cancers are classified according to histologic subtypes into high-grade serous carcinoma (HGSC), clear cell carcinoma, endometrioid carcinoma, mucinous carcinoma, low-grade serous carcinoma (LGSC), and carcinosarcoma. According to the Korean Cancer Registry, histologic subtypes other than HGSC (non-HGSC) comprised more than half of the epithelial ovarian cancer cases in 2012. Furthermore, the incidence of clear cell carcinoma has significantly increased across all age groups in Korea.4
Although the prognosis and underlying carcinogenesis of epithelial ovarian cancer histologic subtypes are different, current treatment guidelines are the same for all. In previous studies, histologic subtype was identified as an independent prognostic factor. Among patients with advanced ovarian cancer, those with a non-HGSC subtype were deemed to have a relatively poor prognosis, compared with HGSC, due to resistance and reduced sensitivity to standard chemotherapy.567891011 Several studies have evaluated subtype-specific treatment of advanced ovarian cancer to improve the survival of patients with non-HGSC. However, these studies were performed only in patients who underwent primary debulking surgery (PDS).12131415
For advanced-stage ovarian cancer, neoadjuvant chemotherapy (NAC) and interval debulking surgery (IDS) have been proposed based on two randomized, controlled, phase III trials demonstrating no inferiority of IDS compared with PDS for the treatment of advanced ovarian cancer.1617 Responses to chemotherapy and clinical/surgical outcomes after the administration of NAC have been widely studied, mainly focusing on HGSC. As non-HGSC is now considered a different disease entity from HGSC, controversy remains as to whether the criteria used for NAC in non-HGSC should be the same as those for HGSC and whether the same chemotherapy regimen used for HGSC should be applied for non-HGSC.
We applied the same criteria and the same chemotherapy regimen for NAC regardless of histologic subtypes. The aim of this study was to evaluate the survival difference between patients with non-HGSC versus HGSC advanced ovarian cancer treated with NAC.
Go to : 
MATERIALS AND METHODS
We performed a retrospective analysis of medical records of 843 patients diagnosed with epithelial ovarian cancer from January 2006 to September 2017 at Yonsei Cancer Hospital. The present study was approved by the Institutional Review Board (IRB) of Severance Hospital at Yonsei University College of Medicine (IRB no. 4-2018-0518).
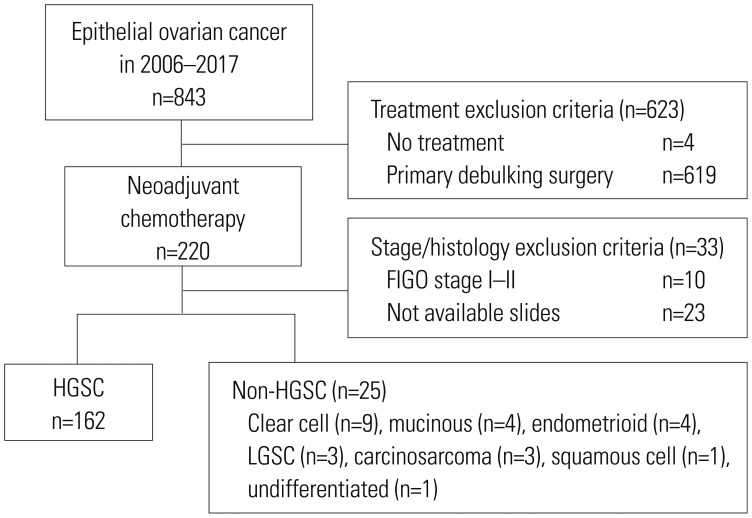
The inclusion criteria were as follows: 1) histologically confirmed diagnosis of epithelial ovarian cancer, 2) International Federation of Gynecology and Obstetrics (FIGO) stage III or IV epithelial ovarian cancer, 3) treatment with at least one cycle of NAC, and 4) availability of medical records and pathology slides. Fig. 1 shows a flow diagram of the study population. Of the 843 patients examined during the study period, we excluded 4 patients who refused treatment and 619 patients who underwent PDS. Of 220 patients who received more than one cycle of NAC, 10 patients with FIGO stage I or II and 23 patients without available pathologic slides for review were excluded. The remaining 187 patients (HGSC, n=162; non-HGSC, n=25) were included in this study.
