

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Arthroplasty can fail because of aseptic loosening, instability, periprosthetic fracture or infection of the prosthesis. In general, the incidence of periprosthetic joint infection (PJI) is lower than aseptic loosening1), but it is more serious and complex complication following arthroplasty. The haematogenous seeding could happen at any time during the rest of patient's life after surgery. For doctor, the treatment and diagnose PJI are still challenging in the modern world. The implant as a foreign body increases the pathogenicity of bacteria and the presence of biofilm makes the diagnosis and treatment complex and difficult. Therefore, appropriate management protocol of PJI should be established, in a timely manner to take preventive measure and diagnosis, and accordant strictly with the results of culture and antimicrobial susceptibility test, to avoid the increase in the rate of bacterial resistance and select reasonably antibiotics combined with adequate operation procedure. Eventually, it achieves eradicating of infection, preserving joint function without any pain.
EPIDEMIOLOGY
The joint arthroplasty is a safe and cost-effective surgical technique. It can alleviate symptoms, recover functions and enhance quality of life, especially in the elderly population23). With the increment of the joint prosthetic replacements, the number of postoperative complications has also increased. The infection rate after hip or shoulder replacement is usually less than 1%, after knee replacement less than 2% and after elbow replacement is between 1.9% and 10.3%. The reason for higher incidence in elbow region may be related to the more frequent rheumatic disorder, trauma or multiple reconstructive procedures compared to hip and knee surgery45).
PATHOGENESIS AND CLASSIFICATION
Development stages of the biofilm formation are divided into 4 phases; namely adhesion, proliferation, biofilm maturation and cellular detachment10). The bacterium adheres to the foreign body material that is the first step which can cause biofilm-related infections. The materials of orthopedic implant (such as titanium, ceramics, hydroxyapatite, and polyethylene) is easy for the bacteria to colonize on. Biofilms is a complex community of microorganisms embedded in an extracellular matrix that forms on surfaces of prosthesis.
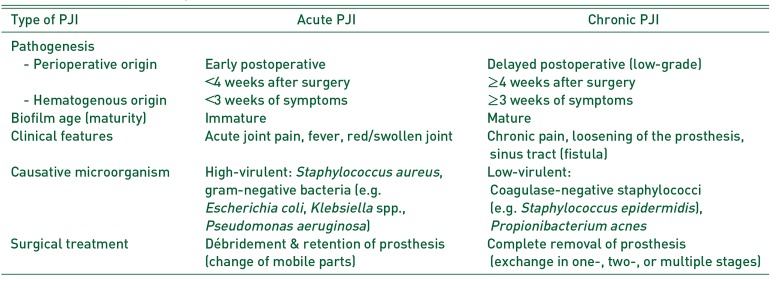
The prosthesis can get infected by three pathways: first, perioperative period, most commonly through intraoperative inoculation; second, haematogenous could happen at any time after implantation, pathogen from different parts, e.g. respiratory or urinary tract infection, skin infection and pneumonia; and third, direct contact with a nearby infected, e.g. infected soft tissue, septic arthritis or osteomyelitis11). Table 1 shows the classification of PJI into acute and chronic infection. The early (immature) biofilm can be eradicated without remove prosthesis. If symptoms persist less than 3 weeks (hematogenous) or infection manifests less than 4 weeks after surgery (perioperative). Other procedures is defined as chronic PJI, the implant must be changed due to mature biofilm.
DIAGNOSIS
Early diagnosis is a positive factor to save the prosthesis and the joint function. No single indicator of a test using in clinic or in laboratory can hand out ideal sensitivity and specificity aiming to the diagnosis of PJI12), so a mixture of multiple tests can reasonably increase the diagnostic accuracy. Some criteria from the Musculoskeletal Infection Society (MSIS), European Bone and Joint Infection Society (EBJIS) and Infectious Diseases Society of America (IDSA) have been recently published131415). The EBJIS criteria are more sensitive for the diagnosis of PJI than other criteria (Table 2)16).
