

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Cleft lip and palate are the second most frequently occurring major congenital anomalies (1:750 to 1:1,000 live births)12, with club foot being the most common34. In the spectrum of congenital orofacial anomalies, cleft lip and palate remain the most common5. The reconstruction of lip defects involves both extraoral and transoral incisions, and primary closure of the surgical wound with suture materials is an essential step in this process678.
The generally accepted characteristics of an ideal suture material include superior tensile strength, good knot security, excellent handling characteristics, minimal tissue reaction, absence of allergenic properties, resistance to infection, and eventual absorption when tissue repair has reached a satisfactory level910. Suture materials are required, in practically every surgical operation, for reconstruction of incised or damaged tissues and for ligation of major blood vessels11. Some of the complications following surgery may be directly attributable to the suture material itself9. It is therefore essential that every surgeon have knowledge of the properties and behaviors of different sutures because the type of material used will undoubtedly influence the results of surgery11.
Traditionally, skin closure in cleft lip repair has been performed using only fine, non-absorbable sutures to minimize scarring12. However, the disadvantage of using non-absorbable sutures lies in the need for suture material to be removed postoperatively, which often necessitates sedation or general anesthesia912. Topical, local anesthetic preparations have also been tried, but these are not without risk12. The removal of sutures is often torturous for a baby, who makes violent efforts to ease out of restraints. It is also extremely distressing for the parents, who must witness their child's distress12. Absorbable sutures have also been used in the past by others with good results13.
Therefore, the aim of the study was to compare immediate wound healing complications following the use of absorbable and non-absorbable sutures in cleft lip repair.
II. Materials and Methods
This was a randomized controlled study of postoperative wound healing complications of cleft lip repair following the use of either absorbable (Vicryl) or non-absorbable (Nylon) skin sutures. All subjects who presented with congenital cleft lip and those who required lip revision after primary cleft lip repair and satisfied the inclusion criteria at the cleft clinic of Lagos University Teaching Hospital (Idi Araba, Lagos State, Nigeria) between May 2013 and October 2014 were included in the study. Approval for the study was obtained from the Health Research and Ethics Committee of Lagos University Teaching Hospital (approval no. ADM/DCST/HREC/VOLXVI/APP/747).
All subjects were randomly allocated to either Group A (Vicryl skin suture) or Group B (Nylon skin suture) with the aid of a computer generated (GraphPad software, La Jolla, CA, USA) random sequence. Unilateral cleft lip and bilateral cleft lip were repaired at age 3 to 6 months or as soon as possible after presentation for those that presented later. Surgical repair was carried out under general anesthesia for 57 subjects, while surgery conducted under local anesthesia in 3 subjects.
Surgical repair of unilateral cleft lip was performed with either Millard rotation advancement or the Tennison-Randall triangular surgical technique, while bilateral cleft lips were repaired using the Millard fork flap technique. After suturing was complete, the skin wound was dressed with Sofra-Tulle gauze, over which dry gauze was placed, and plaster was applied over the dry gauze.
Preoperative prophylactic antibiotics (ceftriaxone 100 mg/kg body weight) and dexamethasone 0.4 mg/kg body weight were given intravenously.
1. Suture materials
Group A: Suturing of the skin layer was done using a 1.5 metric Ethicon-coated Vicryl 4/0 suture on a cutting needle, size 17.5 mm (Johnson & Johnson, New Brunswick, NJ, USA).
Group B: Suturing of the skin layer was done using a 1.5 metric Nylon 4/0 suture on a cutting needle, size 17.5 mm (Ogotex, Lagos, Nigeria).
2. Postoperative wound care
Sofra-Tulle gauze dressing was applied for the first 24 hours postoperation after cleaning with Hibitane-in-water. The wound was subsequently left open, followed by gentle daily cleansing with sterile normal saline applied with gauze swabs until all non-absorbable sutures were removed 7 days postoperatively. Absorbable sutures were left to resorb. The subjects were reviewed regularly post-surgery and evaluated at postoperative days (POD) 3, POD7, and POD14 after repair14.
All wounds were evaluated on POD3, POD7, and POD14 for the presence of tissue reactivity, wound dehiscence, local wound infection, and any other wound healing complications.
