

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is one of the most common malignancies worldwide [1]. Although the surgical outcomes of HCC have improved over time, there is still a high recurrence rate [234]. On the other hand, primary liver transplantation (LT) may be the optimal treatment of HCC, maximizing the evacuation of any possible hidden tumor within the liver and also replacing cirrhotic liver with a more competent liver reserve. However, organ shortage is the major obstacle to primary LT of HCC patients. Therefore, liver resection (LR) for early HCC is more frequently performed, while liver grafts from deceased donors are reserved for patients who are at high risk of death due to liver failure [567].
Nevertheless, patients who undergo LR have a risk of recurrence, and identifying optimal t reatment for recurred HCC patients after LR has always been the interest for oncologists. Salvage liver transplantation (SLT) for recurrent HCC patients after LR was first proposed by Majno et al. [8] and its efficacy has been evaluated at many centers around the world [91011]. Although there are conflicting reports on the outcomes of SLT compared to primary LT [121314], it may still be the best option for patients with recurrent HCC [15].
Currently, many centers are adapting their SLT strategy to curative intent for recurrent HCC after initial LR [8111617]. However, there is not enough evidence to provide guidance for oncologists on whether to perform locoregional therapy (LRT) or SLT under certain circumstances. As a center with substantial experience in SLT, we designed this study to analyze which factors are related to the success of SLT.
METHODS
Patients and data
Patients who underwent SLT for recurrent HCC after LR from November 1996 to May 2017 were included as study subjects. Our center uses expanded criteria for LT, which limits the size up to 6.5 cm and the number of 5 tumors. Patient data were retrospectively reviewed based on our prospectively updated database for LT. Patient demographic, clinical and pathologic characteristics, operative data, hospital course and follow-up data regarding initial LR, LRT after recurrence and SLT were reviewed. Data were collected according to three time points: initial LR, concurrent recurrence after initial LR, and SLT. Pathological data were only available at initial LR and SLT. Exclusion criteria were as follows: patients who underwent SLT for liver failure without HCC recurrence; patients who were diagnosed as having no viable tumor in the extracted liver during SLT; patients who underwent deceased donor LT; and patients who underwent LRT instead of surgery more than 6 months prior to initial LR.
This study was approved by the Institutional Review Board of Samsung Medical Center for not receiving informed consent from the patients (approval number: 2017-06-113).
Statistical analysis
Prognostic factors for recurrence-free survival were analyzed. Potential prognostic factors included interval between initial LR and concurrent recurrence and clinical and pathological data at SLT. Recurrence-free survival was analyzed using Kaplan-Meier survival analysis. Prognostic factors were analyzed using Cox proportional hazard ratio. Multivariate Cox analysis was done including factors with P-value under 0.1 in the univariate analysis. Statistical significance was indicated by a 2-tailed P-value of <0.05. To analyze the prognosis related to the number of LRT performed, patients were divided into 2 groups by analyzing the receiver operation curve and finding the point where they showed the most appropriate sensitivity and specificity on predicting the recurrence within 1-year posttransplantation.
All statistical analyses were performed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA).
RESULTS
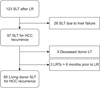
Among 123 patients who underwent SLT after LR, 85 patients were included as study subjects (Fig. 1). Twenty-six patients were excluded because they underwent SLT without evidence of HCC recurrence in the extracted liver. Nine patients with deceased donor LT were excluded. Three patients were also excluded because they had LRT more than 6 months prior to initial LR.
Initial LR
Table 1 summarizes the demographic, clinical, and pathological characteristics of patients at initial LR. Seventy-seven patients were male and 8 patients were female, and mean age was 48.1 ± 9.0 years. The mean model for end-stage liver disease (MELD) score was 7.87 ± 1.69. Nineteen out of 82 patients (23.2%, data of Milan criteria were absent in 3 patients) did not meet the Milan criteria. Median α-FP was 43.0 ng/mL (interquartile range [IQR], 208.8 ng/mL) and 12 patients (14.1%) were above 1,000 ng/mL. Mean tumor size was 4.05 ± 2.96 cm, and 20 patients had a tumor size greater than 5 cm (24.4%). Thirteen patients (16.3%) had multiple HCCs, and microvascular invasion was present in 43 patients (56.6%). A total of 5 patients (5.9%) underwent LR within 6 months after their first radiofrequency ablation.
Recurrence after Initial LR
Table 2 summarizes the clinical characteristics of patients at the time of recurrence after initial LR. The mean model for MELD score at the time of recurrence was 8.78 ± 3.40. There were 8 patients with a median α-FP ≥ 1,000 ng/mL. Median recurrence-free duration was 12.7 months (IQR, 19.7 months), and 50 patients (58.8%) had a recurrence-free duration ≥ 8 months. All the recurrences were intrahepatic. While 13 patients (15.3%) did not undergo additional LRTs after the recurrence, nearly half of the patients (n = 42, 49.4%) underwent five or more LRTs after recurrence. Transcatheter arterial chemoembolization was the mostly performed LRT (78.8%). Other LRTs included radiofrequency ablation (28.2%), radiotherapy (2.4%), and additional LR (2.4%). Viable tumors were detected in the 1-month post-LRT imaging on 143 out of 299 LRTs (47.8%), while the other LRTs showed successful removal of tumor after 1-month post-LRT.
