

 PDF
PDF ePub
ePub Citation
Citation Print
Print



서론
슬관절은 고관절과 족관절 사이에 위치하며 정상적으로 중력에 의한 체중 부하선이 관절의 중심을 지나가게 된다. 만약 하지의 정렬이 정상범위를 벗어나게 되면 슬관절의 특정 구획에 과도한 부하를 유발하게 되어 통증과 기능 저하를 유발할 뿐 아니라 결국 퇴행성 변화를 일으키게 된다.1) 교정 절골술은 하지의 정렬 이상과 슬관절의 퇴행성 변화를 보이는 환자에서 비정상적인 역학적 축을 교정함으로써 병변부에 가해지는 하중을 분산시키는 수술 방법으로 인공관절 치환술과는 달리 수술을 통해 환자의 통증을 줄이고 퇴행성 변화를 지연시켜 슬관절을 보존하여 수명을 연장시킨다는 차이점이 있다. 이러한 장점 때문에 나이가 비교적 젊은 환자에서 슬관절 주위 단일 구획 관절염의 치료에 근위 경골 절골술과 원위 대퇴골 절골술이 사용되고 있고, 좋은 결과를 보고하고 있다.23456789)
슬관절 변형의 대부분을 차지하는 내반 변형의 경우 근위 경골절골술을, 상대적으로 드문 슬관절 외반 변형의 경우 원위 대퇴골 절골술을 선택하여 교정을 하는 것이 절골술의 기본적인 원칙으로 알려져 있다.1011) 하지만 교정각이 너무 크거나 경골 및 대퇴골에 모두 변형이 있어 근위 경골 절골술이나 원위 대퇴골 절골술 어느 하나만으로는 적절한 교정을 얻지 못할 경우, 이중 절골술 역시 고려해 볼 수 있다.1213) 그러나 환자 선택 및 교정각도가 적절하지 못한 절골술을 시행할 경우, 오히려 나쁜 결과를 초래할 수 있다. 본 종설에서는 슬관절 주위 절골술을 올바르게 시행하기 위한 환자의 선택 및 수술 전 계획의 원칙과 최신 지견 등에 대해 살펴보고자 한다.
본론
1. 하지의 축
하지의 역학적 축은 기립 전후면 하지 전장 방사선 사진에서 대퇴골 두의 중심점부터 거골 원개의 중심점까지 연결한 직선으로 정상적으로 경골의 중심점을 지나가게 된다.14) 정상 슬관절에서는 내측 구획에 60%–70%의 체중이 부하되어 내측 구획이 외측 구획보다 골관절염의 진행이 더 많다.15) 양측 고관절 사이의 간격이 슬관절 사이의 간격보다 넓기 때문에 하지의 역학적 축은 지면에 수직인 선에 대하여 3도 내반되어 있다.161718) 하지의 역학적축이 슬관절의 중심을 지나지 않고 내측으로 통과하는 경우를 역학적 내반 정렬이라 하고, 외측으로 통과하는 경우를 역학적 외반 정렬이라 한다(Fig. 1).14)
대퇴골의 역학적 축은 대퇴골 두의 중심부터 과간 절흔의 중심점까지 연결한 선이며 경골의 역학적 축은 경골 고평부의 중심부터 경골 천장부의 중심까지 연결한 선이다.19) 대퇴골과 경골의 해부학적 축은 각각 대퇴골과 경골 간부의 축으로 평균 6도의 외반을 이루고 있다. 대퇴골의 역학적 축과 해부학적 축은 평균 6도의 각을 이루고 있으며, 경골의 역학적 축과 해부학적 축은 거의 일치한다.20) 대퇴골의 내과와 외과의 관절면을 이은 선과 대퇴골의 역학적 축이 이루는 각인 역학적 외측 원위 대퇴각은 평균 88도를 이루고 있고, 대퇴골의 관절면을 이은 선과 대퇴골의 해부학적 축이 이루는 각인 해부학적 외측 원위 대퇴각은 평균 81도를 이룬다.21) 경골의 고평부선과 경골의 역학적 축이 이루는 경골의 역학적 내측 근위 경골각은 정상적으로 평균 87도의 각을 갖고 족관절선과 경골이 이루는 역학적 외측 원위 경골각은 평균 89도를 이룬다(Fig. 2).1122)
하지의 정렬 이상에서는 이와 같은 하지의 생리적 축과 생리적각들이 정상 범위를 갖지 않고, 정렬 이상의 종류에 따라 비정상적인 값을 갖는다. 수술 전 방사선 사진을 통한 정확한 평가를 통해 정렬 이상의 원인을 찾아 변형이 있는 부위에서 절골술을 시행하는 것을 원칙으로 교정 부위와 교정 각도 등의 술 전 계획을 세울 수 있다.12)
2. 근위 경골 절골술
1) 환자의 선택
(1) 나이
현재 환자 나이에 따른 근위 경골 절골술의 결과에 대해 합의된 결과는 없는 실정이다. 일부 보고들에 따르면 65세 이상으로 나이가 많을 경우 10년 생존율이 감소한다고 하지만,23242526) 나이가 생존율에 영향을 미치지 않는다는 반대되는 보고도 존재한다.272829) 일반적으로 술자들이 나이 많은 환자군에서 실패율이 높을 것이라고 믿는 경향이 있기 때문에 적응증을 좀 더 좁게 잡는 경향이 있는 것으로 보인다.924) 이처럼 저자들에 따라 결과의 차이가 있기 때문에 나이의 적응증을 잡을 때, 실제 나이보다는 생리학적 나이를 고려하는 것이 더 중요하다고 생각된다.
