

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lower urinary tract symptoms (LUTS) and erectile dysfunction (ED) are both significant age-associated health problems in men. Further, recent epidemiologic studies strongly suggested that there was a close association between LUTS and ED [1]. This association proposes new possible approaches to evaluate both conditions and identify new targets for treatment. Studies have recommended that men presenting with LUTS should be evaluated for ED and those presenting with ED should be assessed for LUTS [234]. However, the causal relationship or pathophysiological pathway between LUTS and ED has not been clearly established, although possible pathophysiological mechanisms have been suggested [1].
Postmicturition dribble (PMD) is considered one of the most bothersome and frequent LUTS [56]. PMD, defined as an involuntary loss of urine immediately after passing urine, is classified as a postmicturition symptom according to the standardization subcommittee of the International Continence Society (ICS) [7]. Although the exact pathophysiological mechanisms of PMD are not yet known, several studies have suggested that PMD might occur secondary to a small volume of residual urine in either the bulbar or prostatic urethra that is normally ‘milked back’ into the bladder at the end of micturition [89].
However, most studies on LUTS have focused only on voiding and storage symptoms, not on postmicturition symptoms. In addition, only a few studies on PMD have focused on its prevalence. Furthermore, recent experimental studies showed that changes in the anatomical structure of the corpus cavernosum with aging might be related to the volume of urine in the bulbous urethra after voiding [101112]. These findings suggest that PMD might be correlated with ED and might reinforce the relationship between LUTS and ED. Nevertheless, to our knowledge, only two studies have assessed the correlation between PMD and ED [1314]. Furthermore, both previous studies only considered whether PMD was present. In the present study, for the first time, the correlation between PMD and ED was assessed by performing a quantitative analysis of middle-aged and older men with LUTS.
MATERIALS AND METHODS
1. Study design and ethics statement
Our prospective, cross-sectional, observational, multicenter study was performed at Kangdong Sacred Heart Hospital, Dongtan Hospital, and Chuncheon Sacred Heart Hospital in Korea between April 2017 and December 2017. The study protocol was approved by the Institutional Review Board of Hallym University Chuncheon Sacred Heart Hospital (Reg. No. 2017-7), and the study was performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki, 1964, and Declaration of Tokyo, 1975, as revised in 1983). Men with LUTS (International Prostate Symptom Score [IPSS] ≥8) over 40 years old were enrolled. Men with neurological disorders, urinary tract infections, renal insufficiency, bladder stones, prostate cancer, urethral strictures, congenital or acquired penile malformation, or previous pelvic surgery, or those who took medications that were related to LUTS or ED within 4 weeks were excluded from the study. Finally, 205 men were included. After the study design was explained to the subjects, written informed consent was obtained.
2. Variables
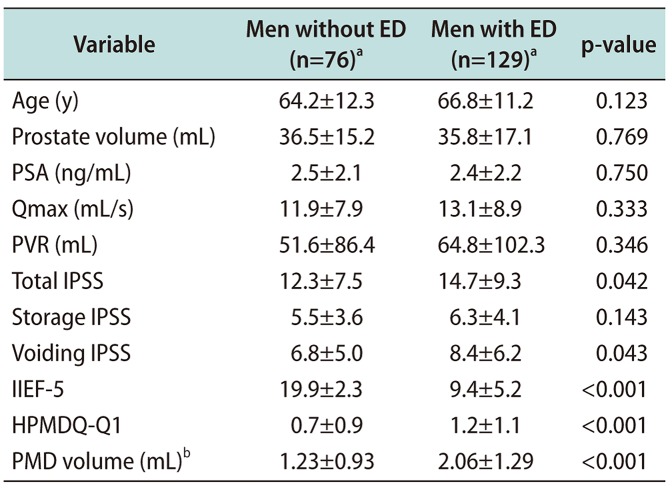
Recorded parameters were age, prostate volume, serum prostate-specific antigen (PSA), maximum urinary flow rate (Qmax), postvoid residual urine (PVR), IPSS, International Index of Erectile Function-5 (IIEF-5) score, Question 1 of the Hallym PostMicturition Dribble Questionnaire (HPMDQ-Q1) score, and volume of PMD (Table 1).
The severity of LUTS was assessed using the IPSS, and a total IPSS ≥8 points was considered to indicate the presence of LUTS [15]. The severity of ED was assessed using the IIEF-5 score, and an IIEF-5 score ≤17 was considered to indicate the presence of ED [16].