All patients underwent CT and PET/CT as preoperative imaging workup. After patients were clinically diagnosed as having FIGO stage III or IV, the pathologic diagnosis of epithelial ovarian cancer was made by cytologic evaluation of ascites/pleural effusion, image-guided aspiration biopsy, and diagnostic laparoscopic/laparotomy biopsy. Our institution applied the following selection criteria for the use of NAC as the primary treatment strategy regardless of histologic subtypes:18 1) pulmonary and/or hepatic parenchymal metastases were observed on initial imaging studies, 2) patients had poor performance status and high operative risk due to medical comorbidities, or 3) optimal debulking surgery (residual disease measuring 1 cm or less) was unsuitable due to high tumor burden (Fagotti score ≥8).19
All patients received taxane-platinum combination chemotherapy. Conventional surgical procedures consisted of total hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and pelvic/para-aortic lymphadenectomy. Radical surgeries included bowel resection, diaphragm/peritoneal surface stripping, splenectomy, liver resection, partial gastrectomy, partial cystectomy/ureteroneocystostomy, cholecystectomy, and/or distal pancreatectomy. All surgical procedures were performed by one of five gynecologic oncology surgeons at a single institute.
The following data were extracted from patient medical records: age, body mass index (BMI), cancer antigen (CA)-125 levels, FIGO stage, tumor histology, American Society of Anesthesiologists (ASA) score, performance of radical surgery, residual disease after IDS, and chemotherapy regimen. Radiologic evaluation was performed after three cycles of NAC to evaluate the responses to treatment based on the Response Evaluation Criteria in Solid Tumors.20 After IDS, patients received various cycles of postoperative adjuvant chemotherapy (POAC).
Overall survival (OS) was defined as the time from the date of first chemotherapy to the date of death. Progression-free survival (PFS) was defined as the time from the date of first chemotherapy to the date of first recurrence. A gynecologic pathologist (H.S.K.) at our institution independently reviewed all microscopic slides according to the World Health Organization classification for accuracy of histologic subtyping.
Statistical analysis
Patients were classified by histological subtype into HGSC and non-HGSC groups. Differences in categorized variables between patients with HGSC and non-HGSC were tested by Pearson's chi-square test and Fisher's exact test. For continuous variables, Student's t-test or Mann-Whitney's U tests were used to compare groups. Kaplan-Meier survival curves were calculated and compared using the log-rank test. Univariate and multivariate analyses were assessed using a Cox proportional hazard model to evaluate prognostic factors affecting PFS and OS. p values less than 0.05 were considered indicative of statistical significance. All analyses were conducted using IBM SPSS, version 23 for Windows (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
Table 1 summarizes the baseline characteristics of the study population. Median age and BMI at diagnosis, as well as ASA score, did not differ between the HGSC and non-HGSC groups. In contrast, the median baseline CA-125 level before chemotherapy was lower in the non-HGSC group than in the HGSC group (351.3 U/mL vs. 2005.5 U/mL, p<0.001). The number of patients with FIGO stage IV was significantly higher in the HGSC group than in the non-HGSC group (74.1% vs. 48.0%, p=0.008). There was no significant difference in the number of NAC/POAC cycles between the two groups. Despite not achieving statistical significance, there was a tendency toward a higher number patients with more than six cycles of total chemotherapy in the HGSC group, compared to the non-HGSC group (153 vs. 21, p=0.077).
