

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastric cancer (GC) is the fourth most frequently diagnosed cancer and the second most common cause of cancer-related deaths worldwide. Although the GC-related death rate is decreasing, the incidence of gastric and gastroesophageal (GE) junction cancers has increased abruptly in recent years [123]. In Korea and Japan, this increase includes cases of advanced, metastatic, or inoperable disease, despite the diagnosis of more early GCs by the national health endoscopy screening programs. Therefore, clinics worldwide require more effective and tolerable therapeutic methods to treat advanced, metastatic or inoperable GCs.
The phase III Trastuzumab for Gastric Cancer (ToGA) trial has reported that the addition of trastuzumab to the chemotherapy regimen significantly improved overall survival, compared with chemotherapy alone. This trial defined human epidermal growth factor receptor 2 (HER2) positivity as an immunohistochemistry (IHC) score of 3+ or positive fluorescence in situ hybridization (FISH+) result and reported an overall HER2-positive rate of 22.1% [45]. The frequency of HER2-positive GC varies considerably among studies, with reported rates ranging from 6% to 30% depending on evaluation assays and other factors; as a result, the precise figure remains uncertain [678910]. It is therefore important for local laboratories to determine the incidence of HER2 positivity among gastric and GE junction adenocarcinomas in a community setting.
The present study aimed to apply a modified scoring system and thus generate vital epidemiological data from local laboratories regarding HER2 expression in gastric and GE junction cancers in a broader and more real-life setting.
MATERIALS AND METHODS
Study design and participants
This was a non-interventional, epidemiology study conducted at 14 centers in Korea to determine the HER2 positivity rate among patients with gastric and GE junction cancer.
Tumor samples that had been stored in the pathology departments of participating centers from October 1, 2010 until the Institutional Review Board (IRB) approval date were collected retrospectively. In addition, new specimens obtained via surgical retrieval or via endoscopic biopsy were included prospectively after IRB approval (Fig. 1). The results were recorded using case report forms.

Objectives
The primary study objective was to assess the HER2 positivity rate in gastric and GE junction cancer tumor samples analyzed by local laboratories. The secondary objective was to assess correlations of the HER2 status with stage, tumor type, gastric vs. GE junction cancer, age, and sex. We described the tumor depth and lymph node metastasis according to the 7th American Joint Committee on Cancer/Union for International Cancer Control tumor node metastasis staging system (2010 revision).
HER2 test algorithm
The definition of HER2 positivity was based on an approved indication by the European Medicine Agency (EMA) (Fig. 2). The HER2 statuses of tumor tissues were examined by 18 pathologists at 14 participating centers. Tumor samples that received IHC scores of 0 or 1+ were classified as HER2-negative, and those that received IHC scores of 3+ were classified as HER2-positive, while waiving the requirement for in situ hybridization (ISH) re-testing. However, samples that received IHC scores of 2+ were subjected to silver-enhanced ISH (SISH) for HER2 status confirmation. Three central laboratories in the present study (Yeungnam University Medical Center, Pusan National University Hospital, Chosun University Hospital) subjected IHC 2+ samples to IHC re-testing before conducting SISH.

IHC scoring system
Local laboratories used 5 different IHC testing methods to evaluate HER2 protein expression according to normal practices. The most common methods used the fully automated Ventana CONFIRM HER2/neu (4B5) Antibody System (Roche Tissue Diagnostics/Ventana, Tucson, AZ, USA) and the Anti-HER2 (A0485) Antibody or HercepTest (Dako, Carpinteria, CA, USA). All re-tested cases were analyzed using the Ventana system. The slides were examined and scored by experienced pathologists at local laboratories by using the ISH scoring criteria defined in the ToGA trial (Table 1).
Table 1
HER2 gastric cancer scoring criteria used in the Trastuzumab for Gastric Cancer trial

SISH
Three central laboratories performed automated SISH analyses using the PathVysion HER2 DNA Probe Kit (Abbott/Vysis, Des Plaines, IL, USA) and Ventana INFORM HER2 DNA dual-color assay (Roche Tissue Diagnostics/Ventana). The entire assay process (deparaffinization, pretreatment, hybridization, stringency wash, signal detection, counterstaining) was fully automated.
