

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Urothelial carcinoma (UC), originating in the bladder or upper urinary tract, is the most common histological type of cancer. Approximately 151,000 new cases of UC are diagnosed annually in Europe, with 52,000 deaths per year. UC results in more than 165,000 deaths annually and is the ninth most common cancer worldwide, in accordance with the International Agency for Research on Cancer [1]. The National Cancer Institute estimated that over 79,000 new cases of UC were diagnosed in 2016, of which more than 16,000 people died in the United States (US) alone [2]; over 5,060 new cases were diagnosed in 2015 in Korea [3].
For more than 30 years, cisplatin-based combination chemotherapy has been used as the standard of care in unresectable and metastatic/advanced UC, showing an overall response rate (ORR) of 40%–50% and a median overall survival (OS) of 14–15 months [45]. However, 40%–50% of patients with metastatic UC (mUC) do not qualify for cisplatin-based chemotherapy, owing to poor performance status and impaired renal function. Thus, these patients were primarily treated with carboplatin-based regimens, presenting an ORR of 30%–40% for 9–10 months [56]. Patients with recurrence after first-line treatment, or who show progress while receiving first-line treatment, have a particularly poor prognosis. Unfortunately, second-line chemotherapies, including paclitaxel, pemetrexed, docetaxel, and vinflunine, have shown only modest efficacy with an ORR of 12% and a median OS of 5–7 months [578].
To date, several immunotherapeutic agents that block immune checkpoints, such as programmed cell death 1 receptor (PD-1) (nivolumab/pembrolizumab), PD-ligand-1 (PD-L1) (durvalumab/avelumab), and cytotoxic T lymphocyteassociated protein 4 (CTLA-4) (ipilimumab/tremelimumab), have been investigated and/or clinically used in various types of cancers, including UC. Among these, five immune checkpoint inhibitors (atezolizumab, pembrolizumab, nivolumab, durvalumab, and avelumab) have already received approval from the US Food and Drug Administration (US-FDA). Also, atezolizumab and pembrolizumab were approved by Korea-FDA for the treatment of mUC after cisplatin failure; these two drugs were also approved as the first-line treatment in patients with cisplatin-ineligible mUC. In this article, we aimed to review the current and ongoing clinical trials being performed in various clinical settings of UC, including mUC, muscle invasive bladder cancer (MIBC), and non-muscle invasive bladder cancer (NMIBC).
RATIONALE FOR IMMUNE CHECKPOINT INHIBITORS IN BLADDER CANCER
T cell-mediated immunity consists of several sequential phases: clonal selection of antigen-presenting cells and the activation, proliferation, transition, and implementation of direct effector function. These phases are controlled by equilibrium between inhibitory and stimulatory signals [9]. In a non-tumor environment, immune checkpoint proteins control the immune system and prevent autoimmunity. Immune checkpoint proteins follow inhibitory pathways that physiologically counterbalance the co-stimulatory pathways to appropriately adjust the immune responses [10].
Generally, cancer cells evade antitumor immunity by adopting active immune escape strategies as follows: (1) diminishing MHC-I expression, and hence CD8+ T cell activity; (2) defective antigen processing and presentation, thereby causing reduced recognition by T cells; and (3) increasing the expression of co-inhibitory (i.e., immune checkpoint) molecules [11]. Since most cancers select the immune checkpoints to evade the immune systemattack by blocking the effector T-cell functions, antitumor immunity may be recovered by antibodies that inhibit the receptor-ligand interaction and deactivate the immune checkpoints [12]. Currently, the most investigated and clinically related immune checkpoint molecules are PD-1, PD-L1, and CTLA-4.
The wide mutational spectrum of UC might be advantageous in establishing efficient immunotherapies for this disease, since mutations might induce more neoantigens that are recognized as ‘non-self’ by the circulating T cells, thereby inducing an immune response [13]. A recent study demonstrated that high mutational burden is observed in UC, melanoma, and non-small cell lung cancer [14]. In addition, the clinical efficacy of PD1-L1 blockade was identified to be proportional to the high tumor mutational burden, especially in melanoma and non-small cell lung cancer [1415]. Consequently, based on this cancer immunologic data, several monoclonal antibodies, that block the ligand-receptor interaction for immune checkpoints and/or its functional consequences, have been developed and clinically applied for the management of UC, including bladder and upper urinary tract cancers [16171819].