Salvage liver transplantation
Table 3 summarizes the clinicopathologic characteristics of patients at the time of SLT. Mean age at SLT was 51.5 ± 9.4 years. Mean MELD score was 9.93 ± 5.07. Thirty-eight patients (44.7%) did not meet the Milan criteria. Median AFP was 9.5 ng/mL (IQR, 146.9 ng/mL) and 7 patients (9.4%) were above 1,000 ng/mL. Mean tumor size was 2.60 ± 1.70 cm and 8 patients (9.4%) had a tumor larger than 5 cm. Fifty-eight patients (68.2%) had multiple tumors. Microvascular invasion was present in 63 patients (74.1%).
Thirty-three patients (38.4%) experienced recurrence after SLT. The median recurrence-free duration in recurred patients was 7.4 months (IQR, 12.9 months), while median recur-free duration of total patients was 15.9 months (IQR, 45.9 months). While 9 patients (27.3% of recurrence) had intrahepatic recurrence, 24 patients (72.7% of recurrence) had extrahepatic recurrence. The most common site of extrahepatic recurrence after SLT was bone (n = 10) followed by lung (n = 8) and lymph nodes (n = 4). Twenty-nine patients (34.1%) expired after SLT; Twenty-one deaths (24.7%) were related to tumor recurrence and 8 deaths were related to graft failure with or without multiple organ failure.
Kaplan-Meier survival analyses showed that recurrence-free survivals were 69.7%, 50.5% and 44.9% after 1, 5, and 10 years, respectively, after SLT. Overall survivals were 85.0%, 61.3%, and 54.6% after 1, 5, and 10 years after SLT.
Prognostic factors for recurrence-free survival
Table 4 shows the multivariate Cox proportional hazard ratio including potential prognostic factors related to recurrence-free survival after SLT. Patients who had 5 or more LRTs prior to SLT had significantly poorer recurrence-free survival compared to patients who had less than 5 LRTs prior to SLT (hazard ratio [HR], 3.74; 95% confidence interval [CI], 1.45–9.64; P = 0.006). Patients who did not meet the Milan criteria at the time of SLT were at significant risk of recurrence compared to patients who met the Milan criteria (HR, 2.66; 95% CI, 1.26–5.63; P = 0.011). Patients whose AFP level ≥ 1,000 ng/mL at the time of recurrence after initial LR (HR, 6.48; 95% CI, 1.83–22.92; P = 0.004) and at the time of SLT (HR, 3.43; 95% CI, 1.28–9.18; P = 0.014) were at significant risk of recurrence after SLT. Patients who were hepatitis B carriers had significant risk compared to those who do not (HR, 9.20; 95% CI, 1.13–74.89; P = 0.04). Fig. 2 shows the recurrence-free survival curves of patients divided by number of LRTs, Milan criteria, and AFP level.
Comparison between patients divided by 5 locoregional therapties
Table 5 shows the comparisons of clinicopathological characteristics of the patients divided by five LRTs before SLT, both at the time of initial LR and at the time of SLT. At the time of initial LR, there were no statistical difference between patients who underwent four or less LRTs and patients who underwent five or more LRTs. On the other hand, there were statistical differences in microvascular invasion (60.5% in LRT < 5 vs. 88.1% in LRT ≥ 5, P = 0.006) and Union for International Cancer Control (UICC) stage (P = 0.011). Patients in the LRT < 5 group had 56.1% of microvascular invasion at the time of initial resection while 60.5% had microvascular invasion at the time of SLT. In comparison, patients in the LRT ≥ 5 group had 57.1% of microvascular invasion at the time of initial LR whereas it was increased to 88.1% at the time of SLT. While 12.2% and 14.7% of LRT < 5 and LRT ≥ 5 groups had UICC T4 stage at the time of initial LR, respectively, it was increased to 30.2% and 50.0% at the time of SLT. Proportion of patients outside Milan criteria increased from 27.9% to 37.2% in the LRT < 5 group and from 17.9% to 52.4% in the LRT ≥ 5 groups. There was no statistical difference between the 2 groups both at the initial LR (P = 0.286) and at the time of SLT (P = 0.160). Multiplicities of tumor were 16.3% and 16.2% in the LRT < 5 group and LRT ≥ 5 group at the time of initial LR, respectively. It was increased to 69.8% and 66.7% in the LRT < 5 group and LRT ≥ 5 group at the time of SLT, respectively.
