

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary artery vasospasm (CVS) is a transient and reversible vasoconstriction of the major epicardial coronary artery evoking myocardial ischemia (Figure 1). The concept of CVS has been a stimulus to look at coronary artery disease (CAD) as a much more varied and dynamic process than the static and rather stable picture. In 1959, Prinzmetal et al.1) first described characteristic clinical features of patients with ‘variant angina’ which could not be explained by significant fixed stenosis of the major epicardial coronary artery resulting in development of classic effort-related angina pectoris. These features include 1) development of chest pain not associated with increased myocardial oxygen requirement such as exercise or emotional excitement, 2) resting chest pain with typical diurnal variation with frequent attack at night or early morning, 3) marked ST-segment elevation in the electrocardiogram (ECG), and 4) prompt response to sublingual application of nitroglycerin.1) More than 10 years later, CVS was proved to be a mechanism of variant angina2) and became a hot topic or keyword in the 1980s representing that CVS has been well accepted part of the spectrum of CAD.3) Spasm provocation testing has been successfully introduced in the cardiac catheterization laboratory to evaluate the full spectrum of CAD4)5)6)7) and the term CVS was often used too liberally to describe any form of constriction of epicardial coronary artery. Further clinical investigations confirmed that CVS is a contributor to the development of effort-induced angina, acute coronary syndrome and sudden cardiac death, covering wide clinical spectrum of CAD. However, we have witnessed in the last 20 years that clinicians' interest in the CVS has decreased significantly8)9)10) and spasm provocation testing is not listed or officially recommended any more in the recent American clinical guideline.11)12) Compared to the western countries, clinical incidence of variant angina in Korea and Japan seems to be higher and role of spasm provocation testing for definite diagnosis of CVS needs to be reevaluated for appropriate education of a new generation of cardiologists.
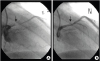 | Figure 1A representative case of coronary artery vasospasm documented by pharmacologic spasm provocation test during invasive coronary angiography: focal vasoconstriction (arrow, A) resulting in total occlusion of proximal left anterior descending coronary artery developed with ergonovine injection (E2, A), which was normalized with nitroglycerin administration (N, B).
|
PATHOPHYSIOLOGY OF VARIANT ANGINA DUE TO CVS
The most important characteristic clinical feature of variant angina due to CVS is that development of chest pain is not associated or parallel with increase of myocardial oxygen demand (Table 1). In normal condition, the diameter of major epicardial coronary arteries changes continuously to maintain adequate oxygen delivery to the myocardial tissue. Coronary flow reserve defined as the ratio between blood flow at the maximum coronary vasodilation and is higher than 4 at normal condition. As the local blood flow parallels the biquadrate of the diameter of the feeding vessel, maintaining the normal coronary artery diameter is critical for normal myocardial perfusion. In patients with classic angina pectoris, diameter narrowing due to atherosclerosis results in significant reduction of coronary flow reserve. Thus, at resting status, sufficient myocardial perfusion may be possible; however, during exercise or emotional stress requiring adequate increase of cardiac output and myocardial oxygen demand, progressive coronary vasodilatation is limited due to fixed stenosis resulting in development of myocardial ischemia or chest pain. In typical angina, we can assume a fixed level of angina threshold and, if routine activity exceeds the angina threshold, development of myocardial ischemia or chest pain is easily expected (Figure 2A). Routine daily activities not exceeding the angina threshold do not cause myocardial ischemia or chest pain development. Thus, as myocardial oxygen demand usually parallels with heart rate, chest pain development due to classic angina pectoris usually aggregates in the daytime coinciding with the changes of the heart rate. On the other hand, variant angina is characterized by varying angina threshold in a day and myocardial ischemia or chest pain can develop irrespective of myocardial oxygen demand associated with routine activities (Figure 2B). The angina threshold in variant angina shows a typical diurnal variant with significantly lower level during nocturnal time or sleep when the heart rate usually shows lower level. Accordingly, variant angina is characterized by its circadian variation of development of chest pain or myocardial ischemia and there is no association between the heart rate and the frequency of chest pain due to variant angina.
