

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dehydroepiandrosterone (DHEA) is a steroid prohormone. By the age of 70 to 80 years, levels may be as low as 10% to 20% of those encountered in young individuals [12]. The mechanism underlying this physiological decline is unknown. However, this age-related decline in DHEA levels may correlate with many age-related phenomena or deterioration in various physiological functions. Particularly, aging; neurological functions including decreased well-being, cognition, and memory; increased depression; aggressiveness; and dementia have involved changes in body composition, decreased bone mineral density, obesity, diabetes, increased cardiovascular morbidity, erectile dysfunction (ED), and decreased libido [34]. Supporting this result, some trials of DHEA supplementation in healthy, middle-aged, and elderly subjects have reported improvements in different aspects of well-being [5].
Consistently, in our previous study we have demonstrated age-related decline in testosterone level throughout 4 years of follow-up in patients with ED. Patients with decreasing testosterone levels were older than patients with a steady testosterone level [6]. Therefore, this steady decrease in circulating DHEA concentrations with age might initiate the speculation that DHEA therapy have potential benefits in several diseases associated with aging.
Recent analyses for the association between age and ED revealed positive effects for testosterone, DHEA, perceived general health, emotional support, intimacy motivation, and a negative effect for interleukin-6 (IL-6) (all p<0.05). Higher testosterone and DHEA and lower IL-6 levels buffered against an age-related increase in ED [7]. Furthermore, an interesting study demonstrated that men who work nonstandard shifts and have poor sleep quality are at increased risk for hypogonadal symptoms and sexual dysfunction however, no associations between sleep quality and mean serum testosterone, free testosterone, estrogen, DHEA, follicle stimulating hormone, and luteinizing hormome levels were observed [8].
Go to : 
BIOCHEMISTRY OF DEHYDROEPIANDROSTERONE
DHEA is a steroid prohormone synthesized in the zona reticularis of the adrenal cortex, the gonads, adipose tissue, brain, and skin. In target tissue, DHEA transformed through intracrine mechanisms to androgens or estrogens. The secretion of DHEA follows a diurnal pattern like that of cortisol. While in women adrenal production of DHEA and DHEA sulfate (DHEAS) contributes substantially to overall androgen production, in men the adrenal contribution is very small [12]. Together DHEA and DHEAS are the most abundant steroid in humans. The highest concentrations of these steroids are observed in men in the second and third decades of age, and gradually decrease by approximately 10% per decade [1].
DHEAS exists at approximately 250 times higher than those of free DHEA in serum. In target tissues such as the brain, bone, breast, and adipose, DHEAS is converted to DHEA by the sulfatase enzyme, which may then be further metabolized to androstenediol, androstenedione, estrone, testosterone, dihydrotestosterone, and 17β-estradiol [91011]. Meanwhile DHEA is a prohormone, it is claimed to have several positive effects on age-related disorders. It would be theoretically transformed according to local and general hormone needs.
Go to :
EFFECT OF DEHYDROEPIANDROSTERONE ON ENDOTHELIAL AND SMOOTH MUSCLES FUNCTION
DHEA is involved in vascular smooth muscle relaxation. Furthermore, the general and sexual effects are not due to the actions of DHEA alone but due to its function as a precursor of multiple androgens, especially testosterone and estradiol as well [910].
Endothelial dysfunction contributes to the pathogenesis of atherosclerosis and cardiovascular disease and leads to the development of insulin resistance. Since DHEA has its own receptors, primarily on endothelial cells its administration has been shown to improve flow-mediated dilation of the brachial artery, an endothelium-dependent process; reduced plasminogen activator inhibitor type 1, a suppressor of fibrinolysis with a pathogenic role in coronary artery disease; and improved insulin sensitivity [12]. The improvement of endothelial function with DHEA was subsequently confirmed in postmenopausal women [13]. Several in vitro experiments have confirmed the anti-atherosclerotic actions of DHEA [1314].