Positive SISH was defined as a HER2 gene copy number per tumor cell to chromosome 17 copy number per cell ratio of ≥2. This ratio was calculated by dividing the total number of HER2 gene signals counted within 20 cells by the total number of chromosome 17 (centromeric probe=CEP17) signals counted in the same 20 cells. For equivocal cases, signals were counted in 20 or 40 additional cells.
Ethics statement
This study was conducted in accordance with Good Clinical Practice Guidelines and the Declaration of Helsinki. Approvals for the study protocol were gained from the independent IRB (KUGH IRB No.11-98) of each of the 14 participating institutes. Human rights and informed consent statements: All procedures were conducted in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later revisions. Informed consent or an acceptable substitute was obtained from all patients prior to inclusion in the study.
Sample size
Although no formal calculation was performed for this exploratory investigation, the sample size was primarily determined using practical considerations such as the availability of patients, laboratories, and resources. Approximately 2,000 samples were collected at 14 local laboratory centers to estimate the HER2 positivity rate in GCs. This sample size was expected to provide sufficiently precise overall and subgroup incidence estimates. For example, the 95% confidence interval (CI) around an observed incidence of 12% would range from 10.5% to 13.5% in a subgroup of 1,800 patients.
Statistical analysis
The Statistical Package for Social Sciences (SPSS) Statistics ver. 17.0 (SPSS Inc., Chicago, IL, USA) was used to conduct statistical analyses. The HER2 positivity rate was determined from local assessments and has been displayed with its 95% CI (Clopper-Pearson method). In addition, incidence estimates have been presented for subgroups defined by the type of GC (e.g., histological type or location), age, and sex. Appropriate subgroup comparisons were performed using the chi-square test for discrete variables and Student's t-test for continuous variables. A P-value <0.05 was considered statistically significant.
RESULTS
This study was conducted at 14 sites nationwide from October 11, 2011 to April 19, 2013. Although an estimated 2,000 samples were planned, 1,695 samples were collected within the planned study period to complete the study.
Of these samples, 6 were withdrawn from the study because of incompatibility with the inclusion criteria, and the rest were included in the clinical study evaluation. Furthermore, 198 of 1,689 samples were subjected to IHC re-testing, one sample was withdrawn, and 64 samples were subjected to FISH/SISH testing. Among the latter, one sample was withdrawn. Sample testing identified 182 samples as HER2-positive and 1,505 as HER2-negative. Among the 1,695 samples included in this study, 8 samples were withdrawn either for incompatibility with the inclusion criteria (6 samples, 0.35%) or for non-evaluable sample testing results (2 samples, 0.12%; Fig. 2).
The primary efficacy evaluation included 1,687 samples subjected to tumor sample testing, among which 182 samples were found to be HER-2 positive. The HER2 positivity rate was therefore 10.8%, with a 95% CI of 9.3% to 12.3%.
Among the 1,687 cases with assessed samples, the mean patient age was 61.9 years, with a wide age range of 24 to 95 years, and the study group comprised 69.5% and 30.5% male and female subjects, respectively. The most common tumor stage was stage 3 (45.5%), followed by stage 2 (32.6%), stage 1 (15.6%), and stage 4 (6.3%). The stomach was the tumor location in most cases (99.0%), and the most dominant tumor type was diffused (46.2%), followed by intestinal (36.8%) and mixed (11.4%). Most samples collected were collected via excision (97.3%), and all were fixed in 10% neutral buffered formalin (Table 2).
Table 2
Correlations of HER2 status with patient information and characteristics
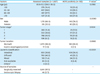
Values are presented as mean±standard deviation (range) or number (%). The sum of the percentages does not equal 100% because of rounding.
HER2 = human epidermal growth factor receptor 2.
