

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Circumcision is the most common procedure performed on newborns. While it has been performed for thousands of years for religious and medical reasons, its use is still controversial. Regional and cultural discrepancies in circumcision rates exist nationally and internationally. Indeed, national medical panels from different countries have arrived at different conclusions and recommendations when reviewing the literature. While circumcision rates in the United States are around 65% to 75% with the American Academy of Pediatrics concluding ‘health benefits of newborn male circumcision outweigh the risks’, England has circumcision rates around 15% with the NHS website stating ‘Most health professionals in England would argue that there are no medical reasons why an otherwise healthy baby boy should be circumcised’ [1]. Similarly, recent Canadian Pediatric Society recommended circumcision in only certain circumstances; however, the methodology of the evidence evaluation has been questioned [23]. The Royal Dutch Medical Association recommends deterrence [4].
Nevertheless, many health benefits of circumcision have been suggested, including lower rates of urinary tract infection (UTI), human immunodeficiency virus acquisition, herpes simplex virus acquisition, syphilis transmission, penile cancer, balanitis, phimosis, bacterial vaginosis in female partners, human papilloma virus transmission and cervical cancer in female partners [1]. Indeed, the Centers for Disease Control (CDC) recently released proposed recommendations for counseling parents and uncircumcised adolescents and adult males about the benefits of circumcision [5]. However, the low overall rate of UTIs in the infant population demonstrated in several large cohort studies, suggested that the number needed to circumcise to prevent one hospitalization for UTI was between 100 and 200 [67]. Importantly, pediatric studies of UTI and circumcision have been restricted to UTI alone, thus other health sequelae, such as renal or hypertensive disease, have not been evaluated [891011]. While some studies reported complication rate of up to 10%, most contemporary series report complications rates well below 0.5% [112]. While most complications are minor, several societies have voiced concerns about the risk to benefit ratio. Even the American Academy of Pediatrics, which acknowledges the benefits of circumcision, has stopped short of recommending neonatal circumcision and instead has suggested the procedure should be offered to the parents of healthy children so that an informed decision can be made [1]. In contrast, the CDC's detailed report on circumcision calculates the benefits of circumcision outweigh the risks by 100 to 1 [13].
A meta-analysis in 2013, which included data on 407,902 children (19 studies) as well as older boys and men, concluded that there is a lifetime benefit to circumcision which prevents UTI [14]. A recent systematic review published in 2017 concluded that early infant circumcision should not be considered controversial and suggested that a decline in national rates of circumcision were a threat to public health [4]. However, the most recent Cochrane review identified no randomized or quasi-randomized controlled trials (RCTs) examining circumcision and UTI [15]. The authors concluded that further data was needed before circumcision could be recommended [1]. Indeed, there are significant sociodemographic and economic differences between families utilizing circumcision which may also influence relevant outcomes [16]. However, limiting the analysis to only randomized controlled trial RCT, excludes the wealth of data provided by observational studies over the past several decades.
TECHNIQUES BEYOND RANDOMIZED CONTROLLED TRIALS
There are significant financial, ethical, and logistical challenges to performing RCTs. In such instances, investigators have used observational data to attempt to guide policies. Yet observational data may be biased as differences in baseline characteristics may impact both the treatment and outcome. However, with detailed clinical data, many confounding factors can be adjusted for using analytical models. Moreover, several analytic techniques can help account for overt or hidden biases especially when unmeasured patient characteristics can affect the disease and outcome. We used data from an ongoing study of a geographically and demographically diverse cohort of industrial workers and their families to determine the association between circumcision and the incidence of UTIs and surgical complications to simultaneously assess risks and benefits of neonatal circumcision.
The design of the parent study has been previously described [17181920212223]. Briefly, as part of continuing monitoring of employee health and safety, employee medical, insurance, and workplace records are compiled. Data on over 120K employees from around the US (i.e., 24 states) is available with complete medical claims and pharmacy records as well as insurance claims data for all covered spouses and dependents.
Using insurance claims data, we identified boys that underwent neonatal circumcision prior to 1 month of age. The circumcised group was compared to uncircumcised boys. Diagnosis and treatment codes were used to identify urinary infections, surgical complications, or urologic imaging.
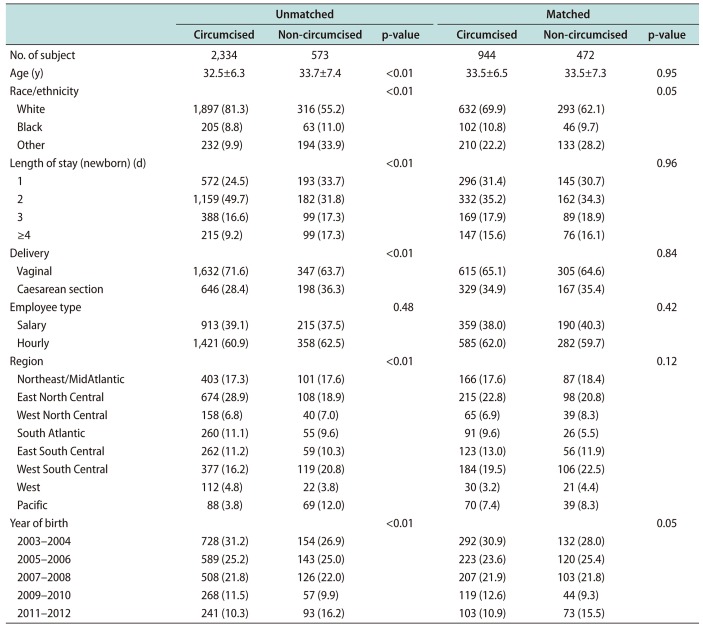
In all, we identified 2,334 boys who underwent neonatal circumcision and 573 who did not during the study period. Method of delivery and length of stay were also associated with circumcision status (Table 1). Propensity-based matching produced 944 circumcised boys and 472 uncircumcised boys matched 2:1 with similar patient characteristics, indicating a high degree of similarity in the distributions of prognostic variables (Table 1).
