

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A combined hepatocellular carcinoma-cholangiocarcnoma is a relatively rare disease entity, accounting for only 0.4–14% of all primary liver cancer.1234 The classification of hepatocellular carcinoma-cholangiocarcnoma first developed by Allen Lisa in 1949 consisted of 3 subtypes: 1) type A, characterized by synchronous, separate and autonomous epicenters of hepatocellular carcinoma (HCC) and cholangiocarcnoma (CC) in a single liver; 2) type B, comprising closely admixed and distinguished foci of HCC and CC; and 3) type C, consisting of truly combined HCC and CC components originating in the same tumor.15
Surgical resection may still lead to intra- and extra-hepatic recurrence, which is a major concern. Although relatively common in hepatocellular carcinoma (HCC), metastasis to adrenal gland rarely occurs in intrahepatic cholangiocarcinoma (ICC) and combined HCC-CC (cHCC-CC). We experienced a unique case of sequentially developed cHCC-CC, classified as Allen Lisa A, with adrenal metastasis as the primary presentation and a hidden primary HCC.
CASE
Sixty-five years old female with a history of jaundice and abdominal discomfort with a high serum alpha-fetoprotein (AFP) and low serum chorioembryonic antigen (CEA) (532 ng/ml and 1.9 mg/dl, respectively). No evidence of prior hepatitis infection was found and preoperative computed tomography (CT) scans showed multiple enhancing lesions intraductally within the left intrahepatic duct as shown in Fig. 1. She was preoperatively diagnosed with segment 4 mixed type cHCC-CC (Allen Lisa C), and underwent an S4 segmentectomy and hepaticojejunostomy. No additional masses were found during surgery. As illustrated in Fig. 2, the pathological result confirmed a 5-cm papillary adenocarcinoma, with intraductal growth, without any evidence of malignant hepatocytes.
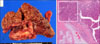
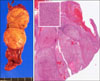
A follow-up CT scan for disease surveillance revealed a right adrenal mass that gradually enlarged, with a marked increase in serum AFP (4,950 ng/mL). Magnetic resonance imaging (MRI) and positron emission tomography (PET)-CT also suggested a metastatic lesion in the right adrenal gland (Fig. 3). A percutaneous adrenal gland biopsy confirmed a metastatic HCC (positive for AFP, glypican-3, and hepatocytes, and negative for CD-10, inhibin-α, EMA, S-100, and cytokeratin-7), and right adrenalectomy was performed uneventfully. The specimen is shown in Fig. 4. As shown in Fig. 5, the serum AFP immediately declined to 4.1 ng/mL, shortly after adrenalectomy. Unfortunately, a recurrent S7 liver mass was suspected 1 year after adrenalectomy, with serum AFP 7.6 ng/mL and CT imaging characteristic of HCC. A series of Trans-arterial chemo-embolization (TACE) and RadioFrequency Ablation (RFA) procedures were then performed with favorable responses (Fig. 6).
DISCUSSION
cHCC-CC was first reported by Wells in 1903, and further classified by Allen and Lisa in 1949 and Goodman in 1985.56 It originates in hepatic progenitor cells, the liver-specific bipotential adult stem cells, which are activated upon injury to hepatocytes and/or cholangiocytes.7 Thus, it has the ability to differentiate into hepatocellular carcinoma, cholangiocarcinoma, or both. A few ductal plate malformations, particularly von-Meyenburg complex, show malignant transformation to intrahepatic CC (ICC) suggesting the possibility of combined HCC and ICC originating in ductal plate malformation.8
Histophatologic diagnosis of cHCC-CC, according to World Health Organization (WHO), is characterized by an unequivocally differentiated hepatocellular and biliary component in one tumor, which correspondends to Allen Lisa C (Mixed Type) or Goodman I (Collision tumor).1 Accurate preoperative diagnosis is difficult and often leads to misdiagnosis. cHCC-CC should be highly suspected in cases where imaging reveals both HCC and CC features, regardless of tumor marker levels; in the presence of elevated tumor markers (AFP and CA19-9, regardless of imaging features) or conflicting imaging and tumor marker findings.