PMD was assessed using the HPMDQ-Q1 (“Over the last month, how often have you experienced dribbling after voiding when you feel you have finished urination?” 0: not at all, 1: 1 out of 3 times, 2: 2 out of 3 times, 3: almost always or always). The HPMDQ is a self-administered questionnaire developed for this study to evaluate PMD and is composed of four items with answers on a scale from 0 to 3 (Appendix). The questionnaire includes questions concerning frequency (Question 1), severity (Question 1-1), bother (Question 2), quality of life (Question 3), and response to treatment (Question 4). Only HPMDQ-Q1, which indicates the frequency of PMD, was used to compare the value of PMD for ED with that of IPSS which indicates the frequency of LUTS. The volume of PMD was calculated with a paper test that was newly developed by the authors of this study. The purpose of the paper test was to directly measure the PMD volume by attaching a paper pad inside the patient's undergarment. The amount of wetting of the paper is compared before and after urination. The prostate volume was measured using transrectal ultrasound, and the Qmax and PVR were assessed using an uroflowmeter and bladder scanning, respectively.
3. Main outcome measures
The primary endpoint was a Pearson's correlation coefficient (r) of 0.3 or greater or less than −0.3 in the correlation between the HPMDQ-Q1 and IIEF-5 scores. The second endpoint was the degree of the correlation between the PMD volume and IIEF-5 score. In addition, the r of the HPMDQ-Q1 for IIEF-5 was compared with the r of each IPSS measure, to further evaluate the value of PMD. We also analyzed whether incorporating the HPMDQ-Q1 score into the IPSS improves the predictive accuracy of LUTS in those with ED, to specifically simulate the need for PMD.
4. Statistical analyses
Our study was designed with 95% power and 1% level of significance to detect an r of 0.3 or greater or less than −0.3 in the correlation between the HPMDQ-Q1 and IIEF-5 scores, based on a previous pilot study (data not published). Based on the pilot study, an r of −0.244 was calculated, which was subsequently rounded to a clinically relevant cut-off of −0.3 because an r of ±0.3 was generally considered a reference for a moderate correlation. A minimum of 189 subjects was required for the statistical analysis.
To compare the distributions of parameters according to the presence of ED, Student's t-test and chi-square test were used to compare continuous and categorical variables, respectively. Analyses of the volume of PMD were conducted using the geometric mean with logarithmic transformation because its distributions were positively skewed. Correlations between continuous variables were assessed using r via a bivariate correlation analysis. A Z-test using Fisher's transformation was performed to compare r values between variables. Nomograms of IPSS not incorporating and incorporating HPMDQ-Q1 were generated using multivariate regression coefficients. And then, receiver operating characteristic curve-derived areas under the curve were estimated and compared using DeLong et al's test.
The Statistical Package for Social Sciences, Window ver. 21.0 (IBM Co., Armonk, NY, USA) and MedCalc for Windows, version 11.0.0.0 (MedCalc Software, Mariakerke, Belgium) were used for the statistical analyses. All p-values were two-sided, and a p-value <0.05 was considered statistically significant.
RESULTS
1. Clinical characteristics in relation to erectile dysfunction
Table 1 shows the clinical characteristics of the patients in relation to ED. Of the 205 men with LUTS, 129 (62.9%) had ED. There were no significant differences in age (p=0.123), prostate volume (p=0.769), PSA (p=0.750), Qmax (p=0.333), PVR (p=0.346), or storage domain of the IPSS (p=0.143) between men with ED and those without. However, the mean total and voiding IPSSs were higher in men with ED than in those without (p=0.042 and 0.043, respectively). Regarding PMD, the mean HPMDQ-Q1 score was higher and the volume of PMD was larger in men with ED than in those without (p<0.001 for each).
