

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
MATERIALS AND METHODS
Table 1
Description of applied readability assessments (based on Kasabwala et al. [2])
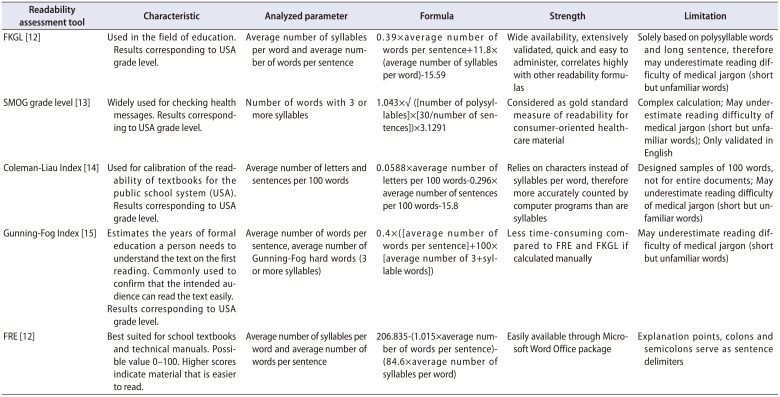
| Readability assessment tool | Characteristic | Analyzed parameter | Formula | Strength | Limitation |
|---|---|---|---|---|---|
| FKGL [12] | Used in the field of education. Results corresponding to USA grade level. | Average number of syllables per word and average number of words per sentence | 0.39×average number of words per sentence+11.8×(average number of syllables per word)−15.59 | Wide availability, extensively validated, quick and easy to administer, correlates highly with other readability formulas | Solely based on polysyllable words and long sentence, therefore may underestimate reading difficulty of medical jargon (short but unfamiliar words) |
| SMOG grade level [13] | Widely used for checking health messages. Results corresponding to USA grade level. | Number of words with 3 or more syllables | 1.043×√ ([number of polysyllables]×[30/number of sentences])×3.1291 | Considered as gold standard measure of readability for consumer-oriented healthcare material | Complex calculation; May underestimate reading difficulty of medical jargon (short but unfamiliar words); Only validated in English |
| Coleman-Liau Index [14] | Used for calibration of the readability of textbooks for the public school system (USA). Results corresponding to USA grade level. | Average number of letters and sentences per 100 words | 0.0588×average number of letters per 100 words−0.296×average number of sentences per 100 words−15.8 | Relies on characters instead of syllables per word, therefore more accurately counted by computer programs than are syllables | Designed samples of 100 words, not for entire documents; May underestimate reading difficulty of medical jargon (short but unfamiliar words) |
| Gunning-Fog Index [15] | Estimates the years of formal education a person needs to understand the text on the first reading. Commonly used to confirm that the intended audience can read the text easily. | Average number of words per sentence, average number of Gunning-Fog hard words (3 or more syllables) | 0.4×([average number of words per sentence]+100×[average number of 3+syllable words]) | Less time-consuming compared to FRE and FKGL if calculated manually | May underestimate reading difficulty of medical jargon (short but unfamiliar words) |
| Results corresponding to USA grade level. | |||||
| FRE [12] | Best suited for school textbooks and technical manuals. Possible value 0–100. Higher scores indicate material that is easier to read. | Average number of syllables per word and average number of words per sentence | 206.835−(1.015×average number of words per sentence)−(84.6×average number of syllables per word) | Easily available through Microsoft Word Office package | Explanation points, colons and semicolons serve as sentence delimiters |
FKGL, Flesch-Kincaid grade level; SMOG, Simple Measure of Gobbledygook grade level; FRE, Flesch Reading Ease.
Data from the article of Kasabwala et al. Otolaryngol Head Neck Surg 2012;147:466-71 [2].
