

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The goal of total hip arthroplasty (THA) is to restore natural biomechanics of the hip joint. To achieve this goal, a number of innovative implants have been designed by pioneers of THA. The idea of stem modularity enables fine tuning of the joint by affording substantial surgical flexibility. Due to its versatility, various modular stem designs have been introduced123).
Despite concerns with possible corrosion and/or failure at the modular interface456), complex surgical procedures7) and high costs, modular stems are being widely used in both primary and revision surgeries. Although tapered stem designs are now gaining popularity in primary cases, femoral implants with modular proximal sleeve are still associated with a number of potential challenges891011121314). In this report, the types and advantages of contemporary modular stems are introduced; our experience with their use in complex primary THAs are also reported.
TYPES OF MODULAR STEMS
Various modular stem shapes have been developed, and currently available modular stems can be broadly classified as: i) proximal, ii) mid-stem or iii) distal based on the location of modular junctions13).
Proximal modular stems have the largest variations in their design styles (e.g., modular heads, shoulders, necks, collars and sleeves). Compared to the original Chanley's monoblock stem which had a body, neck, and head as one unit, almost all modern femoral stems provide proximal modularity by using a modular head. Modular proximal shoulders had been developed based on European experience in the 1970s. There are numerous types of proximal bodies and fixation mechanisms to adjust the medial offset, vertical height, and version to compensate for deformities of proximal femurs1).
Modular neck designs also allow operators to choose the appropriate degree and length of the neck for desired stability and range of motion3) (Fig. 1). However, most implants with modular necks were withdrawn from the market because of junctional problems1516171819). Recently, there has been high incidence of failure due to fretting corrosion at the junction of cobalt-chromium modular neck and titanium body. Corrosion at the modular interface generates metallic debris and ions responsible for hypersensitivity, toxic synovitis, osteolysis, and pseudotumor20212223).
Mid-stem modularity is efficient in a complex revision surgery in which the femur has poor proximal bone stock24252627) (Fig. 2). Under such conditions, the stem should be fixated at the distal diaphysis to gain substantial stability and the mismatch between proximal and distal femoral anatomy can be overcome with mid-stem modularity.
Distal modularity was initially developed to increase distal fixation and reduce thigh pain by inserting a device at the stem tip. However, it has failed to show clinical relevance1).
MODULAR FEMORAL PROSTHESES WITH PROXIMAL SLEEVES
To date, the greatest achievements in the history of modular stems are those with a proximal sleeve. In 1956, Konstantin Sivash, a Russian orthopedic surgeon first developed a hip implant which had an uncemented stem and cup with metal-on-metal articulation2829). In 1967, he modified his original stem by applying a proximal modular sleeve to ensure maximal contact between the bone and the implant3031) (Fig. 3). Four years later, an American company acquired the license for the Sivash stem. After adding coronal slots and 8 flutes to the distal stem, and applying porous coating at the proximal sleeve, the stem was renamed “SRN”. In 1982, the stem was again modified and renamed “S-ROM”. It has been continuously used without major changes since 1985.
ADVANTAGES OF MODULAR SLEEVE PROSTHESES
Tight fixation between the proximal metaphysis and the modular sleeve ensures that the S-ROM stem provides significant proximal stability independent of proximal femoral geometry8932333435). At the same time, the implant can have considerable distal rotational stability when designed with a fluted long stem. The surface of the proximal sleeve has a shape of steps with porous coating, which enables great initial fixability and durable stability by a bone ingrowth.
The major advantage of the S-ROM hip system is that it can be modulated intraoperatively according to femoral anatomies. A surgeon can choose the appropriate sleeve by selecting from various height and width options to match a specific metaphyseal morphology. In addition, there are multiple stem options with different neck styles which enables surgeons to modify medial and vertical offsets. Furthermore, stems with varying curvatures and lengths are available. There are a total of 10,398 possible combinations of sleeves, stems, and heads. These combination can be almost infinite considering independent rotation (or version) of the stem36). This means that a surgeon can modify the biomechanics of the femur without concern for implant stability.
OUTCOMES OF MODULAR SLEEVE IMPLANTS
The S-ROM modular prosthesis was originally introduced to respond to complex reconstructive surgery. In practice, it was widely used in almost all situations including simple primary THAs. It was first implanted by Hugh Cameron in July 1984. Later, he reported8) that there was no aseptic loosening among 202 consecutive THAs after 2 to 8 years of observation. In radiographs, he found osteolytic lesions around proximal stems while, only one osteolysis was visible beyond the proximal sleeve. Christie et al.37) also reported 175 stems with a mean follow-up of 5.3 years. Only one stem was revised for aseptic loosening and 89% showed radiographic bone-ingrowth.
Longer follow-up showed excellent clinical and radiologic outcomes. We have retrospectively reviewed 64 osteonecrotic hips with a minimum of 15 years of follow-up38). The mean Harris hip score improved from 36 points to 92.7 points and survivorship of the stem for aseptic loosening was 100% at final follow-up. Le et al.39) also reported no aseptic loosening with a mean follow-up of 17 years. Osteolysis around the proximal stem was observed in 58% of cases; however, none were located below the sleeve-stem junction.