2. The association between postmicturition and erectile dysfunction
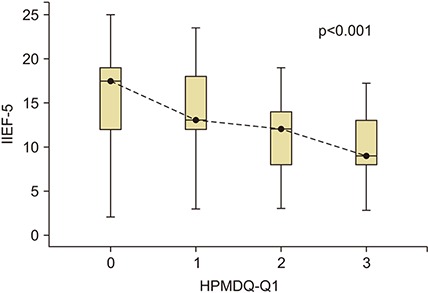
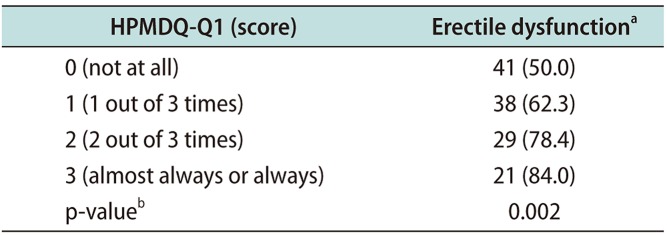
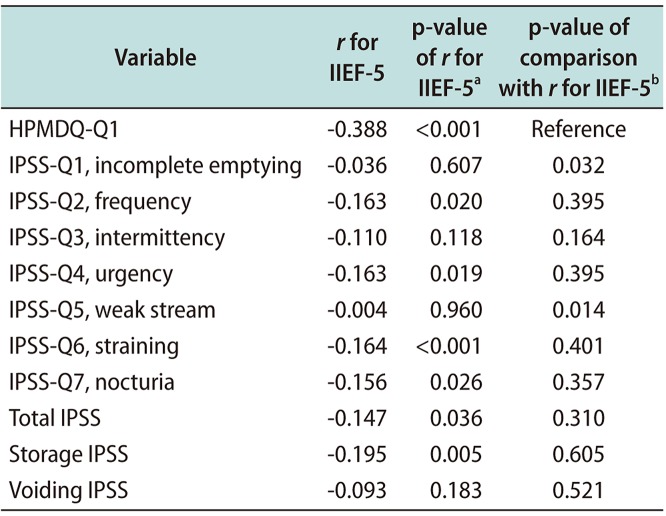
The HPMDQ-Q1 score was inversely well correlated with the IIEF-5 score (r=−0.388, p<0.001; Fig. 1). Moreover, the volume of PMD was inversely correlated with the IIEF-5 score (r=−0.138, p=0.042). The prevalence of ED increased as the HPMDQ-Q1 score increased (Table 2). The prevalence of ED was 50.0% when the HPMDQ-Q1 score was 0, but the prevalence was 84.0% when the HPMDQ-Q1 score was 3 (p=0.002). When compared with IPSS measures one-on-one, r of HPMDQ-Q1 for IIEF-5 was not at least lower than that of all IPSS measures, but rather higher than of some IPSS measures including IPSS for incomplete emptying and weak stream (p=0.032 and 0.014, respectively; Table 3). The predictive accuracies of the IPSS nomogram that did and did not incorporate the HPMDQ-Q1 for ED were 68.5% (95% confidence interval=0.617–0.748) and 64.3% (95% confidence interval=0.573–0.708), respectively. Incorporating the HPMDQ-Q1 into the IPSS tended to slightly increase the accuracy of predicting LUTS in those with ED (p=0.082).
DISCUSSION
Our prospective, cross-sectional, observational, multicenter study demonstrated that PMD was well correlated with ED and that considering PMD reinforced the relationship between LUTS and ED. To our knowledge, this was the first study to assess the correlation between PMD and ED with a quantitative analysis and suggest that postmicturition LUTS, such as a PMD, might be an important component of the association between LUTS and ED.
Regarding the patients' clinical characteristics according to the presence of ED, there were no significant differences in age, prostate volume, PSA, Qmax, and PVR, except for LUTS, between men with ED and those without. It is well known that age does not affect the association between LUTS and ED [1].
Recent epidemiologic studies strongly suggested that there was a close association between ED and the total IPSS which represents LUTS [1]. However, the association between ED and the storage or voiding domains of the IPSS is controversial [17]. A community-based study of 2,084 men found that the severity of ED was associated with the total IPSS, specifically in the urgency and nocturia domains [18]. In contrast, another community-based study of 2,858 men found that the presence of ED was associated with the total IPSS, specifically the scores for the voiding, nocturia, and quality of life domains [19]. A practice-based study of 333 men showed that the prevalence of sexual dysfunction was significantly higher in patients with either storage or voiding LUTS than in men without LUTS [20]. This trend also appeared in our study. The mean total IPSS in men with ED was higher than that in men without ED. Furthermore, the severity of ED was correlated with the total IPSS. However, it was difficult to come to a firm conclusion about the association between ED and the storage and voiding IPSS domains. In men with ED, the mean IPSS for the voiding domain, not that for storage, was higher than that in men without ED. Conversely, the severity of ED was correlated with the storage IPSS domain, not the voiding IPSS domain.
LUTS are defined as non-specific voiding-associated symptoms that may occur secondary to various disorders. According to the classification system of ICS, LUTS are generally divided into three types: storage, voiding, and postmicturition symptoms [7]. Among these symptoms, postmicturition symptoms, which include PMD and the feeling of incomplete voiding, are experienced immediately after micturition. Nearly all studies on LUTS have focused only on both storage and voiding symptoms. Researchers' indifference to postmicturition symptoms may be due to the belief that postmicturition symptoms might have a lower prevalence and elicit less discomfort than storage and voiding symptoms do [12122]. However, recent studies demonstrated that the prevalence of postmicturition symptoms might be higher than that previously expected, and some studies reported that the prevalence was over 50% [523]. It might be necessary to consider postmicturition symptoms in patients with LUTS.