IMMUNE CHECKPOINT INHIBITORS AFTER PLATINUM-BASED CHEMOTHERAPY IN METABOLIC UC
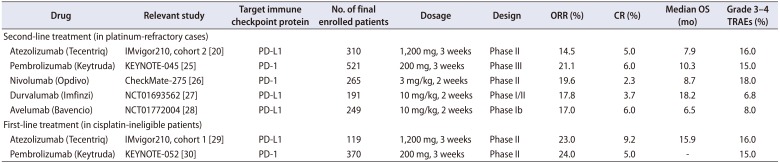
To date, the clinical trials regarding immune checkpoint inhibitors in UC have mainly focused on platinum-refractory mUC. An open-label, multi-center, single-arm, phase II IMvigor210 trial, cohort 2 (NCT02108652) assessed the clinical efficacy and safety of atezolizumab in patients with locally advanced or mUC whose disease had progressed during or following previous treatment with platinum-based chemotherapy or who had disease progression within 12 months of treatment with a platinum-based neoadjuvant or adjuvant chemotherapy [2021]. In that trial, a total of 310 patients received atezolizumab, fixed dose of intravenous 1,200 mg every three weeks. The observed ORR for all patients by independent review was 14.5%. The immune cell (IC) 2/3 subgroup (assessed by immunohistochemistry, correlating to ≥5.0% of ICs) had a clinically meaningful ORR of 26.0% versus 9.0% in the IC 0/1. The median OS was 7.9 months for the entire cohort and 11.4 months for patients with IC2/3 PD-L1 expression with a median follow-up duration of 14.4 months. Grade 3 to 4 treatment-related adverse events (TRAEs) were reported in 16.0% of the patients. Although this study was limited by phase II trial, atezolizumab received US-FDA approval for platinum-refractory mUC in May 2016 [202122]. In a recent multi-center, randomized phase III IMvigor211 clinical trial (NCT02302807), the clinical efficacy and safety of atezolizumab (1,200 mg intravenously, every three weeks) compared to chemotherapy (investigator's choice of vinflunine, paclitaxel, or docetaxel) were reported in 931 patients with mUC, whose disease had progressed despite platinum-based chemotherapy [23]. As a primary endpoint of the trial with atezolizumab, no significant improvement of OS was observed in the subset of 234 patients with ≥5% expression of PD-L1 on tumor-infiltrating ICs (median, 11.1 months vs. 10.6 months; hazard ratio [HR], 0.87; 95% confidence interval [CI], 0.63–1.21); ORR was similar (23% vs. 22%). Although a higher response rate was found with atezolizumab in patients with increased PD-L1 expression compared to that in patients with lower levels of PD-L1 expression, this patient subset also had a higher response rate to chemotherapy. Safety analysis of the intention-to-treat population found that the incidence of grade 3 to 4 TRAEs was lower with atezolizumab than with chemotherapy (20% vs. 43%), as was the incidence of treatment discontinuation (7% vs. 18%). However, the duration of response was longer in the atezolizumab group than in the chemotherapy group (15.9 months vs. 8.3 months). This long durability of atezolizumab was also identified in the IMvigor210 trial [24].
A randomized, phase III clinical trial related to pembrolizumab (200 mg every three weeks for 24 months) was performed in patients with mUC, in whom the disease had progressed during or after platinum-based chemotherapy (KEYNOTE-045 or NCT02256436) [25]. Patients were included irrespective of PD-L1 expression level. The pembrolizumab group showed significantly longer OS (10.3 months vs. 7.4 months; HR, 0.73; 95% CI, 0.59–0.91) and a higher ORR (21.1% vs. 11.4%) compared to that in the chemotherapy (paclitaxel, docetaxel, or vinflunine) group. The 12-month OS rates for the pembrolizumab and chemotherapy groups were 43.9% and 30.7%, and the 18-month OS rates were 36.1% and 20.5%, respectively. No statistically significant difference was found in progression-free survival (median, 2.1 months vs. 3.3 months; HR, 0.96%; 95% CI, 0.79–1.16). Serious TRAEs were less frequent with pembrolizumab than with chemotherapy (15.0% vs. 43.9%) [25].