These data support the action of DHEA on the endothelium, based on the rapidity of action on endothelial nitric oxide synthase (eNOS) and failure to block endothelial cell activation with selective estrogen or testosterone receptor antagonists [1314]. The roles of DHEA in vascular endothelial cell survival [1516], proliferation/ angiogenesis, and activation, including transcriptional regulation of endothelin-1 were demonstrated [17]. Although a convincing evidence from in vitro studies for vasculoprotective effects of DHEA, human clinical trials of DHEA replacement on metabolic and vascular function have shown contradictory results. Epidemiological data in men have demonstrated either an inverse or no relationship between cardiovascular mortality and circulating DHEAS levels [1819].
A specific DHEA receptor was identified on bovine aortic endothelial cells [20]. This receptor is primarily coupled to Ga12 and Ga13 subtypes of the G protein family which activates eNOS. Further study had demonstrated the existence of a DHEA-specific receptor in human vascular smooth muscle cells (VSMC) involving ERK1 signaling pathways that contributes to remodeling of blood vessels and initiation of atherosclerosis [21]. In vitro study DHEA also inhibits VSMC proliferation through a mechanism independent of its transformation into estrogens or androgens and shows minimal affinity for estrogen and androgen receptors found in VSMC cells, but binds specifically to putative receptors in the same cells. Although consistent with the mechanism of action through conversion into testosterone and estradiol, these findings will enlighten our interpretations of the biological actions of DHEA and the control of sexual function, which involves many vascular mechanisms.
Go to :
DEHYDROEPIANDROSTERONE AND NITRIC OXIDE PATHWAY
DHEA is shown to activate potassium channels via soluble guanylate cyclase activation and enhance endothelial function through increased nitric oxide (NO) synthesis and ultimately dilate arteries, block hypoxia-induced vasoconstriction [1422]. Through a plasma membrane initiated mechanism, DHEA acutely increase NO release from intact vascular endothelial cells [23]. The decrease in cytosolic NOS enzyme activity and penile NOS is not affected by adrenalectomy in castrated rats [24]. Adrenalectomy combined with castration significantly reduced penile neuronatal NOS (nNOS) content, in contrast to what was found with castration or total ablation of androgen binding in the penis [25], where NOS activity appeared to be inhibited in the presence of constant NOS levels. The cause of this reduction in penile nNOS content is unknown. It may be related to a loss of nerve terminals or a true NOS downregulation [26]. However, penile eNOS content remains unaffected after 1 week. The rat adrenal gland contributes to the maintenance of the erectile mechanism and may affect nNOS content in the rat penis [27].
In pulmonary artery tissue from DHEA-treated rats, soluble guanylate cyclase, but not eNOS, levels were increased [28]. However, in other experiments, DHEA/DHEAS did not affect relaxation induced by acetylcholine or sodium nitroprusside, and relaxation responses were not changed by treatment with methylene blue [29]. Nevertheless, in vitro studies supporting proper intrinsic functions have shown that DHEA may directly increase NO production from intact endothelial cells, probably through G protein-dependent activation of endothelial NO synthetase [23].
Go to :
DEHYDROEPIANDROSTERONE AND ERECTILE DYSFUNCTION
DHEA plays an important role in sexual function. Low levels of DHEA were associated with a higher risk for ED in men [3031] and low sexual responsiveness in women [32]. It has also been speculated that DHEA plays a role in the process of erection. The Massachusetts Male Aging Study investigated 17 hormones, and DHEAS was the only one inversely correlated to ED prevalence [31]. This data was later confirmed by another study, which demonstrated that DHEAS levels were significantly lower in men with ED in comparison to age-matched normal controls [33]. The same group had demonstrated that DHEA treatment was associated with higher mean scores for each of the five domains of International Index of Erectile Function (IIEF) score [34].
In a more recent study, 79 men with sexual dysfunction and androgen deficiency had received oral testosterone undecanoate (80 mg twice daily), DHEA (50 mg twice daily), or placebo. There were no significant differences in sexual performance outcomes between placebo or intervention, as assessed by IIEF, the Androgen Deficiency in the Aging Male, Aging Male Symptom Scale, and Global Assessment Questionnaire [35].