1. Laboratory Studies
If PJI is suspected, serum C-reactive protein (CRP) is usually performed17). This marker is inexpensive, rapid and has a better performance than erythrocyte sedimentation rate (ESR). However, CRP is not specific for infection and usually increases due to healing process after intervention. Pérez-Prieto et al.18) found that with normal CRP about one-third of chronic, low-grade infections would be missed. So the combination of CRP and ESR is used for diagnose PJI1920), the sensitivity of combined ESR (>30 mm/hr) and CRP (>10 mg/L) was 96%, but low specificity 56%21).
Synovial fluid aspiration and culture are the most accurate preoperative examination for the diagnosis of PJI17). Synovial fluid leukocyte count and granulocyte percentage can accurately distinguish PJI from aseptic failure22), and has a sensitivity of 86% compared with synovial fluid culture (52%)23). The patient with rheumatoid arthritis, periprosthetic fracture or dislocation and in the early postoperative period should be excluded, because the cell count shows falsely high1116212224).
2. Histopathological Studies
Histopathological examination has a high sensitivity (95%) and specificity (92%) for the diagnosis of PJI. Based on histomorphological criteria, four types of periprosthetic membranes have been defined, wear particle-induced, infectious, combined and indeterminate type25). Nevertheless, the nature and degree of infiltration with inflammatory cells may vary markedly among specimens and even within individual tissue sections from the same patient. There is no comprehensively accepted definition about acute inflammation; normally an acute inflammation has been variably defined as from ≥1 to ≥10 neutrophils per high-power field at a magnification of 40012). Unfortunately, though histopathological test has high value in diagnose PJI, it does not identify the causative bacteria. The CD15 focus score values can differentiate low-virulence and high-virulence microbes with high accuracy26).
3. Microbiological Studies
1) Preoperative aspiration
The synovial fluid culture has a sensitivity ranging from 50% to 70% and should be performed before revision surgeries (together with the determination of leukocyte count in the synovial fluid).
2) Intraoperative specimens
Intraoperative tissue samples provide accurate specimens for detecting the infecting microorganism(s), sensitivity ranging from 45% to 78%, and specificity from 91% to 96%232527). At least three to five intraoperative tissue samples from different anatomical sites should be sampled for culture. Samples should always be collected from a zone in which the tissue structure is visibly inflamed, because it is informative. Prior to collecting microbiological samples, any antibiotic regimen should be discontinued for 2 weeks to progress the disease28).
3) Sonication for removed implant
Sonication is used for dislodging adherent microorganisms from the surface of prosthetic joint. The sonication fluid culture proves the higher sensitivity and specificity than periprosthetic tissue culture which is also valid at the patient who has received antibiotic treatment before surgery. Discontinued antibiotic therapy within 14 days will have higher sensitivity27). A study29) about inoculation of sonication fluid in blood culture bottles (BCB) greatly improves the result, even when the patients received antibiotics. The sonication fluid in BCB has 100% sensitivity and specificity, even the half of patients received antibiotics within 14 days. But the sensitivity is 87% for conventional synovial fluid culture and 59% in tissue culture. The sonication fluid in BCB also reduces the culture time; it detects all bacteria in only 5 days. Another study demonstrated that the sonication fluid in BCB has better sensitivity than agar plate culture and also reduces the culture time than agar plate30). But why sonication fluid in BCB increases the sensitivity is still unclear. The method of sonication fluid in BCB still need more clinic practice to find some details about this research.
4. Imaging Studies
Conventional radiography is the most used in the first-step imaging diagnosis of PJI17). However, the sensitivity and specificity of X-ray plain film in the diagnosis of infection are low, and it is difficult to distinguish between aseptic loosening and PJI31). Computed tomography (CT) imaging occupies good contrast resolution of bone and surrounding soft tissue. Magnetic resonance imaging (MRI) can be used safely on patients with non-ferrimagnetic implants. MRI displays greater resolution for soft tissue abnormalities than CT and radiography and does not involve radiation. However, the patients must remain in an enclosed machine, which may be extremely problematic for claustrophobic patients. The main disadvantage of CT and MRI is imaging interference in the vicinity of metallic orthopedic implants. Fluorine 18-fluorodeoxyglucose (FDG) positron emission tomography (PET) is a fast, safety, high-quality imaging for detection of PJI32). One meta-analysis report33) pooled sensitivity and specificity of FDG-PET for the diagnosis of prosthetic hip or knee joint infection were 82.1% and 86.6%.
