

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Currently, the first treatment of choice for ankle osteoarthritis is conservative treatment. For end-stage ankle osteoarthritis that does not respond to conservative treatment, there are several surgical options with ankle arthrodesis being the most prevalent treatment.1)
More than 40 different treatment methods for ankle arthrodesis have been introduced, including open ankle fusion, arthroscopic ankle fusion, and ankle fusion using mini-open ankle arthrodesis.2) Also, there are various approaches used in ankle arthrodesis, and the most widely used approaches include the anterior approach and the transfibular approach. Previous studies have reported a similar rate of fusion for each approach, but the incidence of complications varies among studies.3) However, there have been only a few reports comparing the anterior and transfibular approaches. In this study, we set out to compare the two approaches under the hypothesis that the fusion rate of the transfibular approach would be higher than that of the anterior approach because of the additional stability with autogenous bone grafting or onlay graft using a distal fibula in the transfibular approach. We evaluated and compared the clinical and radiological results of ankle arthrodesis performed with the anterior and transfibular approaches.
METHODS
From January 1, 2005 to January 1, 2015, sixty patients with ankle osteoarthritis treated using an anterior approach or a transfibular approach were included in this study. The approach was selected randomly and compared retrospectively. We conducted this study in compliance with the principles of the Declaration of Helsinki. This study was reviewed and approved by the Institutional Review Board of Inje University Busan Paik Hosipital (IRB No. 18-0154). Written informed consents were obtained. Of the total 60 patients, we used the anterior approach in 38 patients (anterior approach group) and the transfibular approach in 22 patients (transfibular approach group). Demographic data was not different between the anterior approach group and the transfibular approach group (Table 1).
The American Orthopedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot score and visual analogue scale (VAS) score were assessed for clinical evaluation. The AOFAS score is 100 points in total, but the maximal score in patients who underwent ankle fusion was 86 points because the movement of ankle joint was eliminated.
Before and after surgery, the degree of valgus/varus angulation was assessed by the angle between the long axis of the tibia and the long axis of the calcaneus on the hindfoot alignment view.4) The axis of calcaneus was measured using the method suggested by Robinson et al.5) (Fig. 1). Fusion was confirmed radiographically by observing the trabecular lines and loss of radiolucent area between the tibia and talus once every month.2) All radiological evaluations were performed by two orthopedic surgeons (HCG and JGK) using the Picture Archiving and Communication System (PACS) (Maroview, Marotech, Seoul, Korea).
Surgical Technique
Under general anesthesia or spinal anesthesia, a thigh tourniquet was applied. In the anterior approach group, the ankle joint was exposed after a skin incision of approximately 10 cm in front of the ankle joint. Subsequently, the cartilage tissue was removed from the joint surface of the tibia and talus using a burr. With an oscillating saw, an osteotomy was performed to expose the subchondral bone. The ankle joint was fixed with two cannulated screws (7.0 mm) forming an angle of 45° with the tibial axis in a neutral ankle joint position, 5° valgus, and 5° external rotation (Fig. 2).
In the transfibular approach group, a lateral incision, including the distal part of the fibula, was performed with a 10 cm skin incision. Then, an osteotomy with a saw was performed to the distal fibula, and the ankle joint was exposed without an additional medial approach. Thereafter, the cartilage was removed using an osteotomy and a burr on the tibia and the talus, and the subchondral bone was then exposed. A cannulated screw (7.0 mm) was inserted toward the talus body at a 45° angle with the long axis of the tibia, and another screw was inserted toward the tibia at an angle of 45° with the long axis of the tibia. We performed onlay bone graft using the fibular fragment obtained in the osteotomy for exposing the ankle joint, and the fibular bone was fixed with two 3.5-mm cortical screws (Fig. 3A–D). In the case of a large bone defect, a strut bone graft was performed with the distal part of the fibular bone obtained by osteotomy. In both approaches, after skin suture, short leg splinting was performed. On the 3rd postoperative day, non-weight bearing 3-point crutch ambulation was initiated with ankle boots worn to start range of motion at the adjacent joint. Sutures were removed 2 weeks postoperatively. Postoperative rehabilitation was the same in both groups. Partial and tolerable weight bearing was applied 6 weeks postoperatively, and full weight-bearing ambulation was initiated upon confirmation of radiographic union.
Statistics
AOFAS scores and subjective satisfaction were analyzed using the Mann-Whitney U-test. VAS scores were analyzed using independent t-test. The fusion rate between the two groups was analyzed by Fisher exact test. All analyses were performed with IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA).
RESULTS
In the anterior approach group, the mean VAS score was improved from 5.18 (range, 4 to 8) preoperatively to 1.46 (range, 0 to 3) postoperatively, and the mean AOFAS score was improved from 39.8 (range, 29 to 56) preoperatively to 58.3 (range, 46 to 86) postoperatively. In the transfibular approach group, the mean VAS score was improved from 4.87 (range, 4 to 7) preoperatively to 1.27 (range, 0 to 3) postoperatively, and the mean AOFAS score was improved from 44.5 (range, 32 to 60) preoperatively to 60.7 (range, 48 to 86) postoperatively. However, there was no significant difference between the two groups in VAS and AOFAS scores at the last follow-up (p = 0.436 and p = 0.274).
