

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Aging is a global health issue. The World Health Organization predicted that the population of people over 60 years of age will reach approximately two billion by 2050. Aging is defined as a decline in functionality at the cellular, tissue, and organ levels and is related to metabolic, physiological, and functional impairments. In clinical medicine, one of the primary aging-related changes is increased body weight and waist circumference. In the elderly, low levels of physical activity can lead to an increase in body weight and body fat. Even without any weight change, body composition can change with aging [1]. Skeletal muscle mass decreases, whereas body fat, including total body, intra-abdominal, and intermuscular fat, increases [1]. This may be related to functional loss of physical activity and disability [2]. Sarcopenia is a syndrome characterized by progressive and generalized loss of skeletal muscle mass and strength, primarily associated with aging [3]. However, many conditions other than aging, such as acute and chronic diseases, immobilization, malnutrition status, and deficiency of anabolic hormones (e.g., growth hormones and sex hormones) may be involved in the etiology of sarcopenia. The correlations and causal relationships between sex hormones and muscle mass and function have not yet been fully elucidated, but both are known to decrease with age [4]. Although the results are inconsistent, epidemiological studies have found that lower testosterone levels are related to decreased muscle mass or function [567].
Here, we review the etiology of and diagnostic criteria for sarcopenia. Additionally, the relationship between sarcopenia and testosterone and the impact of testosterone treatment on muscle mass and function are also discussed.
SARCOPENIA
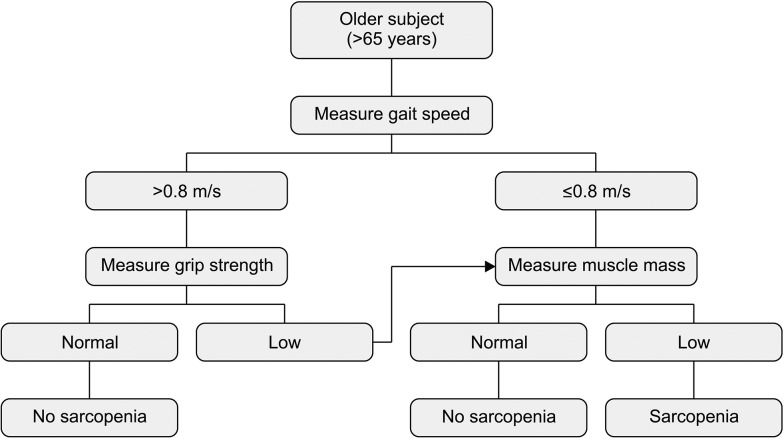
Sarcopenia, from the Greek terms sarx for flesh and penia for loss, was originated by Rosenberg in 1989 to describe the age-related loss of muscle mass [3]. The aging process is connected to changes in body composition involving decreased muscle mass and increased body fat, with or without body weight change [1]. Muscle mass peaks in the third decade of life and decreases by approximately 1% to 2% per year [89] owing to changes in muscle fiber type and size [1011]. Muscle strength decreases by approximately 1.5% to 3.0% per year, and the rate of decline is steeper after age 50 [812]. Loss of muscle mass and function is correlated with high morbidity and mortality owing to an increased risk of frailty and falling. As these medical conditions increase social and healthcare costs, both the perceived importance of muscle mass and function and overall interest in the topic have been increasing. However, until recently, there were no clear diagnostic criteria for sarcopenia, and the detection methods and results differed according to study design. In 2010, the European Working Group on Sarcopenia in Older People (EWGSOP) proposed a practical clinical definition and consensus diagnostic criteria for age-related sarcopenia as a generalized loss of skeletal muscle mass and strength according to risk factors such as physical disability, poor quality of life, and death [13]. They suggested that sarcopenia should be diagnosed using the criteria of low muscle mass and reduced muscle function (decreased strength and/or poor physical performance) [13]; they summarized the methods for detecting muscle mass and function. They recommended estimating muscle function based on gait speed and grip strength and muscle mass according to appendicular skeletal muscle mass adjusted by height squared (Fig. 1).