(3) Osteoarthritis 등급
근위 경골 절골술에서 내측 구획 골관절염의 정도는 술 후 결과에 영향을 미치는 중요한 요소 중 하나이다. 연골손상이 내측에 국한되어 있을 때 술 후 좋은 결과를 기대할 수 있지만, 심한 골관절염에서는 수술 후에도 내측에 통증이 지속될 수 있다.3738) 특히 슬개 대퇴관절염이 있거나 삼중 구획 골관절염까지 진행된 경우는 절골술의 금기증에 해당한다.1839) Ahlbäck40)이 제안한 골관절염의 분류에 따르면, 3등급 이상인 경우 결과가 좋지 않고,23) 0등급일 때 보다 나은 결과를 보인다고 하였다.9) 자기공명영상(magnetic resonance imaging, MRI)은 단일 구획 관절염의 환자에게 있어 연골손상 및 동반된 다른 질환을 확인하고 외측 연골판의 손상 여부를 평가하기 위해 시행할 수 있다.
(4) 관절운동 범위
근위 경골 절골술을 시행하기 전에 관절운동 범위를 검사해보아야 한다. Berman 등42)은 술 전 관절운동 범위가 90도 이하인 경우 술 후 결과가 좋지 않다고 보고하였다. Akizuki 등43)은 술 전 관절운동 범위 100도를 술 후 좋은 결과를 나타내는 기준점으로 보고 하기도 하였다. 많은 골관절염을 가지고 있는 환자들은 굴곡구축이 있으며 절골술을 통해 10도 이하의 굴곡구축은 교정할 수 있지만 10도 이상의 굴곡구축이 있는 경우는 근위 경골 절골술 후후방 경골 경사의 변화로 전후방 십자인대에 나쁜 영향을 미쳐 만족할 만한 수술 결과를 기대하기 어렵다.
(5) 슬관절 불안정성
슬관절 불안정성이 동반된 정렬 이상의 경우가 있을 수 있으므로 근위 경골 절골술을 시행하기 전에 인대 상태에 대한 검사가 필요하다. 후방 경골 경사의 변화는 관절운동 범위 및 전후방 십자인대의 상태에 따라 술 전 계획 및 술 후 결과에 영향을 미칠 수 있다. 즉 내측 개방형 경골 근위부 절골술에 의한 후방 경골 경사의 증가는 과신전의 감소 및 후방 불안정성의 감소(굴곡 구축의 증가 및 전방 불안정성의 증가) 효과를 가져올 수 있다.44) 반대로 외측 폐쇄형 경골 근위부 절골술에 의한 후방 경골 경사의 감소는 과신전의 증가 및 후방 불안정성의 증가(굴곡 구축의 감소 및 전방 불안정성의 감소) 효과를 가져올 수 있다.44)
아급성 전방 십자인대 손상과 내반 변형이 동반된 경우 근위 경골 절골술과 전방 십자인대 재건술을 동시에 시행하는 것이 권장된다.4546) 만성 전방 십자인대 손상과 내반 변형이 동반된 경우에는 근위 경골 절골술만 시행하거나 전방 십자인대 재건술을 같이 할 수 있는데, 환자의 나이와 활동성을 고려하여 결정한다.4546) 후방 십자인대 손상이나 후외측 구조물의 손상으로 만성 후외측 불안정성이 동반된 경우에는 근위 경골 절골술만 먼저 시행하고, 만약 불안정성이 술 후에도 지속된다면 후방 십자인대와 후외측구조물 재건술을 시행하는 것을 고려한다.47)
(6) 체질량지수