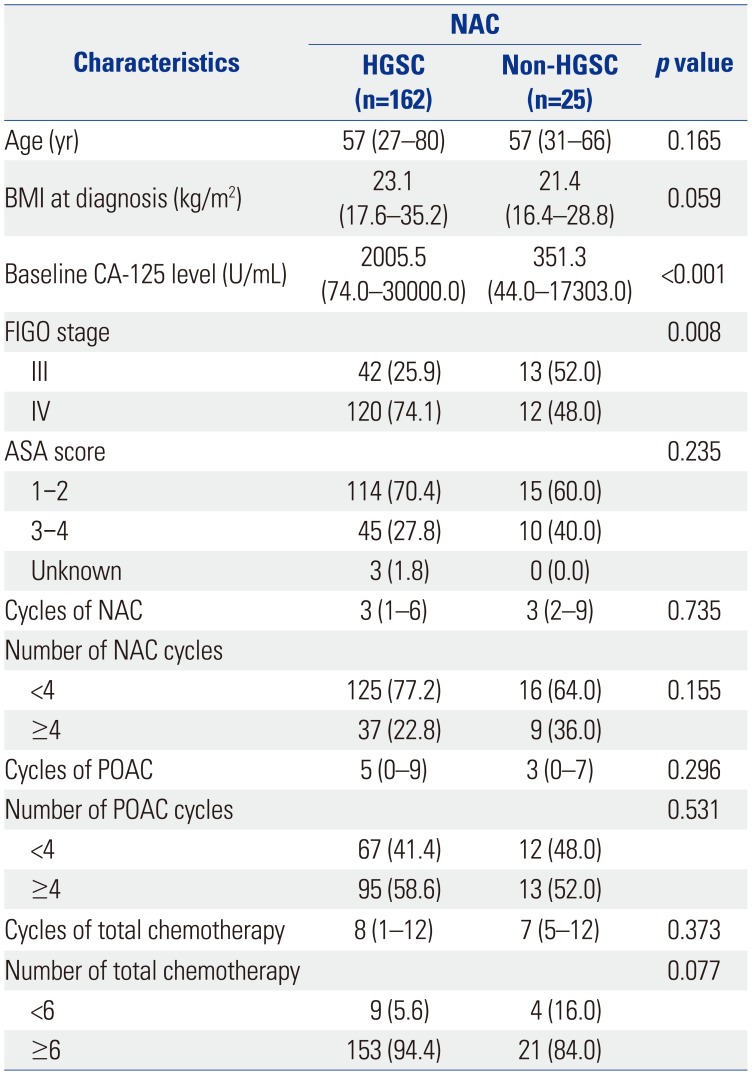
Table 1
Baseline Characteristics of the Patients with HGSC and Non-HGSC
HGSC, high-grade serous carcinoma; BMI, body mass index; CA-125, cancer antigen 125; FIGO, International Federation of Gynecology and Obstetrics; ASA, American Society of Anesthesiologists; NAC, neoadjuvant chemotherapy; POAC, postoperative adjuvant chemotherapy.
Data are presented as median (range) or number (%).
![]()
The median follow-up duration was 24.1 months (range: 0.1–106.3 months), during which there were 142 cases of recurrence and 71 deaths. Table 2 shows the treatment outcomes after NAC/IDS between the two histologic subtypes. The number of patients with more than a 90% reduction in CA-125 levels (comparing baseline and after the third NAC treatment) was greater in the HGSC group than in the non-HGSC group (74.1% vs. 28.0%, p<0.001). A significantly higher response rate after the third NAC treatment was found in the HGSC group than in the non-HGSC group (87.7% vs. 56.0%, p<0.001). The numbers of patients who achieved optimal debulking surgery (residual disease ≤1 cm) comprised 137 (84.6%) patients in the HGSC group and 16 (64.0%) patients in the non-HGSC group (p=0.003). There were no significant differences in the extent of surgery, lymphadenectomy, lymph node metastasis, and peritoneal cytology.