A multi-center, phase II single-arm study assessing nivolumab (3 mg/kg every two weeks) in patients with platinum-refractory mUC has also been reported (NCT02387996 or CheckMate-275) [26]. The confirmed ORR was 19.6% in the entire study cohort, with a median OS of 8.7 months; this ORR was also observed (28.4%) in the PD-L1 high expression group (defined as ≥5%). Grade 3–4 TRAEs occurred in approximately 18.0% of patients [26]. Nivolumab (240 mg, intravenously, every two weeks) was approved by the FDA in February 2017. Subsequently, an alternative schedule of administering 480 mg nivolumab every four weeks was approved, based on clinical pharmacology analyses and safety assessments.
Durvalumab (10 mg/kg, intravenously, every two weeks) was injected to patients with advanced UC that had progressed during or after the previous platinumbased chemotherapy, either for metastatic disease or for progressive disease after less than 12 months of adjuvant or neoadjuvant chemotherapy (NCT01693562). In this phase I/II study, ORR in the entire cohort was 17.8%, including 9 (3.7%) with complete response (CR), and the median OS of 18.2 months. The ORR was 27.6% and 5.1% in the PD-L1 high and PD-L1 low or negative expression group, respectively, when applying a 25% cut-off value. Grade 3 to 4 TRAEs were observed in 6.8% of patients [27].
In a phase Ib trial, avelumab showed clinical efficacy in patients with platinum-refractory mUC (JAVELIN Solid Tumor trial, NCT01772004) [28]. Confirmed ORR was 17%, including 6% CR, 11% partial response (PR), and median OS 6.5 months. This ORR was observed (24%) in the high PD-L1 expression group (defined in this study as ≥5% staining of tumor cells only) [28]. Safety profiles showed a low rate of grade 3 to 4 TRAEs (8%) and no treatment-related deaths. The outcomes of the clinical trials regarding anti-PD-1 or L1 inhibitors are summarized in Table 1.
IMMUNE CHECKPOINT INHIBITORS IN PLATINUM-INELIGIBLE METABOLIC UC
Up to 50% of patients with advanced UC do not qualify for cisplatin-based chemotherapy due to age or comorbidity (i.e., impaired renal function, neuropathy, and heart failure). Although comparative phase III data are not available for a first-line setting, a phase II study supports the use of immune checkpoint inhibitors.
In a multicenter, single-arm phase II study, atezolizumab (total dose 1,200 mg, every three weeks) was used as first-line therapy in 119 patients with advanced or mUC, who were not eligible for treatment with a cisplatin-based regimen [29]. At a median follow-up of 17 months, ORR was observed in 27 patients (23%), including 11 (9%) with CR. Median duration of response was not reached, and 19 out of 27 patients continued to respond at the time of analysis. Median OS for the entire cohort was 16 months; TRAEs mirrored those used after cisplatin-based chemotherapy or in other indications [29].
In another single-arm phase II trial, the first-line use of pembrolizumab was investigated in patients with mUC who were not eligible for cisplatin-based chemotherapy (NCT02335424 and KEYNOTE-052) [30]. The ORR was 24% in all treated patients, including 5% CR and 19% PR. In particular, the high PD-L1 expression group (positive score of 10% or more) showed a high ORR (38%). Grade 3 to 4 TRAEs were observed in 15.0% of all treated patients. These results for the first-line use of an immune checkpoint in mUC are comparable to those of the existing carboplatin-based combination chemotherapy, including gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine regimens [6], in terms of efficacy and safety. On the basis of the outcomes of these phase II trials, atezolizumab and pembrolizumab have gained accelerated US-FDA approval for first-line use in cases with cisplatin-ineligible mUC. The outcomes of these trials are also summarized in Table 1.