Flecher 등23)은 체질량지수가 30 kg/m2 미만인 경우, 근위 경골 절골술 후의 결과가 더 좋다고 보고하였다. Giagounidis와 Sell48)은 체질량지수가 정상보다 10% 이상 높을 경우 술 후 통증이 없는 기간이 5년, 체질량지수가 정상보다 10% 미만으로 높을 경우 술 후 통증이 없는 기간이 7.8년이라고 보고하였다. 이와는 반대로 Naudie 등25)은 체질량지수가 25 kg/m2 미만인 환자에서 근위 경골 절골술 후 더 나쁜 결과를 보인다고 보고하였는데, 이는 가벼운 사람이 더 활동적이어서 절골술 부위에 더 많은 부하가 걸리기 때문이라고 주장하였다. 이처럼 체중과 골 관절염 발생에 대한 논쟁은 아직까지 진행 중이며 보통 비만 환자의 경우 슬관절에 더욱 부하가 가해지는 것은 사실이다.
2) 수술 전 계획
과소한 혹은 과다한 교정을 피하기 위해서 수술 전 계획을 바르게 세우는 일이 필요하다.
(1) 방사선 검사
술 전 방사선적 평가를 위해 여러 촬영이 필요한데, 슬관절을 완전히 신전한 상태에서 하지 정렬 평가를 위한 양측 장하지 체중 부하전후방 촬영이 반드시 포함되어야 한다. 이 때 하지의 정렬이 중요하며 일반적으로 양하지 체중 부하된 상태로 발의 위치는 약간 내회전, 슬개골은 대퇴골과의 중심에 위치해야 한다.4950) 또 관절염의 평가를 위해 양측 체중 부하 전후방 및 진성 외측 촬영, 45도 골곡 양측 체중 부하 촬영인 Rosenberg view와 sky line view를 촬영하여야 한다.51) 내측 구획 골관절염의 정도 및 슬개골의 높이는 전후방 촬영에서 Insall-Salvati, Blackburne-Peel, Carton-Deschamps index52)를 이용하여 평가할 수 있고, 슬개골 고위가 있는 경우 경골결절 절골술을 동반하기도 한다. MRI는 연골 손상, 인대 손상, 골연골 결손, 골괴사, 연골하 부종 등을 확인하는 데 도움을 준다
(2) 고위 경골 절골술의 목표
내반 변형의 교정 목표 및 수술 전 계획 방법은 저자에 따라 다양하다. Coventry53)는 해부학적 대퇴경골각을 8도 외반으로 과교정할 것을 주장하였고, Hernigou 등54)은 역학적 축을 3–6도 외반으로 교정할 것을 주장하였다. Fujisawa 등18)은 술 후 역학적 축이 경골고평부의 내측에서부터 60%–70% 지점을 지나야 한다고 보고하였다. Miniaci 등55)은 경골 고평부의 30%–40% 지점을, Dugdale 등56)은 경골 고평부의 62.5%를 지나야 한다고 보고하였으며 Fujisawa 등18)이 언급한 방법에 따라 위치를 계산하였다. 최근 Jakob과 Jacobi57)는 내측 구획의 연골 두께에 따라 교정 정도를 조절하여야 한다고 주장하였다. 만약 내측 연골의 1/3이 손상되었다면 역학적 축은 경골 고평부 중심에서 외측으로 10%–15% 지점을 지나야 하고, 내측연골의 2/3가 손상되었다면 20%–25% 지점을, 내측 연골이 모두 손상되었다면 30%–35% 지점을 지나야 한다고 보고하였다.