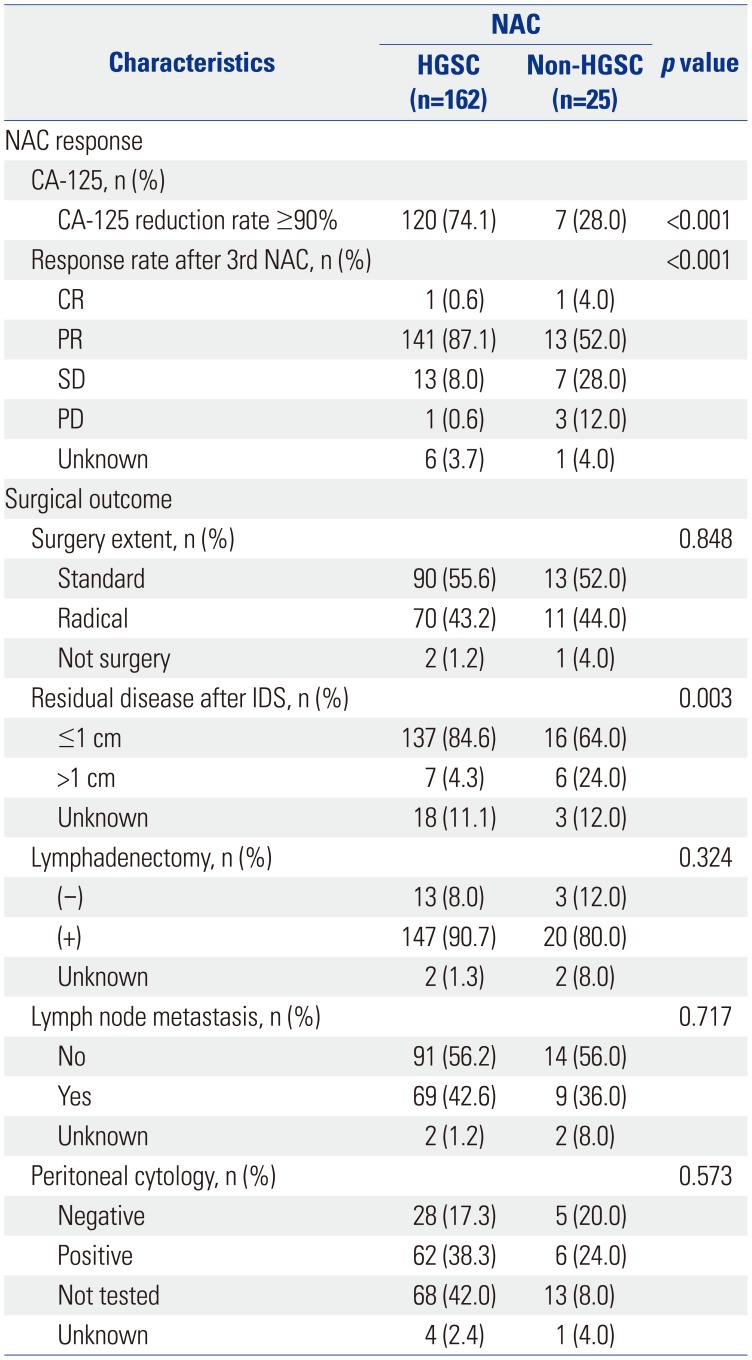
Table 2
Treatment Outcomes after NAC/IDS for HGSC and Non-HGSC
![]()
Of 25 patients with non-HGSC, histologic subtypes included clear cell carcinoma (n=9, 36.0%), mucinous adenocarcinoma (n=4, 16.0%), endometrioid adenocarcinoma (n=4, 16.0%), LGSC (n=3, 12.0%), carcinosarcoma (n=3, 12.0%), squamous cell carcinoma (n=1, 4.0%), and undifferentiated carcinoma (n=1, 4.0%).
Various methods were used to diagnose ovarian cancer before NAC: 13 by diagnostic laparoscopy (52.0%), nine by cytology of ascites (36.0%), two by pleural effusion cytology (8.0%), and one by aspiration biopsy (4.0%). After these diagnostic methods were performed, histologic subtypes could be determined in only eight cases (32.0%) before NAC. The reasons (multi-selectable) for NAC in patients with non-HGSC were high tumor burden (n=25, 100%), old age/poor Eastern Cooperative Oncology Group (n=2, 8.0%), diagnosis of HGSC before NAC (n=2, 8.0%), and being referred from another hospital after NAC (n=1, 4.0%) (Table 3).