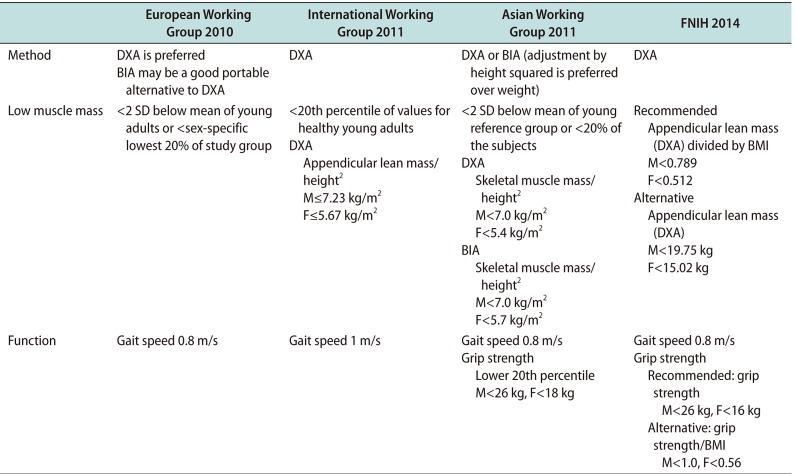
Thereafter, the International Working Group on Sarcopenia (IWGS) [14], Asian Working Group for Sarcopenia (AWGS) [15], and Foundation for the National Institutes of Health (FNIH) Sarcopenia Project suggested a consensus diagnosis based on social conditions (Table 1) [16]. In general, the target population consisted of individuals aged 65 years and older, but the cutoff values varied by ethnic group or population. As a result, the specific prevalence of sarcopenia differs according to the diagnostic criteria. The large population studies have reported that sarcopenia affects over 20% of 60- to 70-year-old, and approaches 50% in those over 75 years [17]. The symptoms reported in these studies are not specific. Usually reported as a general weakness, sarcopenia can be recognized in cases of decreased muscle function, such as reduced lower leg power or functional mobility measured by short physical performance battery [17]. These symptoms can cause falls, which are related to the patient's morbidity and mortality. As a result of previous studies, and its important impact on social health, sarcopenia was admitted as a disease entity with the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) (M62.84) code in 2016. Currently, treatment of sarcopenia is a growing challenge, with many modalities being suggested and studied. Some of these include resistance exercise, consumption of protein with essential amino acids, as well as treatment with selective androgen receptor modulators, growth hormone, ghrelin agonists, myostatin antibodies and activin II receptor antagonist and testosterone [18].
TESTOSTERONE
Sarcopenia has numerous causes, including anorexia, inflammation, hypovitaminosis, immobilization, and hypogonadism. Testosterone, one of the representative sex hormones, is produced by Leydig cells in the testes in response to luteinizing hormone. A longitudinal study showed that testosterone levels decreased at a rate of approximately 1% per year after the age of 30 [19]; thus, approximately 40% to 70% of men older than 70 are likely to have low testosterone levels [20]. That is, along with androgen deprivation, age-related decreases in sex hormone levels can be defined as a hypogonadal state [21]. A study reported men with obesity, metabolic syndrome, and type 2 diabetes have low testosterone levels, especially when visceral adiposity is high [22]. However, in a cross-sectional study, testosterone exhibited a stepwise decrease with age with or without obesity [23], even after adjustment for other factors, such as body mass index and subscapular skinfold measurements [24]. Whether decreased serum testosterone levels explain aging-related loss of muscle mass or function has not yet been established; however, there have been several studies on the relationship between testosterone and muscle mass and function. One study reported that muscle mass was significantly associated with serum-free testosterone and insulin-like growth factor 1 (IGF-1) in relatively healthy, well-nourished elderly men [25]. Another study showed that decreases in basal blood testosterone levels in aging people may be associated with age-related declines in maximal voluntary neuromuscular performance capacity [26]. Age, arm, and leg regional fat-free mass, serum testosterone, and the free testosterone index are significantly associated with arm and leg strength in generally healthy men [25].
1. The mechanism of the effects of testosterone on muscle
The exact mechanism of how androgen affects muscle has not yet been elucidated, however, a number of suggestions have been put forward. In human studies, testosterone treatment increased type I muscle fibers in both low and high concentrations, and type II muscle fibers in high concentrations [2728]. An increase in muscle fiber size is enhanced by increased protein synthesis, due to the high rate of re-utilization of intracellular amino acid by testosterone [29]. Testosterone is also reported to stimulate the mitotic activity of satellite cells in myoblast culture systems [30], which is a major source for the addition of new myonuclei into the hypertrophying muscle fibre [31]. Some studies have suggested non-genomic testosterone actions on the activation of a G-protein-linked receptor with increased intracellular Ca2+ concentration of myoblasts, which resulted in cellular growth [32], while others reported that androgens affect muscular hypertrophy by increasing IGF-1 expression [33], dependent upon Erk and mammalian target of rapamycin signaling [34].