In a population-based study that involved more than 3,000 men aged 50 to 70 years, the prevalence of PMD was 63% [24]. Another study involving more than 7,000 men aged 30 to 80 years showed that the prevalence of PMD was 58.1% [5]. Another internet-based study involving 30,000 people from the general population reported an overall PMD prevalence of 46% [23]. PMD is considered as one of the most bothersome LUTSs as well as of the most common LUTSs [625]. In a population-based study involving 1,709 men, PMD was one of the most prevalent symptoms that caused moderate or severe bother among men [6]. Another study involving 7,470 men reported that men aged 30 to 40 years were bothered the most by PMD [25]. In addition, from a practical point of view, PMD is not included in the IPSS, which is the most widely used tool to evaluate LUTS worldwide. These evidences suggest that considering PMD might affect the association between LUTS and ED.
To our knowledge, only two studies have specifically assessed the correlation between PMD and ED [1314]. In a population-based study in France, Macfarlane et al [13] analyzed 2,011 men between 50 and 80 years old regarding their satisfaction with their sexual lives. Data were obtained with a self-administered questionnaire or an interview. They showed that PMD was closely associated with sexual life dissatisfaction. However, it is noted that sexual life satisfaction could not directly reflect erectile function. Frankel et al [14] analyzed 1,271 men over the age of 45 years with LUTS in 12 countries. Data on the rigidity of erection and PMD were obtained with a self-administered questionnaire. They showed that PMD was closely associated with the reduced rigidity of erection. However, it is noted that PMD and rigidity of erection were considered as simple variable that is only divided into two groups in their study.
The results of the previous two studies were generally similar to those of our study. However, our study has several strengths that allow us to better understand the correlation between PMD and ED. First, to determine the correlation between PMD and ED, the degree of severity was analyzed as well as prevalence. Second, objective measures of PMD such as the PMD volume were used for the analysis, in addition to subjective measures such as the questionnaires. Finally, the relative importance of PMD was analyzed with a one-on-one comparison between PMD and other LUTS.
The mechanism by which PMD might be correlated with ED remains unknown. One hypothesis is that the changes in the anatomical structure of the corpus cavernosum occur with aging. Owing to the urethrocorporocavernosal reflex, relaxation of the sinusoidal muscle and contraction of the cavernosus muscles during micturition might produce a mild degree of penile tumescence and stretch that might assist urinary flow during micturition [10]. With aging, fibrosis of the corpus cavernosum causes a modification of cavernosal angioarchitecture including a decrease in the smooth muscle components and an enlargement of the vascular lumens, which limit the basic function of penile vasculature, leading to weakened urethro-corporocavernosal reflex as well as ED [1112]. This weakened urethro-corporocavernosal reflex could cause disturbances in urinary flow in a bulbous urethra during micturition, leading to PMD.
The most widely used tool for evaluating LUTS is IPSS. However, PMD cannot be assessed using the IPSS, as there are no questions concerning PMD. Therefore, most studies have used the Danish Prostatic Symptom Score (DAN-PSS-1) questionnaire to assess PMD [2627]. However, the DAN-PSS-1 questionnaire does not include information on the frequency of PMD and related quality of life, although the severity of symptoms and associated bother may be assessed. Therefore, we used the HPMDQ to assess PMD. The HPMDQ was designed by authors, to allow for the assessment of various aspects of PMD, including frequency, severity, bother, quality of life and response to treatment.
There were a few limitations to our study. First, the HPMDQ has not been validated for the evaluation of PMD, although it is a modified form of validated questionnaires including the IPSS, DAN-PSS-1, and Clinical Global Impression scale. Second, comorbidities such as metabolic syndrome, which might affect the association between PMD and LUTS, were not considered in our study [1]. Evaluating these comorbidities might provide a better understanding of the impact of PMD on LUTS. Third, the patients in our cohort did not represent the whole population because only middle-aged and older men with LUTS were included. Finally, because all the men who were included in this study were Korean, the association between PMD and ED might differ when it is assessed in other countries and in people of other ethnicities [28]. However, recent studies suggested that Asian men including Korean men tend to be similar to Western men, in the association between LUTS and ED [29].
CONCLUSIONS
PMD was significantly correlated with ED in middle-aged or older men with LUTS. Also, the significance of PMD on ED was not at least lower than that of other LUTSs, and PMD reinforced the relationship between LUTS and ED. Our results suggest that PMD might be an important component to assess the association between LUTS and ED, and suggest the possibility of PMD improvement by managing ED. Further studies including larger cohorts are needed.
 XML Download
XML Download