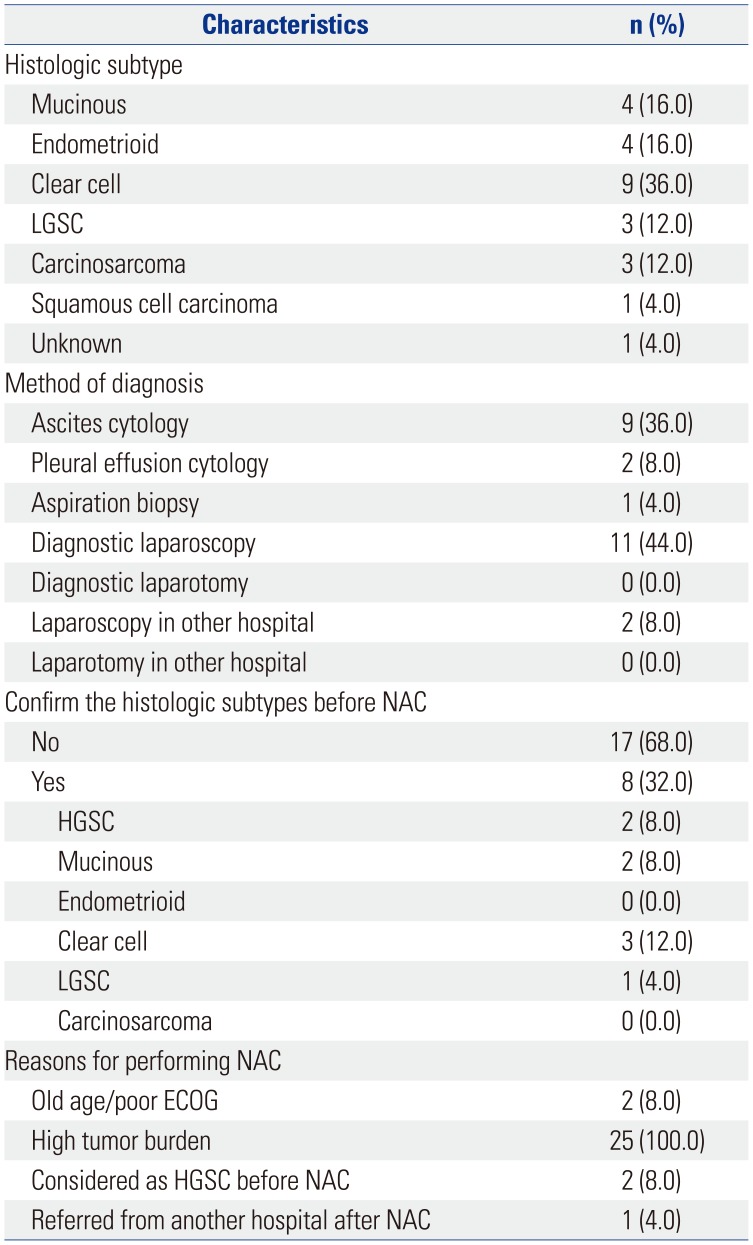
Table 3
Characteristics of Patients with Non-HGSC
![]()
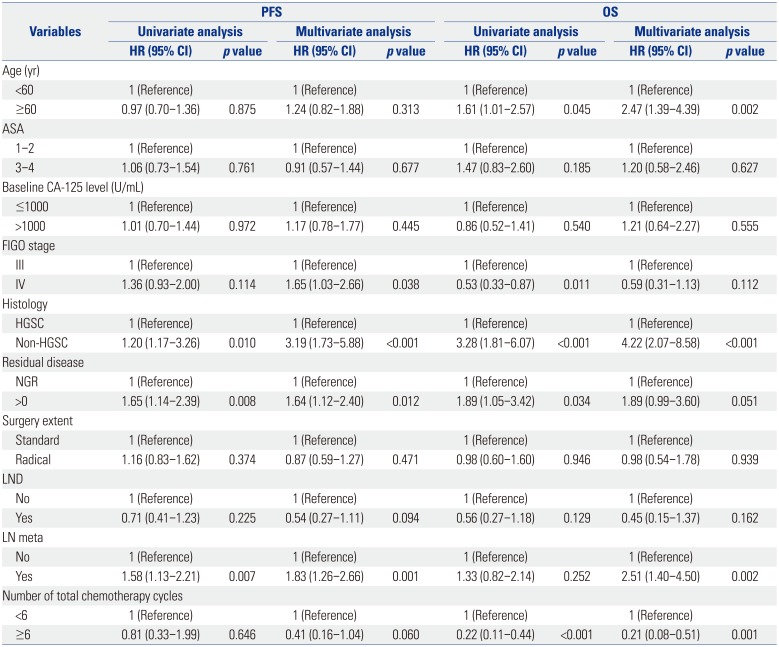
The Kaplan-Meier curves and the log rank test results showed that patients with non-HGSC had significantly poorer PFS (median PFS 10.3 months vs. 18.3 months; p=0.009) and OS (median OS 25.5 months vs. 60.6 months; p<0.001) than those with HGSC (Fig. 2). Table 4 demonstrates the cumulative hazards of adverse outcomes in patients receiving NAC. Multivariate analyses indicated non-HGSC as a negative predictor for both PFS [hazard ratio (HR), 3.19; 95% confidence interval (CI), 1.73–5.88] and OS (HR, 4.22; 95% CI, 2.07–8.58) in patients who underwent NAC.
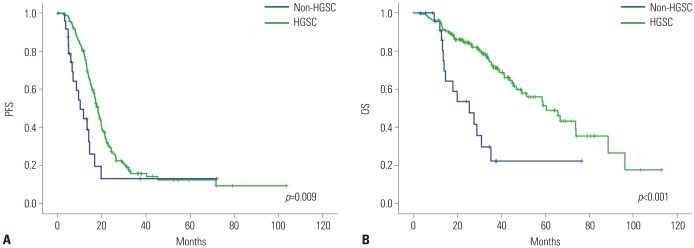 | Fig. 2Kaplan-Meier survival curves of (A) PFS and (B) OS according to histological subtype. HGSC, high-grade serous carcinoma; PFS, progression-free survival; OS, overall survival.
|
Table 4
Univariate and Multivariate Analyses for Progression-Free and Overall Survival Using the Cox Proportional Hazards Model
PFS, progression-free survival; OS, overall survival; HR, hazard ratio; CI, confidence interval; ASA, American Society of Anesthesiologists; CA-125, cancer antigen 125; FIGO, International Federation of Gynecology and Obstetrics; HGSC, high-grade serous carcinoma; NGR, no gross residual disease; LND, lymph node dissection; LN, lymph node.
![]()
Go to :
DISCUSSION