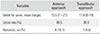
In the anterior approach group, the mean time to bone union was 13.5 weeks (range, 11 to 21 weeks). In the transfibular approach group, the mean time to bone union was 11.8 weeks (range, 9 to 18 weeks). There was no statistically significant difference in the time to bone union between the two groups (p = 0.148) (Figs. 2E and 3E).
The mean hindfoot alignment was 0.7° varus in the anterior approach group and 2.4° valgus in the transfibular approach group at the last follow-up. There was a statistically significant difference in the postoperative alignment between the groups (p = 0.05).
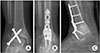
There were four cases of nonunion in the anterior approach group, including one case of osteomyelitis with nonunion; one case of nonunion occurred in the transfibular approach group. There was no statistically significant difference in the union rate between the two groups (p = 0.400) (Table 2). Revision ankle arthrodesis was performed with the transfibular approach or the anterior approach using cannulated screws for nonunion cases in the anterior approach group (Fig. 4), whereas a fusion plate was used for the nonunion case in the transfibular approach group (Fig. 5).
DISCUSSION
The most commonly used surgical method for end-stage osteoarthritis of the ankle is open ankle fusion performed widely with an anterior approach or a transfibular approach. 6)
An ankle fusion using the anterior approach has the advantage that the ankle joint is completely exposed and the joint deformity is easy to correct. The disadvantage is that the superficial peroneal nerve, which is located in the anterior aspect of the ankle joint and the anterior tibial neurovascular structure, is more likely to be injured.7)
Because the soft tissue is thicker on the lateral side than on the anterior side, complications such as wound infection, dehiscence, and delayed healing are less common in the transfibular approach than in the anterior approach. In addition, the transfibular approach is advantageous for correction of deformity because the subtalar joint and sinus tarsi as well as the ankle joint are exposed. It allows not only easy correction of deformities such as ankylosis but also results in minimal shortening, wide contact area, and high stability.8910) Furthermore, an ankle joint fusion using an open, transfibular approach has been reported to provide a fusion rate of 90% or more without bone graft.9) It is also possible to perform autologous bone graft or onlay graft using a distal fibula, which is thought to provide more stability,11) and to reduce nonunion with the transfibular approach.7) However, transfibular arthrodesis requires additional osteosynthesis of the lateral fibula.2)
There are many ways to fix the joints, and they are classified into internal fixation and external fixation.1213) Internal fixation with a compression screw is most widely used in ankle arthrodesis.14) Internal fixation can be done by a compression technique using a cannulated screw or a cancellous bone screw.15) Cannulated screws in ankle arthrodesis are more resistant to bending than cancellous screws. Cannulated screws can be easily inserted using a guide pin under real-time radiographic guidance and can be fixed accurately and easily at a desired position.16)
In an earlier study, fusion rates in the open surgery group with internal fixation were reported to be between 77% and 100%.17) In 1991, Holt et al.18) suggested the standard technique of the transfibular approach with fibular onlay graft and reported a 93% rate of union in a low-risk group for nonunion. Besides, in a high-risk group for nonunion, they reported a 62% nonunion rate. Monroe et al.19) reported a 93% rate of union in a high-risk group for nonunion, with an average duration of 9 weeks for union.
In previous studies of the anterior approach, Holt et al.18) demonstrated a 74% union rate and reported a 93% fusion rate when patients high-risk for union were excluded. In another study, Gordon et al.20) reported a 100% rate of union with the anterior approach.
In this study, 60 patients with osteoarthritis of the ankle joint were investigated. There was no statistical difference between the groups except for the incidence of nonunion and hindfoot alignment. There were four cases of nonunion in the anterior approach group and one case of nonunion in the transfibular approach group. Thus, we achieved a 95.4% rate of union in the transfibular approach group and an 89.5% rate of union in the anterior approach group. These findings were similar to fusion rates reported in previous studies.
On the last follow-up assessment of the hindfoot alignment, the transfibular approach group showed valgus angulation compared to the anterior approach group, and there was a statistically significant difference. In a previous study, the ideal alignment after ankle arthrodesis was suggested to be the neutral ankle position, 0°–5° of valgus angulation, with a slightly external rotation.21) Therefore, the valgus alignment of the transfibular approach group compared to the anterior approach group may indicate better clinical results.
The limitations of this study include the retrospective design and the small number of cases. In particular, the number of cases in the transfibular approach group was significantly smaller than that in the anterior approach group. In addition, the mean follow-up period was relatively short. Therefore, we think that our findings should be corroborated by further prospective studies involving more patients and a longer follow-up designed to offer more reliable clinical results of the anterior approach and the transfibular approach.
In the treatment of ankle joint osteoarthritis, the anterior approach and the transfibular approach for ankle fusion have shown comparably good results. It is considered that obtaining a firm fixation is the most important factor for successful ankle fusion regardless of the approach used. In view of this, we suggest that transfibular ankle arthrodesis be a more reliable method for ankle fusion because of additional stability with fibular onlay graft. In addition, it does not necessitate additional bone graft, and results in a favorable alignment.





 XML Download
XML Download