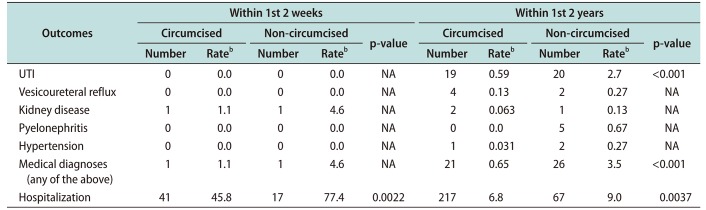
A total of 39 boys were diagnosed with a UTI during 3,945.5 person-years of follow-up. The hazard ratio (HR) for UTI of circumcised boys was 0.29 (95% confidence interval [CI], 0.15–0.58) compared to uncircumcised boys. Using the propensity-matched control, circumcision was associated with a 75% lower rate of UTI (HR, 0.23; 95% CI, 0.10–0.54) comparing the propensity matched cohort. Similar results were also seen for propensity score risk adjustment (HR, 0.29; 95% CI, 0.15–0.59) (Table 2).
Importantly, no difference in the rate of UTI was identified in the first two weeks of life. However, up to 2 years of age, uncircumcised boys had a higher rate of UTIs compared to circumcised boys (2.68 per 100 person-years vs. 0.59 per 100 person-years), the difference was statistical significant (p=0.0005). The number needed to treat (NNT) with circumcision to prevent one UTI was 37. This number decreased to 25 when we included other sequelae (i.e., vesicoureteral reflux, renal disease, pyelonephritis, and hypertension) into the avoided outcomes. The overall rate of hospitalization was also significantly higher for uncircumcised boys (Table 2). Importantly, the incidence of other diseases not associated with urologic disease did not vary based on circumcision status such as bronchiolitis, respiratory syncytial virus infections, and ear infections were similar across all time periods examined. Similar results were seen with propensity matching or propensity score adjusted models.
In addition, a significantly higher rate of radiologic procedures (i.e., renal ultrasounds) occurred in uncircumcised boys (Table 3). Unlike UTIs, the difference in radiologic evaluation between circumcised and uncircumcised boys began in the first 2 weeks of life. Over the first two years, uncircumcised boys had a significantly higher rate of radiologic evaluation of urinary organs compared to circumcised boys (2.2% vs. 0.8%). The number needed to treat with circumcision to prevent one radiologic evaluation was 17.
When examining surgical complications, no differences were seen at each time point for composite end-points when comparing circumcised and uncircumcised boys. Hemorrhage, infection, meatal stenosis, need for repeat interventions, or unspecified complications were similar between groups (p>0.05).
DISCUSSION
Prior reports have demonstrated a lower UTI rate in boys after circumcision. The American Academy of Pediatrics Ad Hoc Task Force on Circumcision reported on data from 427,698 infants born in all US Army hospitals between [24]. They noted an 11-fold increased UTI rate among uncircumcised boys compared to circumcised boys which was reflected in the decline prevalence of neonatal circumcision over this time period. A cohort study from Canada reported a risk reduction of 3.7 fold among 69,100 eligible boys born in 1993 to 1994, but given the low rate of UTIs, the authors estimated that 195 circumcisions must be performed to prevent on UTI [7]. While socioeconomics were estimated with geocoding, the homogeneity of the population limits generalizability. An analysis of members of the Kaiser Permanente Northern California system in 1996 identified 28,812 infants. A 10-fold higher cost for managing UTIs in uncircumcised boys was noted reflecting higher rates of hospitalization [6]. Moreover, the odds of a UTI declined 90%. However, the study represents a single region of the country and was unable to account for race/ethnicity, socioeconomic factors, and delivery characteristics which may impact circumcision and UTI rates.
UTIs early in life can lead to renal and hypertensive disease, thus it is important to consider these diseases as well. Moreover, a UTI in a male often prompts evaluation including urologic imaging. In addition to UTIs, circumcised boys also experience a lower utilization of diagnostic imaging with its associated costs (financial and emotional).
As with all observational data, it is important to note the important baseline sociodemographic differences among boys utilizing and not utilizing circumcision as this can lead to bias. However, application of multivariable, propensity score risk adjustment, and propensity score matching can minimize the impact of overt bias in patient characteristics [2526].
The mechanism whereby circumcision may lower urinary infection rates has been studied. Studies demonstrate an accumulation of urinary pathogens under the prepuce and in the urethra of uncircumcised boys [27]. While severity of infection, including renal involvement or need for hospitalization, is affected by the specific urinary pathogen as well as the patient's anatomy, a urinary predisposition will increase a patient's rate of urologic complications. Consistent with existing data, the risk reduction of UTI associated with circumcision is greatest early in life [28]. As chronic renal disease may predispose to additional lifelong health impairments, it is possible early circumcision may prove more beneficial with longer follow-up into the early and middle adulthood [1011].
It is important to note that estimates using observational data can be subject to unmeasured selection bias. However, given that RCTs cannot guide all clinical decisions, in certain cases, observational data can be useful. Current data identified a consistent reduction in UTI of circumcision and a NNT of 25 to 100 which implies that circumcision demonstrates a higher efficacy than infant influenza vaccination with an estimated number needed to vaccinate of >1,000 [29].

 XML Download
XML Download