In this study, we found that patients with non-HGSC experienced a poorer response rate, lower rate of optimal debulking surgery, and poorer PFS and OS than those with HGSC. Furthermore, our results showed that the non-HGSC subtype is an independent prognostic factor for PFS and OS in patients with advanced ovarian cancer who undergo NAC.
Epithelial ovarian cancer includes a diverse group of heterogeneous neoplasms, with the five main subtypes being HGSC, endometrioid, clear cell, mucinous, and LGSC. In recent years, understanding of the underlying pathogenesis and the onset of molecular events in the different histologic subtypes has greatly increased, and although ovarian cancer is often clinically considered a single disease, there is now recognition that the various subtypes have different features and prognoses.21 Confirming the histological subtype of ovarian carcinoma before NAC is difficult. In most cases, the histologic subtypes cannot be confirmed by cytologic evaluation of ascites and pleural effusions; however, they can be determined from tissue obtained by performing diagnostic laparoscopy. In the EORTC 55971 trial and CHORUS trial, if a biopsy was not possible, patients with a CA-125 to carcinoembryonic antigen ratio greater than 25 were enrolled in order to exclude primary gastrointestinal tumors, and histologic subtype confirmation of diagnosis was not needed before randomization.1617 In our study, diagnostic laparoscopy was performed as a diagnostic method in 13 cases; however, NAC was administered according to criteria, such as high tumor burden, regardless of histologic subtype.