Lacking evidence-based data to show involvement of DHEA in ED is obvious, however promising data supporting the possibility of DHEA-specific receptors availability on vascular endothelial and smooth muscle cells allows the postulation of its possible involvement in the vascular mechanisms of erection [21]. DHEA is only a weak androgen by itself that does not have any restorative effect on the erectile response in adrenalectomized or castrated animals [3637]. Furthermore, DHEA is involved in conditions associated with aging, immune suppression, and major diseases. In addition, DHEA enhances the feeling of well-being, but not libido in older men [3637]. The positive effect of DHEA on erection supports the notion that adrenal corticoids are involved in this process. Clinical studies showed that oral DHEA treatment increased total serum testosterone levels, libido, sexual activity, and sexual satisfaction in postmenopausal women [38]. More recent study reported that higher endogenous levels of testosterone and DHEA are beneficially related to sexual health in men and seem to ameliorate the age-related ED [39].
Furthermore, testosterone and DHEA might exert their positive effects on erectile function via their vasodilative and molecular properties. Additionally, lower levels of IL-6 were associated with age-related increase of ED, which further confirms the hypothesis of an association between inflammation and ED. The levels of several proinflammatory cytokines are also elevated in cardiac dysfunction, and the administration of phosphodiesterase type 5 inhibitor such as sildenafil was reported to cause a sustained reduction of proinflammatory cytokines, linking the influence of proinflammatory cytokines on vasculogenic function and ED [40].
Go to :
DEHYDROEPIANDROSTERONE AS A TREATMENT FOR ERECTILE DYSFUNCTION
Several studies have reported decreased serum DHEAS levels in patients with ED and denoted that decreased secretions of DHEA and DHEAS are important risk factors for ED in aging men [41]. DHEA levels reach their peak in the third decade of age in men. The serum DHEAS levels were significantly lower in the younger patients with ED compared with non-ED patients. Diminished DHEAS levels, especially in young men with ED, may either be an etiologic factor for ED or a negative consequence of it. However, patients treated with DHEA had a statistically significant increase in all domains of the IIEF in contrast to the placebo group. Interestingly, the serum DHEAS levels increased significantly after sildenafil citrate treatment in the ED group (especially in patients younger than 50 years). Also, patient age was an important factor affecting the sildenafil citrate response [42].
The first clinical effects were reported after 8 weeks of DHEA treatment and a remarkable improvement in maintaining the erection after 16 weeks. Prostate volume, postvoid residual, prolactin and PSA were not significantly changed after DHEA therapy [34]. Despite the evidence that has questioned the validity of improvement in sexual function when treatment relied solely on DHEA administration [43], several previous studies had demonstrated the usefulness of DHEA in treating sexual dysfunction associated with testosterone or DHEA deficiency [34]. A nice explanation of that effect was demonstrated as both testosterone and DHEA are considered central neurosteroids and have been found to modulate endothelial function, which ultimately influence libido and penile erections [44]. Several studies on other organs support the protective role of DHEA and DHEAS i.e., reduction of vascular stenosis in heterotopic heart transplants [45]. Because there is also some experimental evidence for direct effects on the brain, the possibility of a central effect of DHEA might be evident. An interesting mechanism that could better define the role of DHEA in sexual performance is that administration of DHEA results in biosynthesis of active androgens by tissue targets without representation in the peripheral circulation [10].
Although experimental studies had demonstrated that DHEA has direct genomic and nongenomic effects on the vascular endothelium, however its clinical effect as a facilitator of penile erections is not evident [46]. Most of the literature had not confirmed the role of DHEA in the field of sexual medicines [4347]. Additionally, other studies questioned the concept of DHEA as a neurosteroid with a central putative effect on libido [48], although this hormone had been found to influence self-esteem and mood in younger individuals [49]. Furthermore, the evidence-based studies supporting an anti-aging, anti-inflammatory, antiatherosclerotic actions, and antidepressant effect of DHEA supplementation are often poor [5051] (Table 1).