3. Tissue reactivity
Tissue reactivity was defined as an erythema and/or crust at the suture site that extended more than 3 mm from the surgical wound14. All subjects had their repaired lips examined on POD3, POD7, and POD14 for evidence of erythema and/or crust extending 3 mm from the surgical wound. This was documented as ‘yes’ or ‘no’ depending on whether erythema was present or absent, respectively. Tissue reactivity was managed by cleaning the wound with normal saline and follow up until resolution of the tissue reaction.
4. Wound dehiscence
This was defined as spontaneous suture disruptions that were not the result of trauma such as scratching3. Review of the wound site for evidence of spontaneous suture disruptions was performed on POD3, POD7, and POD14. This was documented as ‘yes’ or ‘no’ depending on whether it was present or not. For cases with wound dehiscence, the wound was cleaned with normal saline, Sofra-Tulle gauze dressing was applied, and the patient was followed until resolution.
5. Local wound infection
Local wound infection was diagnosed when the wound contained purulent material and/or showed other clinical signs of infection (warmth, erythema, local tenderness)3. Surgical wounds were examined for evidence of purulent discharge with or without other signs of local infection such as warmth, erythema, and local tenderness on POD3, POD7, and POD14. This was documented as ‘yes’ or ‘no’ depending on whether one or more of these clinical signs of infection were present or not. In cases of local wound infection, the wound was cleaned with normal saline, and Sofra-Tulle gauze dressing was applied. Subjects were placed on an extended antibiotic regimen (ceftriaxone 50 mg/kg body weight for 4 days after the initial dose given to all subjects postoperatively).
Data analysis was performed using SPSS for Windows (ver. 17.0; SPSS Inc., Chicago, IL, USA). Data is presented in the form of tables. Other descriptive and inferential statistics were used as appropriate. The complication rate between the two groups was compared using chi-square and Fisher's exact tests (for cells whose expected count was less than 5). For all comparisons, P<0.05 was adopted as the criterion for establishing statistical significance.
III. Results
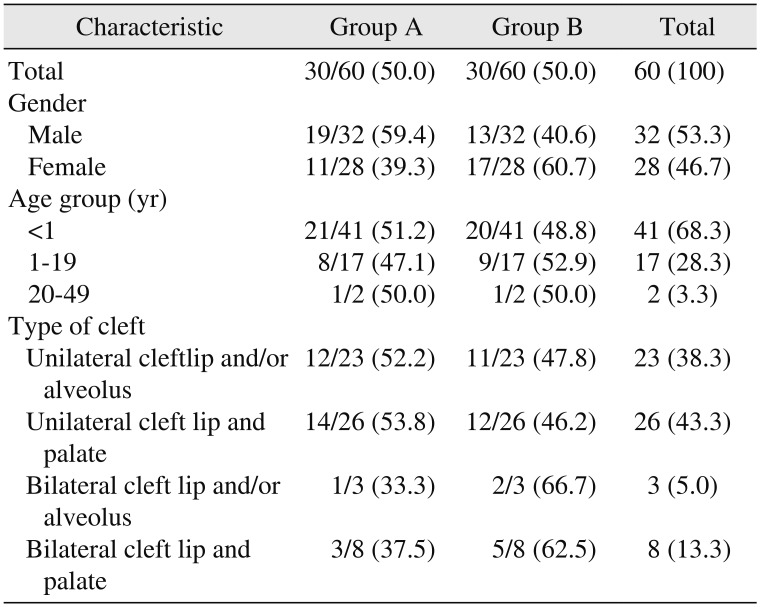
A total of 60 subjects (30 in each group) who required cleft lip repair were included in this study. There were 32 males and 28 females, resulting in a ratio of 1.1:1. The overall age of subjects in the study ranged from 3 months to 48 years. The median age of the subjects was 0.39 years. There was no statistical difference in gender distribution between the two groups (P=0.12).
The most common presentation of orofacial clefts was unilateral cleft lip and palate (43.3%), followed by unilateral cleft lip and/or alveolus (38.3%), bilateral cleft lip and palate (13.3%), and bilateral cleft lip and/or alveolus (5.0%). Table 1 shows the age, gender, and pattern of presentation of orofacial clefts in the two groups.