Several studies have evaluated the prognosis of patients with non-HGSC who have undergone PDS. Hosono, et al.6 reported that suboptimal residual tumor size was associated with poorer prognosis in non-serous subtype tumors, but not in serous subtype tumors. Melamed, et al.7 reported that there is no prognostic significance of residual disease status by histologic subtype. Mackay, et al.8 showed that mucinous and clear cell carcinomas are poor prognostic factors in stage III/IV ovarian cancer. Simons, et al.10 also suggested that patients with mucinous ovarian carcinoma have a significantly worse prognosis than patients with advanced-stage serous ovarian carcinoma.
NAC followed by IDS has been widely used for advanced-stage ovarian cancer, particularly for patients with an unresectable high tumor burden, old age, and a poor performance status. However, characteristics of the response patterns and survival outcomes of patients with non-HGSC who received NAC have not yet been published. In the NAC setting, the effect of debulking surgery is excluded, and chemo-sensitivity during NAC is a well-known prognostic factor for survival. Therefore, we could predict that patients with non-HGSC may have a poor prognosis due to resistance and may be less sensitive to taxane-platinum chemotherapy.
Recent advances in pathology and genetics have provided insights into the pathophysiologic features and natural history of ovarian cancer. For example, several studies have demonstrated that LGSC, mucinous, endometrioid, and clear cell carcinomas are characterized by mutations involving KRAS/BRAF, KRAS, CTNNB1, and PIK3CA genes, respectively.222324 Therefore, a tailored approach should be considered for this heterogeneous disease.
Many studies have evaluated histologic subtype-specific treatment of ovarian cancer. In the JGOG 3017 study, the alternative chemotherapy agent irinotecan combined with cisplatin was compared to conventional paclitaxel plus carboplatin for clear cell carcinoma in a randomized, phase III trial, with no significant survival benefit observed in the irinotecan plus cisplatin arm.12 Furthermore, there are currently two ongoing histology subtype-specific studies: one evaluating mitogen-activated protein kinase inhibitors in LGSC subtype tumors and one evaluating carboplatin and paclitaxel versus oxaliplatin and capecitabine with or without bevacizumab in mucinous subtype tumors. The Gynecologic Oncology Group recently completed accrual of a front-line, phase II trial of temsirolimus (mammalian target of rapamycin inhibitor) plus paclitaxel/carboplatin as first-line therapy for treating patients with newly diagnosed stage III/IV clear cell carcinoma. However, clinical data specific to subtypes are limited; thus, there is an unmet need for novel treatments according to histologic subtypes of ovarian carcinoma.222324
Several potential limitations of this study should be considered. First, the selection bias resulting from its retrospective nature may affect the results. Second, due to the increased use of NAC in recent years, this study is limited by the short follow-up period. Further studies with long-term follow-up are required for accurate evaluation of survival outcomes. Third, the non-HGSC group included several histologic subtypes because of the small patient sample. However, each subtype is considered to have distinctive morphologic and molecular genetic features that could affect study outcomes. Therefore, future studies with larger numbers of patients are needed to evaluate the subtype-specific outcomes among patients with NAC.
Despite these limitations, our study has the following strengths. Since we applied the same criteria and the same chemotherapy regimen for NAC regardless of histologic subtypes during the study period, the comparison of non-HGSC and HGSC might be justified.
In conclusion, histologic subtype is an independent prognostic factor for patients undergoing NAC for advanced-stage ovarian carcinoma, and patients with non-HGSC showed poorer survival than those with HGSC. Therefore, different selection criteria and different treatment strategies for NAC should be applied to patients with non-HGSC.
Go to :
 XML Download
XML Download