5. New Diagnostic Methods
Polymerase chain reaction (PCR) techniques can identify an isolated bacterium and some difficult-to-cultured bacteria. When the patient receives antibiotics, the sensitivity and specificity are still high by multiplex PCR for diagnosis PJI and to distinguish aseptic loosening34). According to a meta-analysis of 14 studies35), the sensitivity and specificity of PCR in synovial fluid samples were 84% and 89% and the PCR in sonication fluid culture were 81% and 96% for the detection of PJI. The sensitivity in fresh samples was better than using frozen samples.
The alpha defensin lateral flow (ADLF) is a rapid biomarker for test PJI, but the sensitivity and specificity are a controversial idea363738). In a recent study16), the ADLF test was detected PJI with sensitivity and specificity in the criteria of MSIS 84.4% and 96.4%, IDSA 67.3% and 95.5%, and EBJIS 54.4% and 99.3%. The EBJIS criteria used for ADLF test are not a good screening diagnose to rule out the PJI, while it could be a good method to confirm PJI.
Microcalorimetry is able to be used to rapidly detect the existence of microorganisms through measuring microbial heat produced by microbial growth and metabolism. A study reports that in microcalorimetry of sonication fluid the sensitivity is 100% and specificity is 97%39).
TREATMENT
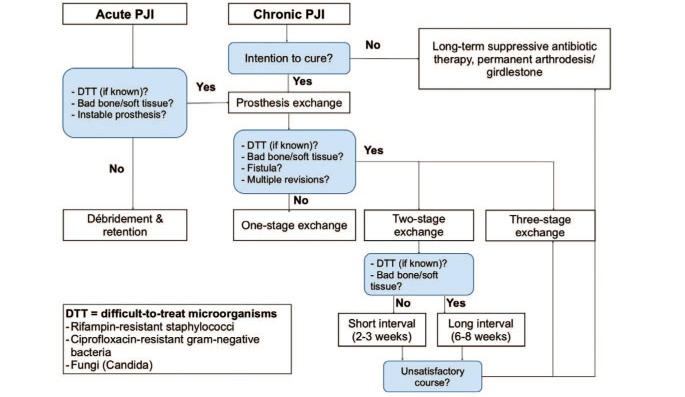
The goals of PJI treatment are to alleviate suffering, restore the normal joint function and eliminate the infection. Treatment decisions should be individualized, and involve a cooperation of a multi-disciplinary team in order to tender the best approach for each patient based on a critical review of the current information. An appropriate operation combining with antimicrobial concept is required for successful treatment. The existing recommendations for treatment of the PJI440) have been refined further by new scientific evidences and clinical experiences, as optimized and summarized in a surgical and antibiotic treatment algorithm in Fig. 1.
1. Surgical Therapy
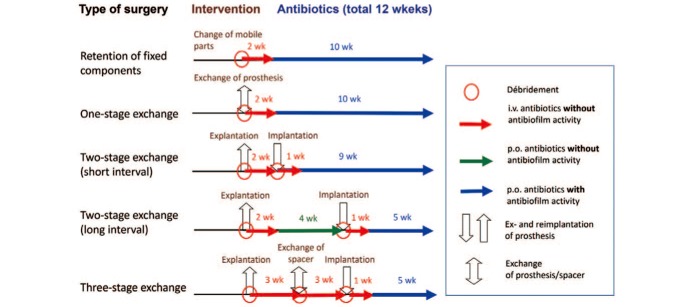
Major surgical strategy for the treatment of PJI includes; débridement and implant retention, one-stage or two-stage implant replacement (Fig. 2).