Initial preoperative diagnosis in our case report was cHCC-CC, based on the contradictory findings: tumor marker level (a very high AFP) and imaging features of cholangiocarcinoma (intraductal gradually enhancing lesion within the left intrahepatic duct). However, since no additional metastatic lesions were present, liver resection and lymph node dissection was a rational choice,13 despite the fact that the recurrence rate after surgery was still higher than in hepatocellular carcinoma (disease-free survival of HCC vs. cHCC vs. ICC : 68.2 months vs 23.4 months vs 15.5 months).9
Several prognostic factors of cHCC-CC associated with unfavorable outcome include large tumor size, vascular invasion, lymph node metastasis, and the presence of satellite lesions.69 Ariizumi et al.10 reported a median survival of 15.4 months, with a 5-year overall survival rate found in 24% of all patients. Another report by Lee at al.9 showed an overall survival rate of 47.3 months, shorter than HCC (71.7 months), but longer than ICC (21.5 months).
With regards to the nature of disease recurrence and poor survival, close surveillance after surgery is an important aspect of management strategy, as in HCC or ICC. Early intra- and extra-hepatic recurrence was detected, warranting regular imaging surveillance as well as tumor marker follow-up studies. The incidence of extra-hepatic metastasis is around 13.5 to 42 %,1112 including metastasis to adrenal glands (12%).11 Presentation of a cholangiocellular component appeared to be a poor prognostic indicator.13
Since both adrenal glands are almost always included in the scanning area, any changes in size and glandular characteristics may be visualized to detect adrenal incidentalinoma, 3 an adrenal tumor discovered fortuitously during imaging for other indications.14 Possibility of malignancy increases with large tumor size, heterogeneous lesion and presence of peritoneal lymphadenopathy. Because of the rich sinusioidal blood flow and its multiple arterial supplies, the adrenal gland is a potential site for metastasis.15 The mechanism of extrahepatic metastasis from primary liver tumor to adrenal glands may involve a direct extension through exophytic growth or systemically through retroperitoneal venous system.12 Poor differentiation of malignant lesions from benign adenoma remains a diagnostic challenge in the management of adrenal incidentalinoma.16
The diagnosis of adrenal metastasis in our case was straightforward—based on the size of the lesion, history of previous malignancy, and low attenuation in pre-contrast study. However, percutaneous biopsy was indicated for accurate histopathological diagnosis, due to conflicting results based on initial preoperative diagnosis of cHCC-CC and postoperative histopathology of ICC.
The 5-year survival rate of HCC patients with resected adrenal metastasis was reported around 20% to 45%.15 When compare to other modality or no treatment, adrenalectomy provides the highest survival (11.1 months, 5.7 months, 21.4 months, respectively).17 Disease-free interval of less than 12 months is associated with poor survival.15
Interestingly, we detected a sequentially developed cHCC-CC (Allen Lisa A), with adrenal metastasis as the first presentation of a hidden hepatocellular carcinoma. Although S4 mass was cholangiocarcinoma, metastasis or recurrent mass showed HCC-like features. Tsalis et al.18 first reported the case of adrenal metastasis as the first presentation of HCC in a 76-year-old male with a marked increase in tumor markers but without initial liver masses. Pandey et al.19 reported a case of adrenal metastasis from ICC, and the patient is still alive with recurrent disease 2 years after surgery.
The sequentially developed cHCC-CC in this case was unique and invaluable although the S4 mass was cholangiocarcinoma, whereas metastatic recurrent mass showed HCC-like figures. Our report suggests that a markedly increased level of tumor markers, after resection of a liver malignant lesion, without a visible postoperative liver mass, requires comprehensive evaluation for the possibility of disease recurrence. In conclusion, adrenal metastasis may present as the primary focus of HCC in sequentially developed cHCC-CC patient with hidden primary HCC.




 XML Download
XML Download