

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Dear Editor:
Onychomatricoma is a rare benign fibroepithelial tumor of the nail unit. It typically presents as thickening of the nail plate, splinter hemorrhage, xanthonychia, and transverse overcurvature, and generally arises in patients with pale skin. Onychomatricoma rarely manifests longitudinal melanonychia (LM). In this case, it is termed pigmented onychomatricoma. However, the occurrence of onychomatricoma in the Asian population is rare and pigmented onychomatricoma is immensely unusual12. Here, we present a rare patient with pigmented onychomatricoma.
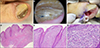
A 67-year-old man presented with an 8-month history of gray LM on the left hallux nail. He was under 2 months of targeted therapy with gefitinib for non-small-cell lung carcinoma with pericardial metastasis. Physical examination showed longitudinal gray bands with ridging on his left toe nail (Fig. 1A). Dermoscopic examination showed nail plate thickening, longitudinal parallel gray and white lines, and multiple cavities at the distal nail plate (Fig. 1B). Patient consent was gained regarding publication of all photographic materials. A nail matrix biopsy was performed to exclude subungual melanoma. Partial nail avulsion revealed a villous tumor of the nail matrix penetrating the thickened nail plate (Fig. 1C). Histopathologic examination of the excised mass revealed papillomatosis covered by nail matrix-like epithelium without stratum granulosum and spindle cell proliferation in the stroma (Fig. 1D~F). Immunohistochemical stain showed CD 34 expression of mesenchymal cells.
Pigmented onychomatricoma has been considered as an extremely rare nail tumor. Wynes et al.3 reported a case of onychomatricoma with LM mimicking a subungual melanoma. Due to the clinical resemblance of pigmented onychomatricoma and subungual melanoma, diagnosis may be challenging, hence an excisional biopsy is required to differentiate these conditions.
Recently, Di Chiacchio et al.4 analyzed 30 cases of onychomatricoma in which LM was present in seven cases (23%). Other signs included increased nail thickness (85%), splinter hemorrhages (80%), xanthonychia (73%), increased transverse overcurvature (50%), woodworm-like cavities at the free edges of the nail plate (43%), swelling and periungual erythema (50%), and pain during nail compression (30%). Therefore, a pigmented variant of onychomatricoma may not be as infrequent as previously regarded. We assume that unfamiliarity of the tumor among dermatologists may have attributed to its under-diagnosis and low prevalence.
Diagnosis of onychomatricoma is often delayed leading to inadequate management. Late diagnosis may be due to a lack of awareness of its clinical features and the fact that the tumor is usually painless4. Recently, dermoscopy has been proposed as a valuable adjuvant tool in facilitating the diagnosis of onychomatricoma. Several dermoscopic features of onychomatricoma have been reported including longitudinal parallel white lines, gray lines, splinter hemorrhage, dark dots, multiple cavities at the distal nail plate25. In our case, parallel longitudinal white and gray lines, yellowish background color, and multiple cavities at the nail edge were found.
In conclusion, we report a rare case of pigmented onychomatricoma occurred in an Asian patient. The recognition of key characteristic features of onychomatricoma is essential for early suspicion and appropriate management of this rare tumor.
 XML Download
XML Download