1) Débridement with retention
Early studies of débridement combining with retention strategies to treat prosthetic joint infection have high failure rates41). However, success rates can be greater than 80% when the following conditions are met42): (1) prosthesis is stable; (2) a pathogen with susceptibility to antimicrobial agents is active against surface-adhering microorganisms; (3) there is no sinus tract or compromised soft tissue; (4) symptom duration of infection is less than 3 weeks. Based on a recent report43), 90% of orthopedic device-related infections are successfully cured by surgical débridement and implant-retention plus antimicrobial therapy according to a predefined treatment algorithm, if patients fulfill the above selection criteria and the pathogen is susceptible to rifampin (for gram-positive pathogens) or ciprofloxacin (for gram-negative pathogens).
2) One-stage implant replacement
One-stage exchange is a single operation, which includes the removal of the old and reimplantation of a new prosthesis. The operation is mostly used in Europe, whereas two-stage replacement is often used in United States513). One-stage exchange is suitable for patients who have good bone conditions and soft tissue without sinus tract, as well as known bacteria with no difficult-to-treat (DTT) infections caused by pathogens resistant to biofilm-active antimicrobials42). If based on the indication, the success rate of one-stage exchange could be reach 100%44). In a single center report45), the success rate of one-stage replacement is from 85% to 90% over 35 years. The one-stage exchange is an effective surgery with high success rate, earlier mobility, shorter period of hospitalization and less cost than two-stage exchange.
3) Two-stage implant replacement
It includes removal of the prosthesis and subsequently delayed reimplantation of a second prosthesis. The approach of short interval (2–4 weeks) is suitable for patients who have known and easily treatable organism, compromised soft tissue or sinus tract. The approach of long interval (8 weeks) is suitable for the organism which is unknown or DTT and strongly compromised soft tissue. Two-stage exchange is identified as a golden standard to treat the patients13), especially in DTT microorganisms such as enterococci or fungi, etc. The success rate of two stage usually >90%4), but the reinfection is important and easy to be ignored question, and the incidence of reinfection in one and two stage according to a meta-analysis shows 8.2% versus 7.9% (95% confidence intervals)46). If more than three morbidities and a high ESR or CRP is present before reimplantation, the risk of reinfection is high47).
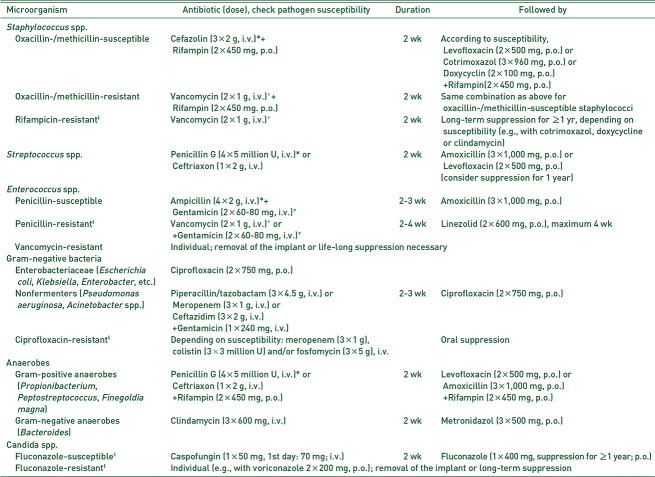
2. Antimicrobial Therapy
For all surgical procedures, a total duration of antibiotic treatment of 12 weeks is recommended (Fig. 2). Antibiotic treatment without surgery is not recommended and should be only performed, if the patient refuses surgery or the surgical procedure is associated with high risk for patient life. In this case, antibiotic suppression might be considered.
OUTLOOK
Diagnosis and treatment of PJI are still difficult and have a lack of an universal definition. In order to successfully prevent and treat PJI as well as preserve implant functions in the future, PJI management must contain the effective, timely and individualized diagnosis and treatment with interdisciplinary collaboration. On the other hand, research and development of new diagnostic methods with more accuracy, simplicity, and convenience are required.

 XML Download
XML Download