Table 1
Comparison of clinical features between classic angina pectoris and variant angina

![]()
 | Figure 2Schematic illustrations showing relationship between angina threshold (dotted line) and daily activity in classic effort angina (A) and variant angina (B). In classic effort angina with fixed angina threshold, daily activity exceeding the angina threshold results in chest pain attack (blue), which is quite predictable and usually develops during daytime paralleling with the level of physical activity. However, in variant angina, the angina threshold itself varies significantly during a day and the level of physical activity is not associated with chest pain attack: thus, chest pain attack is quite unpredictable depending on the change of angina threshold, not on the level of physical activity (orange) (modified from reference 3).METS = metabolic equivalents.
|
CLINICAL FEATURES OF CVS
Variant angina is a typical clinical presentation of CVS and chest pain is not associated with exercise or effort in daytime: angina pain associated with spontaneous spasm usually develops during sleep or early in the morning (Figure 3). In some patients, chest pain development is associated with alcohol drinking and one interesting point is that angina attack develops several hours later after alcohol intake, rather than immediately after drinking. Thus, many patients may be misdiagnosed to have gastrointestinal problems including peptic ulcer disease or esophageal reflux disease. Although resting chest pain is a usual clinical presentation of variant angina, in some patients of variant angina, development of chest pain is associated with minimal effort such as walking in the morning; these patients do not develop chest pain with more demanding exercise such as running in the daytime. This discrepancy between work loading and angina development represents typical diurnal or circadian variation of angina threshold in variant angina. Meticulous history taking to assess characteristic circadian variation of angina attack is important for correct diagnosis of variant angina.
 | Figure 3A representative Holter monitoring in a patient with spontaneous coronary vasospasm. Characteristic ST-segment elevation at early morning with rapid progression to ventricular tachyarrhythmia is well demonstrated.
|
Variant angina is the most frequent clinical presentation of CVS, but, not infrequently, patients with CVS show different presentations (Figure 4). Acute coronary syndrome is one example of diverse clinical presentations of CVS. Figure 4A is a typical ECG showing deep T wave inversion in the precordial leads in a 40-year old man who visited emergency department due to sudden chest pain. He was admitted to the coronary care unit under the impression of acute coronary syndrome and underwent invasive coronary angiography. The angiogram showed completely normal epicardial coronary arteries and spasm provocation testing performed several days later showed CVS in the left anterior descending artery. Figure 4B is an ECG recorded in the emergency department in a 56-year old man with prolonged chest pain. Marked ST-segment elevation suggesting the diagnosis of ST elevation myocardial infarction prompted an emergent coronary angiography, which revealed no evidence of plaque rupture or significant stenosis in the coronary arteries. He showed CVS in the left anterior descending coronary artery in spasm provocation testing. Sudden cardiac death is another clinical presentation of CVS. Figure 4C shows ventricular fibrillation in the ECG monitoring of 47-year old man who suffered from aborted sudden cardiac death. Coronary angiography was normal and echocardiography showed no significant pathology including hypertrophic cardiomyopathy. Several weeks later after the first event of aborted sudden cardiac death, chest pain developed and ECG at that time showed characteristic ST-segment elevation, which is compatible with variant angina due to CVS. In typical patients with variant angina, coronary flow reserve is within normal range and thus development of chest pain or myocardial ischemia is not associated with exercise. However, in rare cases, patients with CVS may present with effort-related angina with typical ST-segment depression in the treadmill test. ST-segment depression usually develops at the late stage of the exercise and typically persists during recovery (Figure 4E) and persistent ST-segment depression during recovery is believed to be partly associated with hyperventilation, which is an accepted spasm provocative method.
 | Figure 4Representative electrocardiograms showing various clinical presentations of patients with coronary artery vasospasm: acute coronary syndrome with deep T wave inversion in the precordial leads (A), prominent ST-segment elevation mimicking ST elevation myocardial infarction (B), development of ventricular fibrillation and ST elevation in aborted sudden cardiac death (C, D), and ST-segment depression during exercise treadmill test in a patient with effort-induced chest pain (E).
|
The most challenging clinical condition is development of CVS in patients who previously underwent coronary intervention (Figure 5): Figure 5A is a coronary angiogram of 46-year old female presented with unstable angina. Coronary stenting was successfully done in the middle portion of the left anterior descending artery (Figure 5B), but in-stent restenosis developed several months later (Figure 5C). Cutting balloon angioplasty and local radiotherapy was done for this lesion (Figure 5D). Unfortunately, chest pain re-developed and follow-up angiography showed development of tight stenosis (Figure 5E), which needed the second stenting at the proximal left anterior descending artery (Figure 5F). Six months later, she developed early morning minimal effort-related chest pain and follow-up angiogram showed no significant interval change (Figure 5F) with negative treadmill exercise test up to 12 metabolic equivalents. Non-invasive spasm provocation testing showed reversible wall motion abnormality in the left anterior descending artery territory with ergonovine injection; the patient condition stabilized with administration of calcium-channel blockers. These cases reinforce clinical importance of physicians' recognition that clinical presentations of CVS are quite diverse and variable. Thus, if patients with chest pain, ECG abnormality, or sudden cardiac death may show normal coronary angiograms, the possibility of myocardial ischemia due to CVS should be included as differential diagnosis. This approach has important prognostic implication especially in Korea with relatively higher prevalence of CVS compared with the western countries.