![]()
RESULTS
Table 2
Median grade-levels of the different surveys
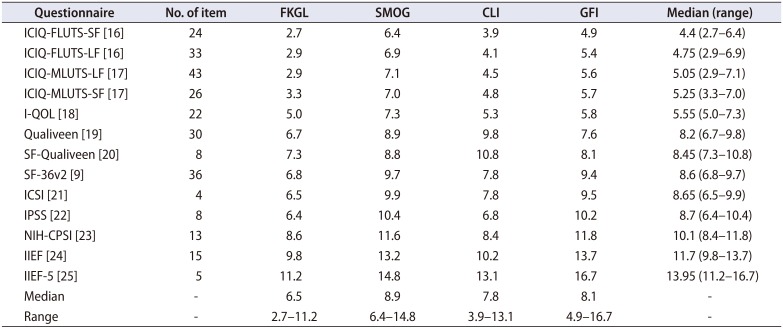
| Questionnaire | No. of item | FKGL | SMOG | CLI | GFI | Median (range) |
|---|---|---|---|---|---|---|
| ICIQ-FLUTS-SF [16] | 24 | 2.7 | 6.4 | 3.9 | 4.9 | 4.4 (2.7–6.4) |
| ICIQ-FLUTS-LF [16] | 33 | 2.9 | 6.9 | 4.1 | 5.4 | 4.75 (2.9–6.9) |
| ICIQ-MLUTS-LF [17] | 43 | 2.9 | 7.1 | 4.5 | 5.6 | 5.05 (2.9–7.1) |
| ICIQ-MLUTS-SF [17] | 26 | 3.3 | 7.0 | 4.8 | 5.7 | 5.25 (3.3–7.0) |
| I-QOL [18] | 22 | 5.0 | 7.3 | 5.3 | 5.8 | 5.55 (5.0–7.3) |
| Qualiveen [19] | 30 | 6.7 | 8.9 | 9.8 | 7.6 | 8.2 (6.7–9.8) |
| SF-Qualiveen [20] | 8 | 7.3 | 8.8 | 10.8 | 8.1 | 8.45 (7.3–10.8) |
| SF-36v2 [9] | 36 | 6.8 | 9.7 | 7.8 | 9.4 | 8.6 (6.8–9.7) |
| ICSI [21] | 4 | 6.5 | 9.9 | 7.8 | 9.5 | 8.65 (6.5–9.9) |
| IPSS [22] | 8 | 6.4 | 10.4 | 6.8 | 10.2 | 8.7 (6.4–10.4) |
| NIH-CPSI [23] | 13 | 8.6 | 11.6 | 8.4 | 11.8 | 10.1 (8.4–11.8) |
| IIEF [24] | 15 | 9.8 | 13.2 | 10.2 | 13.7 | 11.7 (9.8–13.7) |
| IIEF-5 [25] | 5 | 11.2 | 14.8 | 13.1 | 16.7 | 13.95 (11.2–16.7) |
| Median | - | 6.5 | 8.9 | 7.8 | 8.1 | - |
| Range | - | 2.7–11.2 | 6.4–14.8 | 3.9–13.1 | 4.9–16.7 | - |
FKGL, Flesch-Kincaid grade level; SMOG, Simple Measure of Gobbledygook grade level; CLI, Coleman-Liau Index; GFI, Gunning-Fog Index; ICIQ-FLUTS-SF, International Consultation on Incontinence Questionnaires (ICIQ)-Female Lower Urinary Tract Symptoms (FLUTS) short form; ICIQ-FLUTS-LF, ICIQ-FLUTS long form; ICIQ-MLUTS-LF, ICIQ-Male Lower Urinary Tract Symptoms (MLUTS) long form; ICIQ-MLUTS-SF, ICIQ-MLUTS short form; I-QOL, incontinence quality of life; SF-Qualiveen, Short form-Qualiveen; SF-36v2, SF-36 version 2; ICSI, International Cystitis Symptom Index; IPSS, International Prostate Symptom Score; NIH-CPSI, National Institutes of Health Chronic Prostatitis Symptom Index; IIEF, International Index of Erectile Function; IIEF-5, International Index of Erectile Function-short form.
![]()
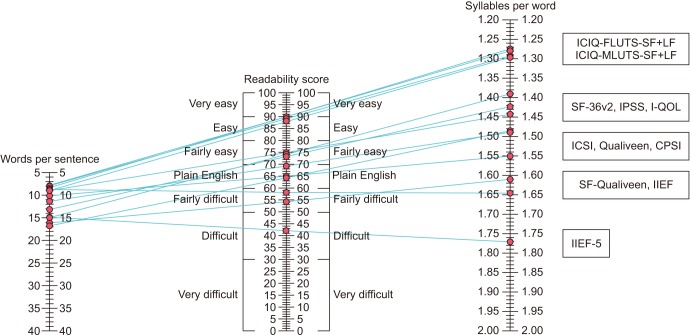 | Fig. 1Comparison of Flesch Reading Ease-scores for the different questionnaires: International Consultation on Incontinence Questionnaires-Female Lower Urinary Tract Symptoms short and long form (ICIQ-FLUTS-SF and -LF), ICIQ-Male Lower Urinary Tract Symptoms long and short form (ICIQ-MLUTS-LF and -SF), 36-Item Short Form Health Survey version 2 (SF-36v2), International Prostate Symptom Score (IPSS), incontinence quality of life (I-QOL), International Cystitis Symptom Index (ICSI), Qualiveen, Chronic Prostatitis Symptom Index (CPSI), Short-Form Qualiveen (SF-Qualiveen), International Index of Erectile Function (IIEF), IIEF-short form (IIEF-5) (‘Plain English’ is recommended for health-related content [12]).