IMMUNE CHECKPOINT INHIBITOR COMBINATIONS
Immune checkpoint inhibitors showed clinical efficacy and manageable adverse effects in advanced UC. To enhance the treatment response of immune checkpoint inhibitors and provide more effective pathway blockade in UC, several trials have been reported and various combined approaches are ongoing.
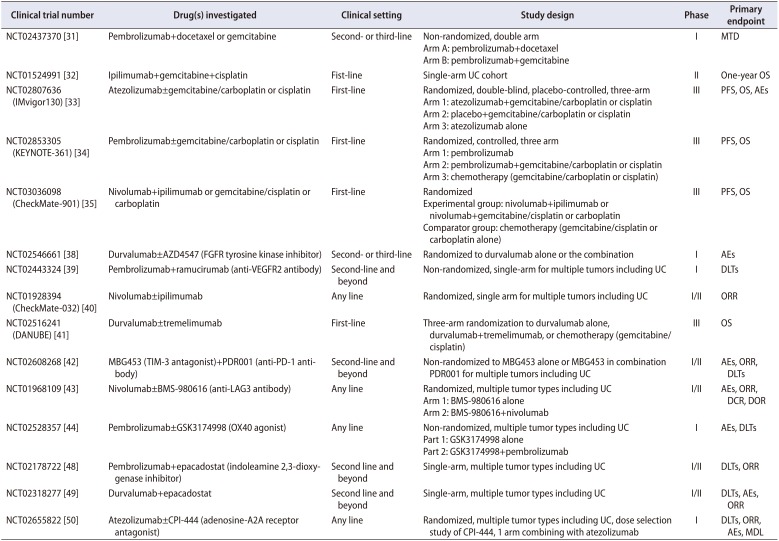
Several PD-1/PD-L1 inhibitors in conjunction with chemotherapeutic agents are being investigated for treating mUC. Theoretically, cytotoxic chemotherapy can cause tumor cell lysis, potentially enhancing immunogenicity bypromoting tumor antigen production [9]. Trials have combined pembrolizumab with gemcitabine or docetaxel (NCT02437370) [31] and ipilimumab, a CTLA-4 checkpoint inhibitor, with gemcitabine/cisplatin chemotherapy as a first-line treatment in patients with mUC (NCT01524991) [32]. Three phase III studies are currently ongoing to assess the first-line use of combined chemo-immunotherapy. The IMvigor130 trial compares atezolizumab plus gemcitabine/carboplatin vs. gemcitabine/carboplatin alone in patients with mUC who are ineligible for cisplatin-based chemotherapy (NCT02807636) [33]. The KEYNOTE-361 is a three-arm phase III study comparing pembrolizumab alone, pembrolizumab plus gemcitabine/cisplatin or carboplatin, and chemotherapy alone in patients with mUC who had not been treated with prior systemic chemotherapy (NCT02853305) [34]. The CheckMate-901 is also a multi-arm phase III trial that compares nivolumab and ipilimumab combination, nivolumab plus gemcitabine/cisplatin or carboplatin, and chemotherapy alone in previously untreated patients with mUC (NCT03036098) [35]. Patients are currently being enrolled in these trials and the forthcoming results of these trials are awaited.
Effective targeted therapies, specific to a portion of tumors with certain driver mutations, might induce release of neo-antigens by triggering target-directed tumor cell killing that generates a durable antitumor response and enhances sensitivity to checkpoint inhibition [13]. In particular, the drugs of interest are inhibitors that target the fibroblast growth factor receptor (FGFR) and vascular endothelial growth factor (VEGF) pathways, which are usually highly expressed in UC [3637]. Phase I trials that combine durvalumab with the FGFR inhibitor AZD4547 (NCT02546661) [38] and pembrolizumab with the anti-VEGFR2 monoclonal antibody ramucirumab (NCT02443324) [39] have been performed as a second-line and beyond therapy in platinum-refractory mUC. Table 2 summarizes the ongoing clinical trials combining immune checkpoint inhibition with other therapeutic modalities.