DIAGNOSIS
As described above, meticulous history taking to find evidences supporting characteristic circadian or diurnal variation of angina threshold is mandatory for accurate diagnosis of CVS. In patients with stable condition, clinical observation period to determine the efficacy of sublingual application of nitroglycerin at the time of chest pain can be a useful screening to determine the next diagnostic step. Patients with clinical presentation of sudden cardiac death or acute myocardial infarction usually do not need this screening period.
The first diagnostic step is to rule out significant fixed stenosis of the major epicardial coronary artery using either treadmill exercise ECG, non-invasive computed tomography (CT) or invasive coronary angiography.10)13) The next step is Holter monitoring to detect ECG changes associated with spontaneous CVS (Figure 3). If a spontaneous episode of rest angina is associated with transient ischemic ECG changes including typical ST elevation and there is no other cause identified for the ECG changes, then CVS is presumed to be responsible and a definite diagnosis of variant angina may be made without formal documentation of CVS: recording of typical ST-segment elevation is helpful for diagnosis of CVS, especially when it occurs during sleep or early morning with minimal increase of heart rate. However, as CVS development is episodic, false negative result is frequently expected.
Given the transience of CVS, correct diagnosis of CVS usually requires more sophisticated provocative diagnostic approaches.8)10)13) For spasm provocation test, physiologic stimulation including hyperventilation or cold exposure once has been suggested, but the diagnostic sensitivity of these maneuvers is reported to be low and pharmacologic stimulation is usually preferred.14)15) The 2 most widely being used pharmacological agents for spasm provocation testing are ergonovine and acetylcholine (Table 2). Ergonovine is amine alcohol derivative of the lysergic acid and acts on smooth muscle mainly via activation of serotonergic receptors to produce vasoconstriction. It is a gold standard agent for spasm provocation test and its sensitivity and specificity for diagnosis CVS has been reported to be higher than 90%.16) Either intravenous or intracoronary administration of ergonovine is possible for spasm provocation. As ergonovine can cause progressive increase of blood pressure with vasoconstriction of peripheral vessels, uncontrolled systemic hypertension is contraindication of spasm provocation testing using intravenous administration of this drug. Acetylcholine is clinically introduced by Japanese investigators for spasm provocation testing. As this drug is rapidly metabolized by cholinesterase, which is abundant in the human plasma, systemic administration is impossible and only intracoronary administration is being used. Due to its very rapid metabolism, using intracoronary acetylcholine is expected to be useful for selective and consecutive intracoronary administration allowing provocation of the right and left coronaries separately. Adverse reactions to acetylcholine include hypotension, bradycardia, dyspnea, ventricular tachycardia, and shock: as this drug can cause bronchospasm, bronchial asthma is a contraindication of spasm provocation testing using this drug.
Table 2
Comparison of pharmacological agents (ergonovine vs. acetylcholine) used for spasm provocation test

![]()
Before spasm provocation testing, drugs potentially affecting coronary vascular tone should be discontinued sufficiently. Calcium-channel blockers, beta-receptor blockers and nitrates are typical examples requiring discontinuation and these drugs should be discontinued for at least 3 or 4 days. For adequate control of systemic hypertension, angiotensin converting enzyme inhibitors or angiotensin receptor blockers are generally used. Invasive provocation testing involves the administration of a provocative stimulus (typically intracoronary acetylcholine but alternatively intracoronary or intravenous ergonovine may be used) during invasive coronary angiography with the monitoring of patient symptoms, ECG, and angiographic documentation of CVS. Usually, temporary pacemaker back-up is being used. A positive provocative test for CVS must include all of the following in response to the provocative stimulus: 1) reproduction of the usual chest pain, 2) ischemic ECG changes (ST elevation, ST depression and U wave changes), and 3) >90% vasoconstriction on angiography.8)13) The test considered equivocal if the provocative stimulus does not induce all three components. According to the recently published multi-center registry study from Japan, the overall incidence of arrhythmic complications was 6.8% and ventricular tachycardia or fibrillation and brady-arrhythmias developed at a rate of 3.2% and 2.7% without any mortality.17)
Non-invasive provocation testing with systemic administration of ergonovine and continuous monitoring of ventricular wall motion abnormality (ergonovine echocardiography) can be performed in patients without significant fixed stenosis.18)19)20)21) Development of refractory CVS during ergonovine provocation test resulting in mortality was reported in early 1980s22) and intracoronary administration of nitroglycerin has been accepted as a mandatory condition for spasm provocation testing. Thus, non-invasive spasm provocation testing has not been accepted as a safe and reliable test. The prejudice against non-invasive spasm provocation testing has been provoked by a few clinical observational studies using ECG only as an objective sign of myocardial ischemia. As CVS is defined as reversible coronary vasoconstriction evoking myocardial ischemia, objective signs of myocardial ischemia at the time of luminal constriction should be demonstrated for correct diagnosis of CVS.9) Although, in Prinzmetal's original description, ST elevation was described as a hallmark of CVS, ischemic ECG changes even including ST depression and U wave changes are not sensitive enough for diagnosis of myocardial ischemia,23) which seems to definitely contribute to late diagnosis of CVS resulting in mortality. Development of regional wall motion abnormality is an early sign of myocardial ischemia and it is sobering to note that the relatively high incidence of negative or inconclusive ECG changes at the time clear transient new ventricular wall motion abnormalities are provoked. In addition to increase of diagnostic power, the advantage of using echocardiographic monitoring of regional wall motion abnormality include safety issue: as early and reliable diagnosis of CVS based on development of regional wall motion abnormality is possible, termination of CVS or spasm provocation testing can be done much earlier, which may guarantee safety of the test. This is well translated to no mortality and lower incidence of arrhythmias (<1%) during ergonovine echocardiography.19) Comparison of potential advantages and disadvantages of ergonovine echocardiography and invasive spasm provocation test during angiography are summarized in Table 3. It should be reminded that both methods require physicians' expertise and skill for both accurate and safe diagnosis of CVS.