|
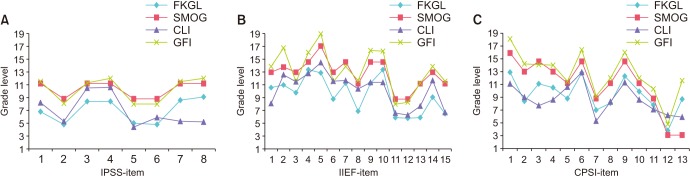 | Fig. 2Readability grade levels for single-items of the questionnaires. (A) International Prostate Symptom Score (IPSS), (B) International Index of Erectile Function (IIEF), and (C) Chronic Prostatitis Symptom Index (CPSI). FKGL, Flesch-Kincaid grade level; SMOG, Simple Measure of Gobbledygook grade level; CLI, Coleman-Liau Index; GFI, Gunning-Fog Index.
|
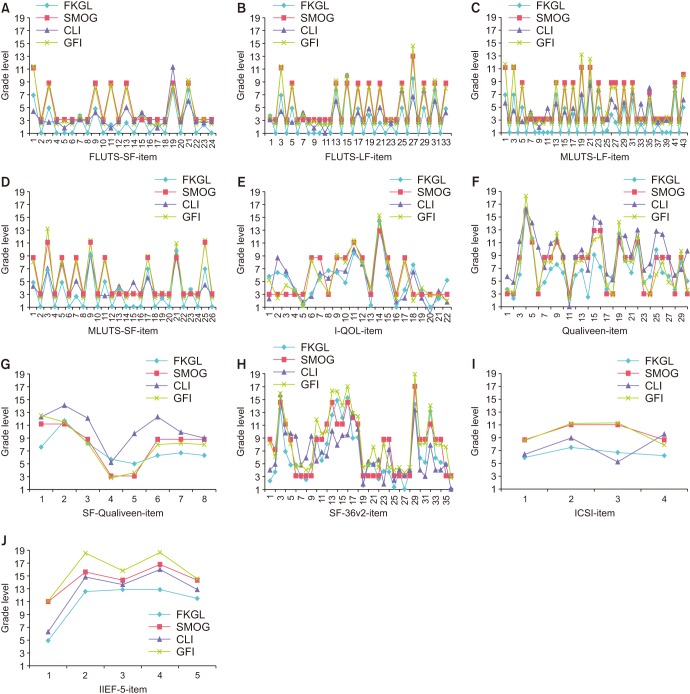 | Fig. 3Readability grade levels for single-items of the questionnaires. (A, B) International Consultation on Incontinence Questionnaires-Female Lower Urinary Tract Symptoms short and long form (ICIQ-FLUTS-SF and -LF), (C, D) ICIQ-Male Lower Urinary Tract Symptoms long and short form (ICIQ-MLUTS-LF and -SF), (E) incontinence quality of life (I-QOL), (F) Qualiveen, (G) SF-Qualiveen, (H) 36-Item Short Form Health Survey version 2 (SF-36v2), (I) International Cystitis Symptom Index (ICSI), (J) International Index of Erectile Function-short form (IIEF-5). FKGL, Flesch-Kincaid grade level; SMOG, Simple Measure of Gobbledygook grade level; CLI, Coleman-Liau Index; GFI, Gunning-Fog Index.
|
 | Fig. 4Median grade reading levels and ranges of all single-items of frequently used urological questionnaires (based on the Flesch-Kincaid grade level). SF-36v2, 36-Item Short Form Health Survey version 2; CPSI, Chronic Prostatitis Symptom Index; IPSS, International Prostate Symptom Score; IIEF, International Index of Erectile Function; ICIQ-FLUTS-SF and -LF, International Consultation on Incontinence Questionnaires-Female Lower Urinary Tract Symptoms short and long form; ICIQ-MLUTS-LF and -SF, ICIQ-Male Lower Urinary Tract Symptoms long and short form; I-QOL, incontinence quality of life; ICSI, International Cystitis Symptom Index; SF-Qualiveen, Short-Form Qualiveen.
|
 XML Download
XML Download