*Indeterminate in two subjects; lymphoid stroma in one subject; mucinous adenocarcinoma in one subject. †Classification according to the the Union for International Cancer Control/American Joint Committee on Cancer 7th edition.
Regarding tumor, node, metastasis (TNM) classification by tumor stage, all 263 samples diagnosed as stage 1 were T stage 2, with infiltration limited to the muscle layer, whereas 393 (71.5%) of 550 samples diagnosed as tumor stage 2 were T stage 3 or 4a. Among 768 samples diagnosed as tumor stage 3, T4N3M0 was most prevalent (264 samples, 34.4%), followed by T3N3M0 (143 samples, 18.6%), T3N2M0 (139 samples, 18.1%), and T4aN2M0 (102 samples, 13.3%). All 106 samples diagnosed as tumor stage 4 were M stage 1 (metastatic).
Automated methods were used for IHC testing and re-testing, and SISH was used for all ISH confirmation testing. The Ventana CONFIRM HER2/neu (4B5) Antibody System (Roche Tissue Diagnostics/Ventana) was used most frequently (777 samples, 46.0%), followed by the Anti-HER2 (A0485) Antibody or HercepTest (Dako; 607 samples, 36.0%) and others (303 samples, 18.0%). All 198 IHC re-tests were performed using the Ventana CONFIRM HER2/neu (4B5) Antibody System (Roche Tissue Diagnostics/Ventana). Ventana INFORM HER2 DNA dual-color assay (Roche Tissue Diagnostics/Ventana; SISH) was used for all 64 samples subjected to ISH. For the secondary efficacy evaluation, correlations of HER2 status with stage, tumor type, gastric vs. GE junction cancer, age, and sex were assessed. Regarding tumor type, the HER2 positivity rates were 17.6%, 12.4%, and 5.3% for the for intestinal, mixed, and diffused tumor types, respectively. These differences in HER2 positivity rates were significant (P<0.0001). Regarding sex, male and female subjects had HER2 positivity rates of 12.1% and 7.8%, respectively, which showed a significant difference (P=0.0080). Regarding the correlation of HER2 status with sex, this significant difference in HER2 positivity did not exhibit a consistent tendency (P=0.0185). Furthermore, significant differences were not observed among tumor stages (stage 1–4, P=0.1554; Table 2).
DISCUSSION
This study examined HER overexpression in 1,695 patients with gastric and GE junction cancer using samples from 14 different hospitals. HER2 positivity was defined as IHC 3+ or IHC 2+ plus SISH+. Regarding the primary study objective, the HER2-positive rate was 10.8% based on data from 14 local laboratories, and slightly lower than the rates reported by other studies [91011]. Moreover, this rate was much lower than the rate reported by the ToGA trial (IHC 3+ or IHC 2+/FISH+; 16.0%) [5]. Regarding the secondary objectives, the HER2-positive rate was significantly higher in intestinal type tumors (Lauren classification), compared to diffuse/mixed type tumors (17.6% vs. 5.3%/12.4%; P<0.0001), which corroborated the findings of other studies, including the ToGA trial. However, the HER2-positive rate of GE junction cancers was not higher than that of GCs in the present study. Furthermore, HER2 positivity did not correlate significantly with disease stage.
HER2 has increasingly become an important biomarker of gastric and GE junction cancers. Current estimations suggest approximately 16% of gastric and GE junction tumors overexpress HER2, although the precise figure remains uncertain with reported frequencies of HER2-positive GC ranging from 6.0% to 30.0% [678910].
Various HER2 positivity rates have been reported for Korean patients with GC; studies have published rates of 3.4% (8/232), 6.0% (11/182), and 4.0% (10/248) using the IHC 3+ criterion and of 6.5% (15/230), 3.8% (7/182), and 7.7% (19/248) using ISH [61213]. Although HER2 positivity appears to vary by IHC and ISH type (chromogenic ISH [CISH], FISH, or SISH), the authors have similarly noted that the frequency of HER2 mutation appears to be lower among GC, compared to breast cancer, and recommend discussion and validation as necessary for consistency among studies.