Table 3
Comparison of potential advantages and disadvantages of ergonovine echocardiography versus invasive spasm provocation test during angiography (reproduced with permission from reference 19)

![]()
TREATMENT
As myocardial ischemia induced by CVS can result in fatal sudden death or acute myocardial infarction, strict medication to control CVS is warranted. Contrary to classic effort angina, β-receptor blockers are generally contraindicated for patients with CVS as these drugs can cause adverse increase of vascular tone. The successful clinical introduction of calcium-channel blockers has contributed to improve clinical outcomes of patients with variant angina and prescription of these drugs has become the most important therapeutic strategy.24) Nitrates are generally recommended, but, in patients with CVS superimposed on near normal coronary angiogram, routine prescription of aspirin or lipid-lowering agent is not routinely done. One important issue is to keep medication time to match the characteristic circadian or diurnal variation of CVS attack: if routine medication is administered early evening after the dinner, patients may suffer from repeated episodes of chest pain attack due to CVS at early morning or mid-night, when the drugs cannot maintain their effective drug blood level. Thus, it is better to take medication before sleep, not soon after the meal. In addition, preparation of sublingual nitroglycerin at bedside is strongly recommended for effective and prompt relief of chest pain attack during sleep or at early morning.
In most patients with variant angina, treatment of both calcium-channel blockers and nitrates is very effective to prevent myocardial ischemia due to CVS, but, in rare circumstances, chest pain becomes intractable. In this case, addition of calcium channel blockers with different classes is effective. There are several different classes of the calcium channel blocker and dihydropyridine calcium channel blocker is the most popular one. Drugs in this class can be easily identified by the suffix “-dipine”: amlodipine, nifedipine and felodipine are classic examples of this class. Non-dihydropyridine classes include phenylalkylamine, benzothiazepine and other non-selective drugs. Verapamil is the representative of phenylalkylamine calcium channel blockers and diltiazem is that of benzothiazepine calcium channel blockers. In patients with intractable chest pain attack despite use of one calcium channel blocker, addition of different class of calcium channel blockers is effective. In rare cases, use of 3 different classes of calcium channel blocker is necessary to prevent chest pain attack.
The most serious clinical presentation of CVS is aborted sudden cardiac death and prognosis of patients with this unique presentation is reported to be poor.25) In addition to the medication, several clinical studies recommend insertion of implantable cardioveter defibrillator in these patients. The timing of implantation of this device needs to be clarified by future investigations.
CONCLUSIONS
CVS can produce any of the manifestations of CAD from silent myocardial ischemia, to effort-induced angina, variant angina, and unstable angina, to myocardial infarction or sudden death. Its clinical significance should be appropriately appreciated by the physicians for patient safety. Although there are no evidences supporting that the incidence of CVS is declining these days, provocative tests for CVS are now done much less frequently in the U.S. and Europe than in former years and reliable spasm provocation agents (both ergonovine and acetylcholine) are not U.S. Food and Drug Administration-approved for the indication of CVS diagnosis; moreover, spasm provocation test is not included or addressed in the recently published American College of Cardiology (ACC)/American Heart Association (AHA) clinical guidelines.11)12) Thus, a new generation of invasive cardiologists is being trained which has little or no experience in doing such test, and hence has little comfort when faced with doing them.9) Bedside ergonovine provocation testing with echocardiography monitoring has been reported to replace invasive provocation test, but larger studies are needed to generate evidence-based guidelines with regard to the effectiveness and safety of spasm provocation testing for diagnosis of CVS.
 XML Download
XML Download