The biggest concern associated with S-ROM stems includes metallosis, fretting corrosions and failures at the modular interface. While Cook et al.4) reported that slippage and micromotion could occur at the stem-sleeve interface based on their biomechanical data, Bobyn et al.5) proved that the volume of wear particle was not significant enough to cause adverse effects, even under extreme conditions. There were also concerns of failure at the modular junction; however, many clinical studies have revealed reliable longevity of the implant. There are only a few case reports of implant fractures limited to 9-mm stems40414243).
MODULAR STEMS IN COMPLEX PRIMARY THAS
1. Developmental Dysplasia of the Hip
Anatomical abnormality make THA difficult in patients with developmental dysplasia of the hip (DDH). Particularly in cases of Crowe type 3 or 4 deformity (or Hartofilakidis type C), femoral heads are highly dislocated with shallow true acetabulum114445) (Fig. 4). Due to contraction of surrounding soft tissues, it is very difficult to pull down the hip center to its original position. Such situations frequently require massive soft tissue release or preoperative traction. Even with careful attention, excessive lengthening or traction of the limb can lead to sciatic nerve injury46).
In this case, subtrochanteric shortening osteotomy combined with the use of an S-ROM prosthesis is effective454748495051525354) in both joint reduction and in the prevention of nerve palsy. Klisic and Jankovic55) introduced a method of making transverse osteotomy distal to the lesser trochanter in 1974. Combined with the use of an S-ROM stem, we can obtain firm fixation at the metaphyseal region and rotational stability at the distal osteotomy site without using additional fixation device like plates or cables. Moreover, increased anteversion can be treated with a free rotation between the sleeve and the stem.
Takao et al.50) reported results of THA with subtrochanteric osteotomy using S-ROM modular stems in 25 patients (33 hips) with Crowe type IV DDH. They found that the average leg length discrepancy was reduced from 5.1 cm preoperatively to 2.8 cm postoperatively. There were no cases of nonunion at the osteotomy site or sciatic nerve palsy. After a minimum follow up of 5 years, only one stem was revised for aseptic loosening. Biant et al.53) also performed THA using S-ROM modular stems in 28 Crowe type III or IV DDH. The Harris hip score improved from 37 points to 81 points at follow-up of more than 10 years. There were no cases requiring stem revision.
2. Sequelae of Septic Arthritis
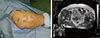
Patients with septic hip sequelae often have more distorted bony structures than those with DDH. Patients with neglected septic arthritis usually have hypoplastic femurs with rudimentary heads, small canal diameters, dysplastic acetabulum, and high-riding hip centers105657) (Fig. 5). Additionally, cases with previous arthrotomies, scars with old draining sinus, contracted peri-capsular structures, and weak abductors with severe atrophies (Fig. 6) are common. Therefore, a precise surgical technique with appropriate implant selection is extremely important.
S-ROM prostheses allow for proximal fixation by using a small sleeve where it is difficult to obtain initial fixation due to severe femoral deformity. In most cases, a narrow stem with small offset is used to reduce soft tissue tension, since preoperative offset is usually minor and the hip is highly dislocated. As with high-riding DDH, subtrochanteric osteotomy is often performed in the infection sequelae. To deal with accompanying severe rotational deformity, derotational osteotomy can be performed at the same time.
In our previous study10), among 58 patients with infection sequelae, 87.9% showed good to excellent clinical results with a mean follow-up of 8.3 years for THA using the S-ROM modular system. Only one patient underwent femoral revision due to recurrence of infection. No aseptic stem loosening was observed during the study period.
3. Skeletal Dysplasia
In cases of skeletal dysplasia, a large, flat femoral head with poor acetabular coverage, coxa vara, and shortened neck with decreased horizontal offset can make THA difficult (Fig. 7). Even under such conditions, favorable results can be obtained by using a small proximal sleeve and a modular stem with proper offset and diameter. In our group14), 23 patients with multiple epiphyseal dysplasia showed excellent clinical and radiographic results maintained for a mean of 4.8 years after THA with modular stems. No revisions of the femoral component were required during that period.
4. Previous Surgery
If joint-preserving surgeries (e.g., osteotomy and core decompression) are performed previously, severe deformities of the proximal femurs and soft tissue scarring are commonly observed (Fig. 8). In this situation, an intraoperative fracture may occur during the broaching procedure due to bony scars and blocks formed by previous operations. Therefore, modular implants applied with a reaming technique may be safer than tapered stems using a broaching system. In addition, precise intraoperative modifications and biomechanics approaching normal (i.e., pre-surgery levels) can be obtained by using modular prostheses.
We compared13) 36 patients who previously underwent joint preserving surgery for osteonecrosis of the femoral head with a matched control group of 39 osteonecrotic hips without previous surgeries. All THAs were performed using S-ROM prostheses and patient follow up was conducted for a mean of 4.6 years. Although the study group had more perioperative blood loss and longer operation times, there was no significant difference in mechanical failure rates between the two groups.
SUMMARY
Modular stems have a long history and have evolved into various forms. Implants with proximal sleeves have shown excellent mid- to long-term outcomes in a large number of cases. Although performing a surgical procedure with a modular prosthesis remains quite demanding and invasive, we recommend its use in complex primary THAs where the proximal femur is severely deformed.







 XML Download
XML Download