(3) 관상면에서 술 전 교정 계획
① Miniaci 방법: 수술 후 교정선이 대퇴골 두의 중심에서 술자가 원하는 체중 부하 위치로 경골 고평부를 지나면서 족관절까지 가도록 선을 그린다(Line A). 근위 경골 절골술의 경첩점에서 족관절의 중심까지 선을 그리고(Line B), 경첩점에서 Line A가 교차하는 선을 그린다(Line C). Line B와 Line C가 이루는 각도가 Miniaci 방법으로 계획된 교정각이다(Fig. 3).55)
② Dugdale 방법: 대퇴골 두의 중심에서 경골 고평부의 62.5% 지점까지 선을 그린다(Line A). 다음으로 족관절의 중심에서 경골고평부의 62.5%까지 선을 그린다(Line B). Line A와 Line B가 이루는 각도가 Dugdale 방법으로 계획된 교정각이다(Fig. 4).56)
③ 체중 부하 단속 촬영법(weight bearing scanography)을 이용한 방법: 체중 부하 단속 촬영을 한 후, 이를 실제크기로 출력한다. 절골술을 시행할 부분을 자른 후 62%–65% 사이로 체중 부하 목표점이 지나도록 선을 그리고 회전시킨다. 절골술 부분의 크기를 자를 이용하여 직접 측정을 하여 교정 정도를 계획할 수 있다(Fig. 5).58)
④ 수술 중 하지 정렬을 확인하는 방법: 수술을 하는 도중에 수술 전 계획에 맞게 하지 정렬 교정이 되는지를 확인하는 것이 필요하다. 수술 중 하지 정렬을 확인하기 위해 cable이나 rod를 이용하는 방법이 고전적으로 사용되고 있으나 정확도 및 재현성에 문제점이 있다. 최근 사용되고 있는 항법 장치 시스템(navigation system)은 수술 중 실시간으로 해부학적 위치에 대한 정보를 제공하여 원하고자 하는 교정각을 보다 정확하게 얻을 수 있고, 오차 범위 및 이상치를 줄이며 교정의 정밀도를 향상시킬 수 있는 장점이 있다.585960) 하지만 임상적인 결과에 대해서는 추가적인 연구 및 장기 추시가 필요하다.
(4) 시상면에서 술 전 교정 계획
후방 경골 경사가 증가하면 굴곡 구축이 발생하고 경골의 전방 전위 및 전방 십자인대의 인장력을 증가시켜 후방 십자인대 결손시 나타나는 경골의 후방 아탈구가 감소하게 된다. 반대로 후방 경골 경사가 감소하면 과신전이 발생하고 후방 전위 및 후방 십자인대의 인장력을 증가시켜 전방 십자인대 결손 시 나타나는 경골의 전방 아탈구가 감소하게 된다.6465) 즉 후방 경골 경사를 조정하여 굴곡 구축 및 과신전과 같은 슬관절 변형을 교정할 수 있다는 것을 고려해야 하겠다. 하지만 후방 경골 경사가 10도 이상 증가하게 되면 전방 십자인대에 가해지는 힘이 3배 이상 증가하므로 주의해야 한다.66)
3. 원위 대퇴골 내반 절골술
1) 환자의 선택
원위 대퇴골 내반 절골술의 주된 적응증은 슬관절의 외측 구획에만 국한된 골관절염이 외반 변형과 동반된 경우이다.707172) 또 다른 적응증으로는 만성 내측 측부인대 부전으로 인한 인대 불안정성으로 외반 견인을 감소하기 위한 경우가 있고,46) 외반 변형으로 인한 슬개 대퇴 부정정렬을 교정하기 위해 시행하는 경우가 있다.73) 그 외에도 구루병, 신성 이영양증, 소아 마비, 기타 외상이나 근육 신경 질환에 의한 외반 변형 등에서 고려해볼 수 있다.2274) 원위 대퇴골 내반 절골술의 1차 적응증은 퇴행성 관절염과 외반변형이 동반되어 심한 통증을 호소하는 경우지만 최근에는 인대재건술, 연골 이식이나 반월연골판 동종 이식 등의 수술에서 수술 후 최상의 결과를 얻기 위해 함께 시행되기도 한다.
2) 수술 전 계획
(1) 방사선 검사
술 전 방사선적 평가를 위해 여러 촬영이 필요하다. 먼저 기본적인 슬관절의 진성 전후면과 측면 촬영을 시행하며, 슬관절 양측 구획의 퇴행성 변화를 평가하기 위해 슬관절을 45도 굴곡하여 체중 부하한 상태에서 후방에서 전방으로 촬영하는 Rogenberg view와 sky line view를 찍어야 한다. 또 슬관절을 완전히 신전한 상태에서 하지 정렬 평가를 위한 양측 장하지 체중 부하 전후방 촬영을 반드시 시행해야 한다. 만약 인대 불안정성이 의심되면 스트레스 촬영을 시행할 수 있고, 교정각 결정 시 인대 이완을 고려해야 한다.