We believe that at least three important points regarding differences in HER2 positivity among studies should be considered. First, inter-study variability can largely be attributed to differences in the definition of HER2-positive GC. The authors of the ToGA study used a modified HER2-scoring system based on a protocol for breast cancer, which defined an IHC score of 3+ and/or FISH positivity, leading to an overall HER2-positive rate of 22.1%. However, the frequency of HER2-positive GC defined as IHC 3+ or IHC 2+/FISH+, after excluding FISH+ IHC 0/1 samples, was 16.0% [45].
Compared to IHC 3+, the criterion of ISH positivity tends to yield a slightly higher rate of HER2 positivity in GC. IHC-based studies have reported a wide range of HER2 positivity rates in GC (8.2%–32.0%) [7, 8, 1415161718]. FISH-based studies have reported a similarly wide range (7.1%–43%) [79192021]. Notably, most previously reported data were generated without applying a modified scoring system for GC and must be interpreted with caution. The present study followed the EMA criteria for HER2 positivity and obtained a rate of 10.8%. Second, inter-observer and inter-institutional variability might also explain differences in HER2 positivity, as different pathologists at each institute use different assays, definitions of HER2 positivity, and scoring systems. HER2 staining results seem to be influenced by a number of factors, including fixative type, staining method, and pathologist's experience level [2223]. However, these inter-observer differences may not be highly influential. In the Chinese HER-EAGLE study, a comparison revealed good concordance regarding HER2 status, with a total agreement rate between local and central laboratories of 97.2% (kappa=0.86) [11]. In addition, several IHC kits are currently available in Korea. Various antibody methods are still used, although only two have been approved by the Food and Drug Administration (HercepTest and Ventana), and all cases were included in the present study. Accordingly, the present study subjected IHC 2+ samples from the 14 participating hospitals to an IHC re-testing step conducted at 3 central laboratories. Third, differences in population characteristics among studies may have contributed to the different outcomes. Per previous reports, HER2 positivity rates tend to be higher among GE junction cancers vs. GCs and among intestinal type vs. diffuse/mixed type cancers. Our study population included a lower proportion of intestinal type cases relative to diffuse/mixed type cases (36.8% vs. 46.5%/11.4%). In contrast, the ToGA trial enrolled more intestinal type cases relative to diffuse/mixed type cases (52.0% vs. 30.3%/17.6%) [4]. These two studies, however, observed similar patterns in HER2 positivity rates among subtypes (intestinal vs. diffuse/mixed, 32.3% vs. 6.1%/20.4% in ToGA and 17.6% vs. 5.3%/12.4% in the present study). Moreover, the proportion of GE junction cases was extremely small in our study, compared to that in the ToGA study (1.0% vs. 18.1%). Our study also reported a higher HER2 positivity rate among GE junction tumors. Their effects did not contribute to HER2 incidence, in comparison to the ToGA study. These factors could potentially explain our lower HER2 positivity rate.
In contrast to breast cancer findings, the ToGA trial reported similar frequencies of FISH positivity among IHC 0/1 and IHC 2 samples (23% vs. 26%). However, in a ToGA study ad-hoc analysis, patients with HER2 IHC 2+/FISH positive or IHC 3+ gastric and GE junction cancer achieved the greatest overall survival benefits when compared to patients with IHC 0/1/FISH positive disease.
In Korea, the national health insurance system does not cover expenses associated with FISH/SISH for all GC patients. Hence, IHC-based HER2 status assessment and subsequent FISH/SISH, if indicated, is more a cost-effective and acceptable clinical practice in a clinical setting.
In conclusion, this was the first epidemiologic study of the HER2 positivity rate in gastric and GE junction cancers among patients in a Korean multicenter community-based setting. Using a modified scoring system and settings more similar to actual clinical scenarios, the HER2 positivity rate among GC and GE junction adenocarcinomas was 10.8% according to assessments by local laboratories at participating centers. Our findings demonstrate the crucial role of epidemiological data in studies of HER2 expression rates in GCs and GE junction adenocarcinomas.
 XML Download
XML Download