

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Today, health systems plan their most important programs based on family health. Women are the center of family health and are the main role model for the next generation of teaching and promoting healthy living.1 Menopause is part of the critical phases of a woman's life, which characterizes the transition from fertility to infertility.2
Menopause is derived from 2 Greek words, “meno” meaning month and “pause” meaning stop. Thus, menopause is permanent cessation of menstrual periods, along with total absence of ovarian follicular function (World Health Organization, 2006). It is characterized by cessation of menstruation, implies loss of childbearing capacity, and aging.3 Postmenopause refers to the period of life after menopause has occurred. According to Webster New World Medical Dictionary, “it is the time after which a woman has experienced 12 consecutive month of amenorrhoea.4 According to Indian Menopause Society research, there are about 65 million Indian women in the age group of 45 years. Average age of menopause is around 48 years but it strikes Indian women at the age of 30 to 35 years. So menopausal health demands even higher priority in Indian scenario.3
Menopause is accompanied by biological and psychological changes that affect women's health and sense of wellbeing. Menopause happens because the woman's ovaries stop producing the hormones estrogen and progesterone. They include changes in periods (shorter or longer, lighter or heavier with more or less time in between), hot flushes and/or night sweats, trouble sleeping, vaginal dryness, mood swings, trouble focusing and less hair on the head, more on the face, experience an age-related decline of physical and mental capacity.4 The physiological, emotional and psychological changes leave women vulnerable in total and reduce the quality of life (QOL). A study was conducted among the postmenopausal women members and nonmembers of elderly support association reveals that mean total score of QOL of member of the association was significantly greater than non-members. There was a significant relationship between QOL and membership of the association (P < 0.05).1
Indian women are ignorant about the changes taking place in their reproductive system. Religion and culture of our society also inhibits to express these changes. So awareness programs need to be conducted to overcome these issues. But there is lack of awareness of the causes, effects, and management pertaining to it.5 Hence there is a growing need to have counseling and training program by the professionals to improve women's health, reducing problems and enhancing QOL in menopause period. It was evident from a study findings which aimed to investigate the effect of counseling on QOL shows that before the counseling session, mean ± standard deviation for QOL in experimental group was 101.2 ± 31.4 and it was significantly decreased to 96.9 ± 27.0 after intervention (P < 0.05). While no significant change was observed in the control group (from 98.9 ± 35.5 to 102.3 ± 35.0, P = 0.443).6
Health personnel can educate women to have modification in the lifestyle practices such as having well balanced diet, regular exercises, decreased fat and salt intake, avoidance of self-medication, fruits and vegetable consumption, blood pressure control, and increased daily water consumption, practicing relaxation through pranayama and meditation. This helps them to identify and adapt to the various changes taking place in the body, so that the women will be better equipped to face the changes and minimize the risk of this potentially disruptive period.78 A wide gap in the knowledge has been documented on the women from developed and developing countries. And this gap is even wider in women among rural and urban communities. In this regard, this study aimed to compare the QOL of postmenopausal woman in rural and urban areas and to improve it through a health promotion awareness program.
Materials and Methods
The study adapted quantitative approach with cross sectional survey design. The study population consisted of postmenopausal women who attained menopause and experienced menopausal problems. Women with surgical menopause, receiving any kind of hormone therapy, presence of medical conditions like diabetes, hypertension and cardiac diseases were excluded. A total of 100 postmenopausal women were selected using purposive sampling technique residing in rural and urban areas of Mangalore. The data was collected using demographic proforma and menopause specific QOL (MENQOL). The MENQOL questionnaire is a self-administered 29-item survey questionnaire, designed to describe QOL in menopausal women and which measures the extent to which an individual is affected by menopausal symptoms. All items in the MENQOL questionnaire followed the same format. It comprised of menopausal symptoms in 4 domains: vasomotor, psychosocial, physical, and sexual. Each women was asked whether she experienced the symptoms in the previous 6 months if answer was no she was asked next item and if answer was yes she was asked to indicate how bothered she had been by the symptoms on a seven point scale ranging from 0 = not at all bothered to 6 extremely bothered. The demographic proforma, MENQOL and awareness program on postmenopausal health was submitted to 12 experts for face validity. Permission was obtained from District Health officer before conducting the study. Pilot study was conducted to check the practicability and feasibility of the study design. The investigator conducted the study in rural and urban areas of Mangalore. The purpose and nature of study was explained to the subjects and informed consent was taken from the participants. The data about the participants was collected using demographic proforma and MENQOL. An awareness program was given to the participants for 30 minutes which highlighted on postmenopausal health which include health promotional activities such as diet, exercise, yoga, meditation and periodic health checkups to relieve menopausal symptoms.
Results
1. Sample characteristics
Among 100 samples 52% of the subjects were in the age group of 51 to 55 years, 48% had secondary education, the occupational status reveals that majority (32%) of them were coolie workers and 92% of the subject were married women. Fifty percentages of participants were from Christian religion. Majority (64%) of subjects' belonged to nuclear family, 50% subjects had monthly income between Rs.6001–9000.
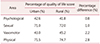
2. Assessment of different domains QOL of postmenopausal women in rural and urban area
As shown in the Table 1, the QOL score of physical domain was 71.5% in urban and 74.7% in rural with difference 2.8, in sexual domain was 71.0% in urban 72.0% among rural women with difference 1.0%, in vasomotor domain was 45.2% in rural and in urban 43.0% with difference 2.2, in psychological domain was 41.8% in rural and in urban 42.6% with difference 0.8.