Another promising approach to enhance the effectiveness of treatment is the use of a dual checkpoint blockade, which involves the combination of PD-1/PD-L1 and CTLA-4 inhibitors. CheckMate-032, an open-label, multicenter, phase 1/2 studies that combine nivolumab and ipilimumab have provided the first indication of the clinical utility of this combination in the treatment of mUC (NCT01928394) [40]. Patients were received with either of two combination schedules, nivolumab 1 mg/kg+ipilimumab 3 mg/kg (N1I3) or nivolumab 3 mg/kg+ipilimumab 1 mg/kg (N3I1) every 3 weeks for four cycles, followed by nivolumab 3 mg/kg every 2 weeks, or nivolumab monotherapy 3 mg/kg (N3) every 2 weeks. ORR was 38.5%, 25.7%, and 25.6% in N1I3, N3I1 and N3 groups, respectively after a minimum follow-up of 3.9 months in N1I3 group (n=26), 13.0 months in the N3I1 group (n=104) and 14.5 months in N3 group (n=78). The frequency of drug-related grade 3–4 adverse events were similar in both combination groups (30.8% in N1I3 vs. 31.7% in N3I1), and higher than in the N3 group (23.1%). TRAEs caused discontinuation in 7.7% (N1I3), 12.5% (N3I1), and 3.9% (N3) of patients. One death was reported in the N3I1 group (pneumonitis) and two were reported in the N3 group (pneumonitis and thrombocytopenia) [40]. A randomized, open-label, multi-center phase III study (DANUBE NCT02516241) is currently underway to investigate the efficacy and safety of durvalumab, with or without tremelimumab, compared to that of standard-ofcare chemotherapy, as first-line treatment for patients with unresectable and/or mUC [41].
Lymphocyte activation gene 3 (LAG3) is an immune checkpoint molecule that is extremely expressed on the surface of activated ICs, including T cells, B cells, and NK cells. T cell immunoglobulin and mucin-3 (TIM-3) are other checkpoint proteins expressed on several ICs, such as T cells, NK cells, and monocytes. OX40, is a protein biding affiliated to the tumor necrosis factor receptor family, transduces a co-stimulatory signal during T-cell activation. Patients with mUC are being actively enrolled for several phase I trials that study TIM-3 antagonists (NCT02608268) [42], LAG3 inhibitors (NCT01968109) [43], and OX40 agonists (NCT02528357) [44], with and without PD-1/PD-L1 inhibitors. Currently, an anti-LAG3 mAb (BMS-986016) is being studied in conjunction with nivolumab in a phase 1 trial (NCT01968109) [43]. Similarly, an OX40 agonist (GSK3174998) is being investigated in conjunction with pembrolizumab in a phase I trial (NCT02528357) [44]. Another interesting approach for promoting the immune response further targets the T-cell microenvironment. Indoleamine 2,3-dioxygenase (IDO), which is an intracellular enzyme made by tumor cells, and plays an important role in the pathways that generate immune-suppressive metabolites [45]. Likewise, considering that high intracellular adenosine concentrations have a inhibitory effect on cytotoxic T-cell function, the adenosine A2A receptor (A2AR) is a potential target for cancer treatment [4647]. Currently, patients with mUC are being enrolled in several clinical trials (NCT02178722 [48], NCT02318277 [49], and NCT02655822 [50]) with regard to IDO or A2AR inhibitors, combined with PD-1 or L1 checkpoint inhibitors. The ongoing trials using dual checkpoint blockade are listed in Table 2.