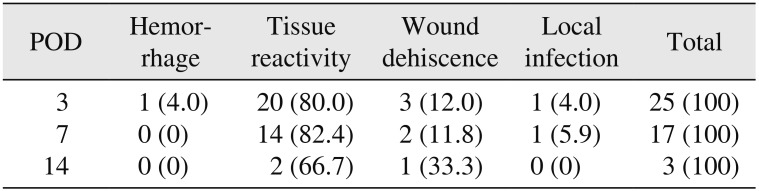
The different types of wound healing complications observed following cleft lip repair were hemorrhage, tissue reactivity, wound dehiscence, and local wound infection. A total of 25 complications were observed on POD3 in 20 subjects. The most common complication was tissue reactivity, accounting for 80% of the complications.(Table 2) There was only 1 case of local wound infection (4.0%). The total number of complications thereafter decreased to 17 cases (POD7) and 3 cases (POD14). Tissue reactivity and wound dehiscence were observed throughout the observation period. Twenty-nine unilateral clefts were repaired with the Millard rotation advancement technique, and 20 clefts were repaired with the Tennison-Randall triangular surgical technique. No significant difference between the two techniques was found in the incidence of immediate wound healing complications (P>0.05).
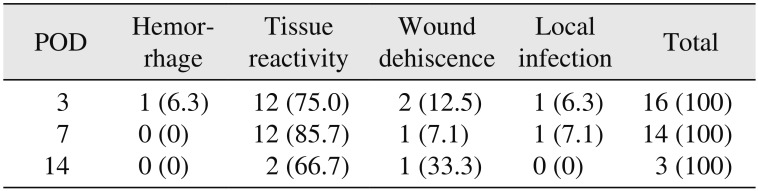
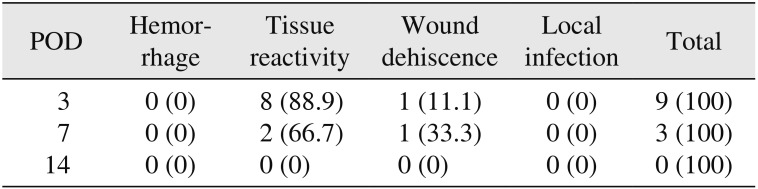
Tables 3 and 4 show the types of complications observed in the two groups. The incidence of complications decreased over the observation period. All four different types of wound healing complications were observed in Group A, while only two types of complications (tissue reactivity and wound dehiscence) were seen in Group B.
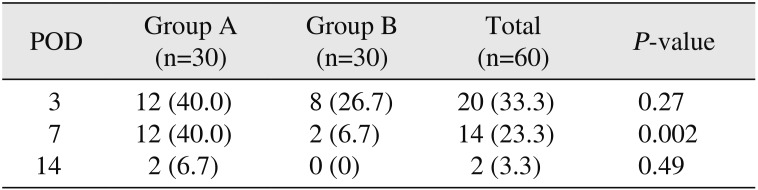
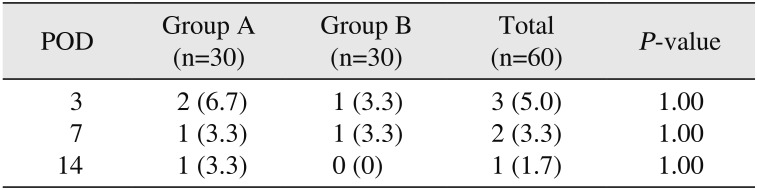
Table 5 compares tissue reactivity in both groups. There were more cases (12 cases) of tissue reactivity in Group A compared to in Group B at POD3, POD7, and POD14; however, the difference was only statistically significant at POD7 (P=0.002). In addition, the 2 cases of tissue reactivity on POD14 occurred in the Group A. There was no statistically significant difference in the incidence of wound dehiscence between the two groups throughout the observation period. (Table 6) The two cases of wound infection recorded (one each on POD3 and POD7) were seen in the Group A. No case of wound infection was observed in either group on POD14.
IV. Discussion
The most frequently reported postoperative wound healing complications in cleft lip repair include hypertrophic scars, wound dehiscence, local infection, hemorrhage, tissue reactivity, and lip notching151617. Most of these complications occur at different times postoperatively161819. They are generally divided into early and late postoperative complications1920. There have been several reports focused on late postoperative wound healing complications; however, late complications require a longer period of evaluation postoperatively161920. Hypertrophic scarring and lip notching are usually studied as late postoperative wound healing complications15. The present study evaluated early postoperative surgical wound complications following cleft lip repair.
The wound healing process generally takes place in three stages: inflammation, proliferation, and remodeling2122. It is, however, a continuous process in which the beginning of one phase and the end of another cannot be clearly defined, and there is considerable overlap between the phases21. Wound healing was evaluated within 14 days after surgery in the present study, which explains why most of the complications identified were related to the inflammatory stage or within the overlap between the inflammatory/proliferation stages of wound healing. Wound healing complications related to the remodeling stage, such as hypertrophic scar/keloid, require a longer period of postoperative evaluation.