3. Comparing the QOL of postmenopausal women in urban and rural areas
The Table 2 shows that the mean QOL score (X2 = 27.24) of rural area was higher than the mean QOL score (X1 = 26.34) of urban area. The calculated ‘t’ value (t = 0.86) is lesser than the table value (‘t98’=1.980). The computed ‘t’ value shows that there is no significant difference in the QOL. This indicates that there is no significant difference between the mean QOL score of postmenopausal women in rural and urban areas.
4. Association between the QOL of postmenopausal women and selected demographic variables
The calculated chi square value and demographic variables such as age of the women (χ2 cal = 0.000; P > 0.05), occupation (χ2 cal = 0.080; P > 0.05), type of family (χ2 cal = 0.325; P > 0.05) and age at menopause (χ2 cal = 0.368; P > 0.05) showed that the association between the QOL and demographic variables are not statistically significant at 0.05 level. The finding shows that the association between QOL of urban postmenopausal women and monthly income of the family (χ2 cal = 4.023, P < 0.05) was statistically significant at 0.05 level.
Discussion
The present study record the socioeconomic profile of postmenopausal women which highlights 52% of women were in the age group of 51 to 55 years which is congruent with the study conducted in Srilanka where the study subjects were (59.4%) predominantly in the age group of 51 to 60 years.9 Similar cross-sectional descriptive study was done at Iran also shows that the participants were over 55 years.1 A study conducted in Karnataka shows that 56% of women from rural area. The present study reveals that the physical symptoms were more among rural women (7.71%) compared to urban women. This includes symptoms such as feeling tired, aches and pains, joint pain and bloating. This could be the lifestyles and status of women at home. The women continue to work for the family in spite of their poor health.10 Similarly psychological symptoms such as loss of memory, anxiety, feeling lonely, sadness was reported more (42.6%) among urban women. Vasomotor and sexual domain the difference in QOL score is very minimal among the rural and urban women.11 Similar findings were reported in a study which shows that the rural women had less prevalence of anxiety attack (7.3% vs. 4.2%) than urban women.12 The study findings were differ in a study conducted by Hakimi et al.13 shows that the mean scores of menopausal symptoms and their subscales showed significantly higher scores in the physical and psychological subscales in the urban women, while the rural women had significantly higher scores in the concern subscale. Another clinical trial findings conducted in Iran shows that there was significant difference in the mean of QOL scores between the 2 groups in immediately after the educational intervention and 3 months after the educational intervention in dimension of vasomotor, psychosocial, sexual and physical (P < 0.001).14
The family support during this transition period is very significant as the women have changes occurring in physical, psychological and social domains of life. Women experience feelings of guilt and embarrassment in the menopause. It is suggested that these feelings are guiding the behavior and affecting the image of one in the eyes of others. Both feelings are enhanced by interpersonal and family relationships.15 This was supported by a study conducted in Iran showed that the knowledge and performance of spouses in the menopausal health training program group were significantly higher 3 months after intervention (P < 0.0001). The QOL in women in the menopausal health training program group was higher 3 months after intervention (P < 0.0001). The mean scores of psychological and physical domains were significantly lower in the intervention group (P = 0.002 and P = 0.001, respectively).16 This is highlighted in a study conducted to find the relationship between the women's attitude and QOL revealed that the women whose relationships with their husband were negatively affected had higher vasomotor, psychosocial, physical, and sexual symptom scores (4.2 ± 1.7, 3.7 ± 1.7, 3.5 ± 1.5, 3.5 ± 1.8). Similarly, the vasomotor, psychosocial, physical, and sexual symptom scores were high in women who declared an unfavorable relationship with their children (4.5 ± 1.8, 3.8 ± 1.6, 3.7 ± 1.4, 3.2 ± 1.9).8
A number of alternative medical discipline including homeopathy, naturopathy, acupuncture and traditional medicine, yoga and meditation have developed remedies for postmenopausal problems and to enhance the QOL. This was strongly supported in a study to determine the efficacy of 3 non hormonal therapies for the improvement of menopause-related QOL in women with vasomotor symptoms.17
While comparing the overall QOL among the urban and rural postmenopausal women the present study findings shows that the difference is not significant statistically. The study findings were supported by a study conducted in Japan reveals that 24.4% of the perimenopausal and 26.6% of the postmenopausal women suffered from moderate or severe menopausal symptoms. The decreasing level of QOL was correlated with the severity of the menopausal symptoms in the peri- and postmenopausal women among community dwellers.18 It infers that the postmenopausal symptoms experienced by women are same, irrespective of their place of residence. The investigator felt that the reason could be the influence of mass media such as TV, radio, newspapers, and social media which have deep rooted impact on the life styles of the people everywhere. In olden days the women had a close knitted interaction with the family members with whom they were sharing their reproductive problems and issues.3 The present study also reveals that most (64%) of the women were from nuclear family. Since the social structure has changed the trend of joint family to nuclear family the women depend on the mass media to know about their health problems.
Conclusion
The changes are inherent everywhere, there is no exception for human life. The changes may be developmental or transitional. Midlife is one such transitional periods, which brings about menopause in women and demands significant changes in the QOL. The health care industry has a vital role in assessing, informing and maintaining an improved QOL. The family, society and the community as a whole have to take a constructive role in supporting a woman as she pass through this crucial period.

 XML Download
XML Download