IMMUNE CHECKPOINT INHIBITORS IN NON-METASTATIC MIBC OR NMIBC
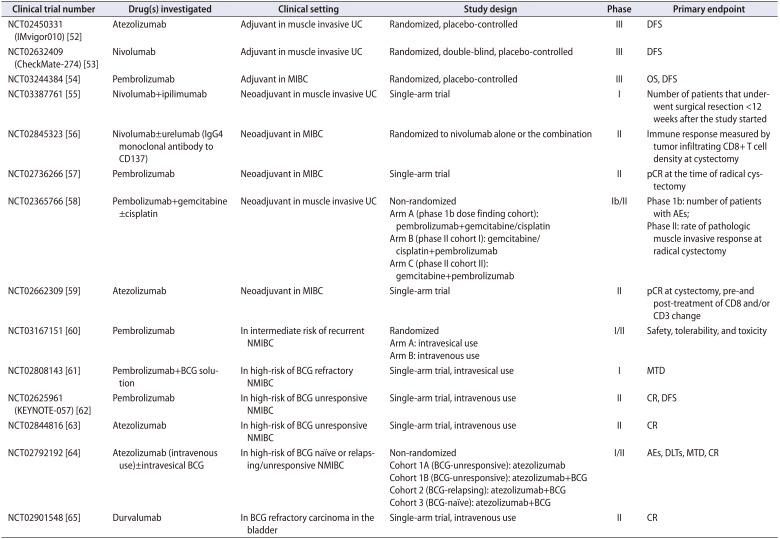
Although surgical therapies, including radical cystectomy and transurethral resection of bladder tumor (TURBT), are primarily applied as the primary standard therapeutic modalities for MIBC and NMIBC, adjuvant or neoadjuvant therapy using various anti-tumor drugs is frequently used to improve oncologic outcome. According to current guidelines, neoadjuvant chemotherapy using cisplatin-based combination regimen is recommended in patients with cT2-4aN0M0 MIBC, and the use of adjuvant cisplatin-based combination chemotherapy is selectively recommended for patients with locally advanced (pT3/4) and/or lymph node-positive disease [45]. In the case of NMIBC, the use of intravesical treatment with bacillus Calmette-Guerin or chemotherapeutic agents after TURBT has been recommended, based on risk group stratification for recurrence and progression [51]. Based on the accumulating evidence of immune checkpoint inhibitor in mUC, several immune checkpoint inhibitors are also being examined in MIBC and NMIBC settings. Three phase III trials are currently being implemented to identify the efficacy of atezolizumab (NCT02450331 or IMvigor010) [52], nivolumab (NCT02632409 or CheckMate-274) [53], and pembrolizumab (NCT03244384) [54] compared to that of placebo in the adjuvant setting of MIBC. Immune checkpoint inhibitors are currently being tested in a neoadjuvant setting as a phase I or II trial for nivolumab plus ipilimumab (NCT03387761) [55], nivolumab plus urelumab vs. nivolumab alone (NCT02845323) [56], pembrolizumab (NCT02736266) [57], pembrolizumab in conjunction with gemcitabine, with or without cisplatin (NCT02365766) [58], and atezolizumab (NCT02662309) [59]. In the case of NMIBC, several PD-1 and PL-L1 inhibitors are currently being tested for the use of adjuvants (intravenous or intravesical administration) in a phase I or II study design for pembrolizumab (NCT03167151 [60], NCT02808143 [61], NCT02625961 [62]), atezolizumab (NCT02844816 [63], NCT02792192 [64]), and durvalumab (NCT02901548) [65]. Patients are currently being enrolled in trials for MIBC and NMIBC, and the results are thus not yet available. The details of these trials are summarized in Table 3.
PREDICTIVE BIOMARKERS FOR IMMUNE CHECKPOINT INHIBITION IN UC
Although no commercialized biomarker is available, to predict the response to immune checkpoint inhibitors, several biomarker candidates including PD-L1 expression, tumor mutational (neo-antigen) burden, The Cancer Genome Atlas (TCGA) subtype, and interferon γ (IFN-γ) expression signature, are currently being explored in relation to UC; however, further validation is recommended.
1. PD-L1 expression
The expression of PD-L1 on tumor and/or ICs has been rigorously examined as a potential biomarker, but the data remain unconcluded; they range from a strong association with overall responses, using a composite biomarker required for patient selection in KEYNOTE-052 (pembrolizumab), IMvigor210 cohort 2 (atezolizumab), CheckMate-275 (nivolumab) [26], and durvalumab study [2766], to no association as identified in IMvigor210 cohort 1 (atezolizumab) [20] and KEYNOTE-045 (pembrolizumab) [25]. These disparities could be attributed to several factors, such as selection of PD-L1 expression either tumor cell or IC, diverse PD-L1 cut-off values, application of 4 different methods for PD-L1 IHC scoring, intra-tumoral heterogeneity of PD-L1 expression, mismatch of PD-L1 expression between primary tumor and metastases, and the possibility of continuous changes in PD-L1 expression due to the animated nature of the tumor microenvironment [6768]. Most importantly, up to 10% of patients with PD-L1-negative tumors are known to respond to anti-PD-L1 therapy, suggesting that the negative predictive role of PD-L1 as a biomarker is inadequate to rule out patients from potentially life-prolonging therapy.