DISCUSSION
This study showed that the outcome of successful SLT can be influenced not only by tumor status at the time of SLT, namely whether the Milan criteria have been met or whether α-FP level is under 1,000 ng/mL, but also by the number of LRTs that have been performed for recurrent HCC after initial LR. LRTs such as transcatheter arterial chemoembolization or radiofrequency ablation are frequently performed in recurrent HCC patients. However, treatment decisions for recurrent HCC after LR vary from center to center and some patients undergo numerous therapies for continuing recurrence after LRT [1819]. In our study, mean number of LRTs performed before SLT was 4.21 ± 3.63, and 49.4% of patients underwent five or more LRTs before undergoing SLT, with the highest being 18 LRTs. Receiver operative characteristic curves performed on recurrence within 1-year post-SLT depending on number of SLTs showed that 4.5 SLTs showed the most balanced predictability (sensitivity, 0.697; specificity, 0.635; area under curve, 0.707; 95% CI, 0.594–0.921) (Supplementary Fig. 1).
Previous studies on SLT have focused on comparing the outcome of SLT to primary LT [812]. Although the outcome of SLT was poorer than that of primary LT, the results cannot justify not performing SLT for HCC recurrence. Still, SLT showed superior outcomes compared to other LRTs in recurrent HCC after LR [15]. Therefore, SLT is the best option for patients when feasible.
Our study restricted patients to those with recurrent HCC after initial LR who underwent living donor SLT. The main goal was to assess whether the patient was free from HCC after SLT. We hypothesized that the risk of tumor progression can be additive as patients exposed to recurrent HCC without definite treatment such as SLT. In other words, patients who undergo more LRTs due to recurrent HCC might be at higher risk compared to patients who experience less recurrence and consequently fewer LRTs. As we demonstrated that patients who underwent five or more LRTs are at increased risk of recurrence (HR, 3.74; 95% CI, 1.45–9.64; P = 0.006) compared to patients who underwent fewer than 5 LRTs, our hypothesis was confirmed. This may be mainly due to the progressiveness of tumor which probably increased as it continues to recur after LRTs. Of course, our study did not investigate whether LRT itself can affect any biological behaviors of the tumor. The topic is out of the scope of our study despite we showed the progressively changed biological behavior in Table 5. Table 5 shows the statistical differences, especially in microvascular invasion and UICC stage. This proves our hypothesis that the progressiveness may increase as the tumor recurs after treatment. However, the progressiveness influencing the prognosis cannot be represented as single prognostic variable. This is why we added number of LRTs as an independent variable in the multivariate analysis alongside with other proven prognostic variables.
Multivariate analysis of recurrence-free survival showed that patients outside Milan criteria (HR, 2.66; 95% CI, 1.26–5.63, P = 0.011) and AFP level ≥ 1,000 ng/mL at the time of recurrence after initial LR (HR, 6.48; 95% CI, 1.83–22.92; P = 0.004) and at the time of SLT (HR, 3.43; 95% CI, 1.28–9.18; P = 0.014), and hepatitis B carrier (HR, 9.20; 95% CI, 1.13–74.89; P = 0.04) had poorer prognosis. While the importance of Milan criteria and α-FP level as key prognostic factors was acknowledged for both primary LT and SLT, the importance of the number of LRTs that were performed prior to SLT due to HCC recurrence has not been documented in other published studies. Interesting finding was that α-FP level ≥ 1,000 ng/mL at the time of recurrence after initial LR showed higher HR compared to α-FP level ≥ 1,000 ng/mL at the time of SLT. This shows that high α-FP level in the earlier period represents more aggressive behavior.
Our center previously published a multicenter retrospective study investigating prognostic factors for SLT [11]. In that study, HCC recurrence within 8 months after LR was related to prognosis of SLT alongside α-FP level and Milan criteria. However, in this study, it was only significant in the univariate analysis. Although microvascular invasion was presented as a significant factor related to the outcomes of both primary LT and SLT, it did not have a statistically significant relationship with prognosis [1314].
This study has certain limitation because it was designed as a retrospective study. While we tried to include patients with homogenous backgrounds, there were still selection biases. Our study demonstrated that the number of LRTs performed prior to SLT can influence the outcomes of SLT. However, different effects of different treatment modalities were not taken into account. Since our center performs LT according to expanded criteria, both patients that did and did not meet the Milan and University of California, San Fransisco criteria were included in this study. However, we performed a multivariate analysis including Milan criteria to minimize potential bias. Despite the meaningful findings of our study, interpretation should be cautious and patients should be taken care with individualized treatment plan.
Our study identified a new prognostic factor related to SLT outcomes. Our results demonstrated that oncologists should be more cautious when performing LRTs for recurrent HCC after LR. For some patients there is not a donor available for SLT, and LRT is the only option. Patients who underwent five or more LRTs including LR were nearly half in our study. This reflects that 5 or more LRTs is not an excessive and deviated number. Therefore, continuing LRT more than 5 times should be reconsidered if SLT is feasible. With additional research, we believe we can establish a consensus on the number of times LRT can be performed for recurrent HCC without compromising the outcome of SLT.






 XML Download
XML Download