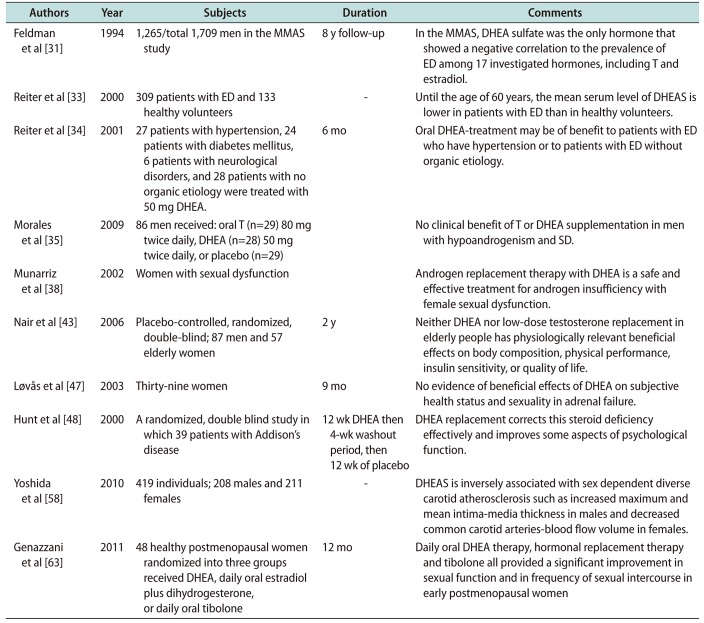
Table 1
Summary of different clinical trials that assessed DHEA in ED and other conditions
| Authors | Year | Subjects | Duration | Comments |
|---|---|---|---|---|
| Feldman et al [31] | 1994 | 1,265/total 1,709 men in the MMAS study | 8 y follow-up | In the MMAS, DHEA sulfate was the only hormone that showed a negative correlation to the prevalence of ED among 17 investigated hormones, including T and estradiol. |
| Reiter et al [33] | 2000 | 309 patients with ED and 133 healthy volunteers | - | Until the age of 60 years, the mean serum level of DHEAS is lower in patients with ED than in healthy volunteers. |
| Reiter et al [34] | 2001 | 27 patients with hypertension, 24 patients with diabetes mellitus, 6 patients with neurological disorders, and 28 patients with no organic etiology were treated with 50 mg DHEA. | 6 mo | Oral DHEA-treatment may be of benefit to patients with ED who have hypertension or to patients with ED without organic etiology. |
| Morales et al [35] | 2009 | 86 men received: oral T (n=29) 80 mg twice daily, DHEA (n=28) 50 mg twice daily, or placebo (n=29) | No clinical benefit of T or DHEA supplementation in men with hypoandrogenism and SD. | |
| Munarriz et al [38] | 2002 | Women with sexual dysfunction | Androgen replacement therapy with DHEA is a safe and effective treatment for androgen insufficiency with female sexual dysfunction. | |
| Nair et al [43] | 2006 | Placebo-controlled, randomized, double-blind; 87 men and 57 elderly women | 2 y | Neither DHEA nor low-dose testosterone replacement in elderly people has physiologically relevant beneficial effects on body composition, physical performance, insulin sensitivity, or quality of life. |
| Løvås et al [47] | 2003 | Thirty-nine women | 9 mo | No evidence of beneficial effects of DHEA on subjective health status and sexuality in adrenal failure. |
| Hunt et al [48] | 2000 | A randomized, double blind study in which 39 patients with Addison's disease | 12 wk DHEA then 4-wk washout period, then 12 wk of placebo | DHEA replacement corrects this steroid deficiency effectively and improves some aspects of psychological function. |
| Yoshida et al [58] | 2010 | 419 individuals; 208 males and 211 females | - | DHEAS is inversely associated with sex dependent diverse carotid atherosclerosis such as increased maximum and mean intima-media thickness in males and decreased common carotid arteries-blood flow volume in females. |
| Genazzani et al [63] | 2011 | 48 healthy postmenopausal women randomized into three groups received DHEA, daily oral estradiol plus dihydrogesterone, or daily oral tibolone | 12 mo | Daily oral DHEA therapy, hormonal replacement therapy and tibolone all provided a significant improvement in sexual function and in frequency of sexual intercourse in early postmenopausal women |
![]()
Go to :
DEHYDROEPIANDROSTERONE DECLINE AND AGE-RELATED DISORDERS
Although the underlying mechanism of organic ED in both middle-age and older men is basically the same, the middle-aged men's ED is assumed to have some difference from older men's ED [52]. The relation between biological, psychosocial, and lifestyle factors in terms of the age-related increase in ED seems to be best explained by their concomitant influence on general health [53]. This notion is supported by the recent results, which indicate that perceived general health, as a proxy of general health, is associated with a buffered age-related increase in ED [754].