2. Tumor mutational (neo-antigen) burden
The high mutational burden shows an obvious predictive implication for the response to the checkpoint inhibitor, since the adaptive cancer immunity is dependent on the recognition of neo-antigens encoded in tumor mutations [1314]. In a recently published trial on atezolizumab in UC, the median mutational load of responders was higher than that of non-responders (12.4 mut/Mb vs. 6.4 mut/Mb) [20]. However, whether mutational density alone can predict patient response still needs to be clarified. A wide variation is found regarding the upper range in non-responders of over 50 mut/Mb, with many responders having fewer than 10 mut/Mb; even tumors with relatively fewer neo-antigens, such as in renal cancer, respond to immunotherapy [1469].
3. TCGA subtype
The genomic analyses of UC have found several molecular clusters, including the luminal and basal subtypes or TCGA clusters I to IV [7071]. Integrated analytical results suggested that the TCGA UC subtype correlates with favorable response to PD-1/PD-L1-targeted immunotherapy [71]. Atezolizumab is likely to be the most effective drug in the luminal cluster II subtype in the IMvigor210 study, whereas nivolumab was the most efficacious drug in the basal type I in the CheckMate-275 study [2026]. The reasons for these discrepancies in the mUC subtype might be associated with tissue source. Both cohorts of IMvigor210 and CheckMate-275 allowed biopsy specimens from primary tumor, lymph nodes, or metastatic lesions for TCGA subtyping, which may have caused incorrect tumor classification. The criteria for molecular subtyping varied in each study, posing a challenge in standardizing TCGA classification. Nevertheless, the luminal I subtype, which is related to the upregulation of the FGFR pathway and high concentration of FGFR3 mutations and/or translocations, was insufficient of an immune signature, had low expression of PD-L1 in tumor cell, and suggested low responses to atezolizumab and nivolumab.
4. Immune gene expression profiling (IFN-γ expression signature)
Immune gene expression profiling can be a more useful biomarker for predicting the response to immune checkpoint inhibition than PD-L1 expression alone, since it can be quantified from multiple cell types within a cancer specimen, which is probably a better representative of the tumor microenvironment [7273]. In UC, the expression of IFN-γ inducible, CXCL9, CXCL10, and T-helper-1-type chemokines showed a close linkage with response to atezolizumab [20]. In the CheckMate-275 trial with nivolumab, a high expression of 25-gene IFN-γ signature was closely associated with almost 2.5-fold response to nivolumab than that without [26]. However, the negative predictive value of this gene panel remains a concern, since some responses were also identified in patients with a non-inflamed cytokine signature.
CONCLUSIONS
Immune checkpoint inhibitors have shown long-term durable response and tolerable safety profiles in several clinical trials. However, approximately 70% to 80% of patients may remain unresponsive to immune checkpoint inhibition. Therefore, further research on combining immune checkpoint inhibitor therapy with other therapeutic modalities, such as cytotoxic chemotherapy or different therapeutic targets, is needed to reinforce the effects of immunotherapies. Additional clinical trials with longer clinical follow-up for the PD-1/PD-L1 inhibitors are required to define their role in treating locally advanced and mUC in the first-line setting, and to define their potential for neoadjuvant and/or adjuvant therapy. Finally, the unavailability of specific biomarkers for predicting treatment responses remains a major limitation on the use of immune checkpoint inhibitors in real clinical practice. The existence of predictive biomarkers will enable selective use of immune checkpoint inhibition in the expected responders. Therefore, identification of these biomarkers should be consistently investigated and validated through additional supportive basic and clinical research.
 XML Download
XML Download