(2) 원위 대퇴골 내반 절골술의 목표
원위 대퇴골 절골술의 교정각을 결정하는 방법에 대해 아직 일치된 의견은 없다. 역학적 대퇴 경골각이 1–3도 혹은 해부학적 대퇴경골각이 6–10도로 역학적 축이 슬관절의 내측을 지날 것을 권장하거나 하지의 역학적 축이 슬관절의 중심을 지나는 것이 좋다는 보고도 있다.227778798081) 원위 대퇴골 절골술이 생역학적으로 신전 상태를 교정하는 수술이기 때문에, 굴곡 상태에서 증상호전을 기대하기 어렵다. 90도 굴곡상태에서는 대퇴골 후방과에 부하가 걸리고, 이 부분은 대퇴 원위 절골술로 교정되는 부분이 아니므로 환자에게 이에 대한 설명을 미리 하는 것이 좋다.
(3) 술 전 교정계획
원위 대퇴골 절골술의 교정각은 양측 장하지 체중 부하 전후방 촬영 사진을 통해 결정할 수 있다. 대퇴골 두의 중심 A에서 족관절의 중심 B로 역학적 축을 그린다(Line A–B). 족관절의 중심 B에서 술 후 원하는 역학적 축이 경골 과간 융기 바로 내측 지점을 지나도록 Line B–C를 그린다. 이 때 Line A–B와 Line B–C의 길이는 동일해야 한다. 대퇴골 과상부 외측인 절골술의 경첩점 D에서 그린 Line A–D와 Line C–D가 이루는 각도가 교정각α가 된다. 교정각 α를 원위 대퇴골에 적용하였을 때 내측 피질골 위치에서 두 선이 이루는 사이 간격이 절골술에서 제거되는 쐐기 기저부의 길이가 된다(Fig. 6).2277)
4. 이중 절골술
관상면에서 하지의 축을 교정할 때 단일 절골술만 시행하는 경우, 과도한 관절선 경사를 만들어 관절면에 전단 부하를 증가시킬 수 있다. 또한 교정각도가 15도 이상으로 크고 경골 및 대퇴골에 모두 변형이 있는 경우 단일 절골술만으로는 좋은 결과를 기대하기 어렵다.82) 이러한 경우 고려할 수 있는 이중 절골술은 근위 경골 절골술과 원위 대퇴골 절골술을 모두 시행하는 것으로 Benjamin83)이 처음으로 제안하였다.
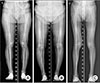
수술 전 교정 계획을 위해 체중 부하 단속 촬영이 필요하다. 체중 부하 단속 촬영 사진을 실제크기로 출력하고 대퇴골과 경골의 변형을 고려하여 절골술을 대퇴골과 경골에서 각각 개방형으로 할 것인지 혹은 폐쇄형으로 할 것인지를 결정한다.84) 절골술을 시행할 부분을 잘라 대퇴골과 경골의 변형이 교정되고 하지 정렬이 회복되도록 회전하여 교정 정도를 결정할 수 있다(Fig. 7). 또 다른 방법으로는 osteotomy analysis and simulation software (OASIS; Mayo Medical Ventures, Rochester, MN, USA)를 이용하여 수술전 계획을 세우는 방법도 소개되고 있다.85)
결론
인공관절 치환술은 진행된 슬관절의 퇴행성 관절염에서 환자의 증상을 호전시키고 술 후 빠른 통증 감소와 짧은 재활 기간 등의 장점이 있는 우수한 수술 방법이다. 하지만 모든 환자를 대상으로 시행하기에는 무리가 있고 특히 젊고 활동적이고 슬관절의 기능적 요구가 많은 환자인 경우 더욱 그러하다. 하지 정렬 이상을 동반한 단일 구획 관절염의 치료에 근위 경골 절골술과 원위 대퇴골 절골술이 좋은 결과를 보여주고 있다.35778687) 또 단일 절골술만으로 만족할 만한 결과를 얻기 힘든 경우 이중 절골술을 고려해볼 수도 있다.82) 물론 이러한 절골술을 시행할 때, 적절한 환자의 선택과 철저한 수술 전 계획이 수술의 성공을 결정하는 중요한 요소라고 할 수 있겠다






 XML Download
XML Download