In the present study, hemorrhage, tissue reactivity, wound dehiscence, and local wound infection were the wound healing complications recorded. This is similar to previous studies where hemorrhage, wound dehiscence, and local infection were reported following cheilorraphy1722. Several authors also reported tissue reactivity, wound dehiscence, and local infection as the wound healing complications following various surgeries carried on pediatric patients232425262728. Some authors opined that longer hospital stay contributed to the occurrence of these complications1729.
The prevalence of wound healing complications in this study was 33.3%. Ugburo et al.16 and Kim and Rothkopf17 also reported early postoperative wound healing complications following cheilorraphy but with lower incidence (6%). However, Lees and Pigott19 reported none of these complications. The reason given for the lower rates of complication in studies by Ugburo et al.16 and Kim and Rothkopf17 was the shorter period of hospitalization after cheilorraphy, as subjects were discharged within 24 hours of the operation, unlike in the present study, where the subjects were admitted for a minimum of 5 days postoperatively. This might have contributed to the higher prevalence of complications recorded in this present study.
Clinically significant postoperative hemorrhage is uncommon following cheilorraphy3031. Bleeding can be avoided with meticulous dissection, hemostasis, and closure30. Care is taken during surgery to perform the operation using a local anesthetic agent containing adrenaline30. Some surgeons perform the surgery using loupe or microscopic magnification, identifying any small bleeding points. Also, layered closure of the mucosa, muscle, and skin also ensures a dry surgical field30. A small amount of bleeding is expected post-operation and might appear somewhat magnified as it mixes with oral and nasal secretions30. Demey et al.20 reported a 3.1% incidence of hemorrhage following cleft lip repair, the result of which was in agreement with that of a study by Tempest32. In the present study, only one subject (1.7%) had an episode of bleeding on the third day post-cheilorraphy. As observed by other authors20, slipping of sutures was responsible for the bleeding. The loss of blood did not warrant blood transfusion as the bleeding ceased with compression only.
Tissue reactivity is indicative of an inflammatory response, which develops during the first few days after suturing3334. Various suture materials, including cotton, braided silk, polyester, Nylon, and cat gut, have been frequently investigated with respect to tissue reactivity3335. However, the study outcomes remain debatable3335. Polyester sutures have been reported to cause a mild inflammatory reaction, whereas cotton threads have been associated with an intense tissue inflammatory response35. Parell and Becker23 compared the use of Vicryl and Prolene on facial skin wounds and reported a total prevalence of 4.5%. This was similar to the prevalence of 4% recorded by Edwards and Elson24. However, Mouzas and Yeadon25 reported the prevalence of tissue reactivity to be 19% in a study carried out in the United Kingdom in 1975. Technological advancement has been credited for the lower incidence of tissue reactivity in the American and European studies mentioned earlier, which may also explain the lower incidence of tissue reactivity in the study carried out in the United Kingdom in 1995 compared to the one carried out 20 years earlier. The prevalence of tissue reactivity in this study was 33.3%, which was far higher than reported by other authors. The higher prevalence rate could potentially be associated with the higher propensity for formation of inflammatory tissue reactions and other complications like hypertrophic scars, seen more frequently in the black population relative to their white counterparts36. Patients with tissue reactivity in this study were managed by cleaning the wound with normal saline until resolution of the tissue reaction.
Wound dehiscence or rupture of a wound has been attributed to increased pressure on the healing site caused by vomiting, coughing, or retention of debris26. This may lead to inadequate formation of granulation or disruption of the fragile blood vessels26. The prevalence of wound dehiscence in cleft lip surgery has been reported to vary from 0% to 7.5%3. Reinisch et al.30 observed wound dehiscence in 7 out of 123 cleft lip subjects (5.7%). Five of these subjects were older than nine months of age. Age-related mobility and activity were the reasons given for this outcome. Holger et al.27 reported the prevalence of wound dehiscence to be 4.5%. The 5% prevalence of wound dehiscence in the present study is similar to that reported by others30. This similarity might be due to the similar tensile strength of Vicryl, which was used in this study, and chromic catgut, used in the earlier-mentioned studies, in cutaneous wounds37. Regular debridement of the healing site led to satisfactory resolution of the problem.