2. The effects of testosterone on muscle
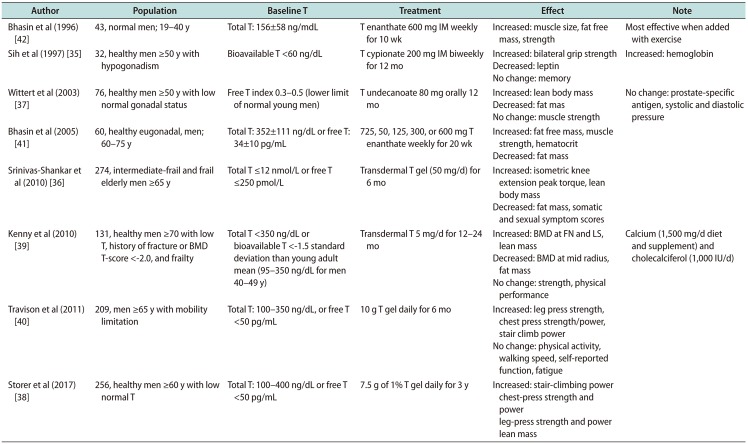
Several randomized controlled trials (RCTs) showed the efficacy of testosterone on muscle, but the results varied by subject, dosage, and treatment methodology. These data are summarized in Table 2 [3536373839404142]. In the hypogonadal men, results were consistent regarding the effect of testosterone on muscle mass and fat mass [353637]. In the past, testosterone was given as an injection [35]. In one study, 15 hypogonadal men (mean age 68 years old, bioavailable testosterone <60 ng/dL) were randomly assigned to receive a placebo or 200 mg testosterone cypionate biweekly for 12 months. Although testosterone supplementation improved grip strength, side effects such as increased hemoglobin levels were reported. Additionally, the difficulty of administration via injection was pointed out. One of the largest studies with non-injectable testosterone was the Testosterone's Effects on Atherosclerosis Progression in Aging Men (TEAAM) trial reported in 2017 [38]. Healthy men over 60 years of age with low normal testosterone levels (total testosterone 100–400 ng/dL or free testosterone <50 pg/mL) were randomly assigned to daily treatment with 7.5 g 1% testosterone or placebo gel for 3 years. Testosterone replacement for 3 years was associated with modest improvements in chest press strength, muscle power, unloaded and loaded stair-climbing power, and lean body mass, but not leg press strength. Likewise, the results regarding the effect of testosterone on muscle function were inconsistent. Some reported that muscle power was increased [38], while others reported that there was no difference in muscle strength [3739], physical performance, activity or walking speed. These results are in line with the meta-analysis of 11 RCTs that evaluated the efficacy of androgen treatment (testosterone/5α-dihydrotestosterone) [43]. These data showed moderate efficacy in muscle strength, not only for the hypogonadal men but also in eugonadal older men or healthy young normal men who underwent supplementation of testosterone in various concentrations [41]. Both increased muscle size and decreased fat mass were seen, especially in those treated with both a supraphysiologic concentration of testosterone and exercise [42]. Additionally, it was effective in both muscle and bone when treated with calcium and vitamin D [39]. One study (not an RCT) involving muscle biopsy showed that muscle accumulation was associated with an increased fractional synthesis rate of mixed skeletal muscle proteins and that a trend existed toward a similar increase in the fractional synthesis rate of myosin heavy chain after treatment with testosterone [44]. Direct comparison is not possible between the studies, but the studies themselves indicate an important role for testosterone in developing and maintaining muscle mass and function.
CONCLUSIONS
Testosterone is widely used to improve impotence or increase libido but not for muscle mass or function. Its efficacy for increasing muscle mass or function varies by subject and method. In terms of the treatment of sarcopenia, sex hormones are probably not the only answer. However, it is evident that testosterone holds potential for treating sarcopenia, although the side effects, such as increased hematocrit levels and risk for cardiovascular disease, are concerning. Sarcopenia is the result of a multifactorial process, and the precise contribution of sex hormones is not evident. However, if current interest levels and research efforts continue, the role of testosterone in sarcopenia may be clarified in the near future.
 XML Download
XML Download