Reduction of DHEA with aging is clinically relevant and has been related to a variety of age-related conditions [54]. A positive relationship between diminution of DHEA levels and decline in muscle mass, muscle strength, as well as mobility and a higher risk for falls, has been reported with aging [5556]. The relationship between DHEA levels and cardiovascular risk factors such as dyslipidemia and hyperglycemia are inconsistent [54]. Nevertheless, studies have shown that low DHEA levels are related to a higher risk for atherosclerosis, heart failure, cardiovascular complications, and overall mortality [575859]. A meta-analysis of endogenous DHEA on cardiovascular disease risk indicates the variations in metabolic effects of DHEA and suggests inconsistency in the positive effects of DHEA on cardiovascular disease [60].
The relationship between low level of DHEA and mood disorders and depression symptoms were more obvious in the literature [61]. Furthermore, DHEA supplementation has shown positive effects on mood as well as sexual function both for men and for women [6263].
Increased DHEA concentrations under hypoglycemic conditions denotes stimulation of the hypothalamic-pituitary-adrenal axis on hypoglycemic stress. Therefore, decline of androgen may have deleterious effects on glycemic control and ultimately therapeutic effect in type 2 diabetes mellitus (DM).
In one of our previous studies, we have assessed the pattern of type-2 DM-associated androgen alteration in patients with ED. We have shown that there were significant associations between low levels of total testosterone or DHEAS and poor control of DM [64]. Furthermore, in a consequent study we have demonstrated that there were significant associations between good control of DM, decreased fasting blood sugar, and achievement of normal levels of testosterone at 3- and 6-month follow-up visits. However, no significant associations were detected between controls of DM or decreased fasting blood sugar and change in DHEAS and insulin levels [65]. In addition, administration of testosterone to hypogonadal men improves insulin sensitivity and glucose homeostasis [66]. Earlier study reported no significant linear correlations between total or free testosterone with fasting plasma glucose; however, total testosterone was negatively correlated with glycosylated hemoglobin levels [67]. Among other researchers, we expanded the current knowledge regarding, the percentage of patients with type 2 DM with subnormal levels of total testosterone or DHEAS is much higher than that observed with subnormal levels of these androgen in patients without DM. Further study had shown that the existence of chronic diseases subtracts 10% to 15% from the values of androgens found in men without chronic diseases [68]. Other study had shown also, no positive effects on erectile function were found when conditions such as diabetes or neurological disorders were present [34].
The mechanisms of androgen alteration in men with DM have not been completely discovered. It has been shown that androgen deficiency in type 2 DM is commonly associated with hypogonadotropic hypogonadism [67]. A more recent study showed that in middle-aged pre-diabetic men, the more severe lower urinary tract symptoms were associated with low total testosterone and DHEAS, while in elderly men were associated with low free testosterone and DHEAS [69].
Go to :
FUTURE THERAPEUTIC SUPPLEMENTATION OF DEHYDROEPIANDROSTERONE
DHEA has gained a lot of attention and media interest as a dietary supplement and sold over the counter in some countries as in the USA. In Europe, it is either forbidden as in France or subjects to medical prescription as in Switzerland. Since long time, alleviation of aging consequences was a dream to obtain durable and healthy life and to sustain a better quality of life. DHEA is recently proposed as an antiaging medicine and is considered as a “fountain of youth” hormone. As DHEA is claimed to have several positive effects on age-related disorders. It would be theoretically transformed according to local and general hormone needs.
As a potential future therapy, DHEA supplementation in specific indications such as osteoporosis, mood and cognitive disorders, sexual well-being and rehabilitation protocols, needs to be better studied in more prospective multicenter and larger studies. We believe that the route to achieve an ideal antiaging supplementation, which should be readily available, effective and safe, is still long. Therefore, physicians prescribing DHEA should consider and inform their patients of the fact that long-term effects not only concerning efficiency, but also safety, remains uncertain [70].
Go to :
CONCLUSIONS
Several studies had demonstrated that DHEA level is declined as a part of aging. It is not yet clear whether this decline should be considered as a physiologic reflection of the aging process or whether active administration of DHEA might help to prevent and treat age-related disorders. Furthermore, large-scale well-designed prospective studies are warranted to better define indications and therapeutic implications of DHEA in men with ED [7172].
Go to :
 XML Download
XML Download