The low incidence of wound infection recorded in the present study is comparable to reports by others28. This may be due to the use of aseptic technique during surgery, as well as meticulous wound care postoperatively. Wound infection was managed by debridement and an extended antibiotic regimen.
The occurrence of postoperative hemorrhage and local wound infection in a one patient in Group A might either be due to unknotting of the absorbable suture material or poor handling of the surgical site by the patient's mother.
A comparison of the incidences of tissue reactivity in the two study groups showed that tissue reactivity was observed more frequently in the absorbable suture group than in the non-absorbable group throughout the evaluation period, although the difference was only significant on POD7. Parell and Becker23 compared tissue reactivity associated with the use of Vicryl and prolene in facial skin wounds and found no difference in the incidence of tissue reactivity. Edwards and Elson24 did not record any cases of tissue reactivity in the absorbable (polydioxanone) group, whereas an incidence of 8.6% was recorded in the non-absorbable (Nylon) group. Mouzas and Yeadon25 in another study comparing absorbable (Dexon) and non-absorbable (Nylon) sutures in wound repair reported prevalence of 16% and 19.7% tissue reactivity in the absorbable (Dexon) and non-absorbable (Nylon) groups, respectively. Katz et al.35 and Leknes et al.38 suggested that bacterial adherence to suture materials, especially the multi-filament types, plays a pivotal role in the causation of tissue reactivity. Hochberg et al.37 and Tajirian and Goldberg39 also reported that Nylon has a lower chance of inducing tissue reactivity than Vicryl. These results might explain why there were more cases of tissue reactivity in the absorbable (Vicryl) group in this present study.
In the present study, there was no significant difference in the incidence of wound dehiscence in the two studied groups. Nylon exhibits a lower coefficient of friction than Vicryl, which increases the likelihood of a knot unraveling, thereby leading to wound dehiscence when Nylon is used. However, use of an increased number of throws in the knot compensates for this limitation when skin is sutured using Nylon37. Holger et al.27, in a study carried out on wound dehiscence associated with absorbable (chromic catgut) and non-absorbable (Nylon) sutures used for facial lacerations, reported more cases in the absorbable group (6%) than non-absorbable group (2%). In contrast, Karounis et al.28 in another study on pediatric facial lacerations repaired with either chromic catgut or Nylon reported a higher prevalence of wound dehiscence in patients who underwent repair with Nylon (11.1%) than in those who underwent repair with chromic catgut (2%). Gabrielli et al.14 and Marcusson et al.40 found no statistically significant difference in the prevalence of wound dehiscence between absorbable and non-absorbable sutures used for plastic surgery procedures. The type and caliber of sutures have been reported not to have any clinically significant impact on short-term postoperative wound healing complications. Instead, the general characteristics of patients (age and sex), wound length and site, and the surgeon's experience are the primary risk factors responsible for the outcomes of interest14.
The incidence of local wound infection in the present study was low and was only observed in the absorbable group. The use of proper aseptic technique may have contributed to the low prevalence of wound infection. Fluid absorption and capillarity are inherent properties of multi-filamented sutures and are related to the ability of the suture to transport and spread micro-organisms leading to wound infection. Vicryl, being a multi-filamented suture, is expected to exhibit these properties more often than the mono-filamented suture, Nylon. Rothenburger et al.41 reported that the multi-filamentous nature of a suture material like Vicryl plays a role in the causation of local wound infection. Murphy et al.42 also reported a low incidence (2.2%) of surgical wound infection associated with absorbable (polyglyconate) sutures. Several other authors have also reported no/low prevalence of surgical wound infection associated with absorbable sutures2324.
V. Conclusion
Hemorrhage, tissue reactivity, wound dehiscence, and local wound infection were identified as wound healing complications following cleft lip repair. While all four were observed in the absorbable group, only tissue reactivity, wound dehiscence, and local wound infection were identified in the non-absorbable group. Tissue reactivity was more common in the absorbable group than in the non-absorbable throughout the evaluation period, although the difference was only statistically significant on POD7. There was no significant difference in the incidence of wound dehiscence between the two groups on POD3, POD7, and POD14. In addition, there was no significant difference in the incidence of wound infection between the two groups on POD3 and POD7. No cases of wound infection were observed in either group on POD14. Particular attention must be paid to detect the occurrence of wound healing complications, particularly tissue reactivity, whenever a Vicryl suture is used for skin closure during cleft lip repair.
 XML Download
XML Download