

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The superior labrum anterior to posterior (SLAP) lesion is an injury located within the superior labrum that extends anterior to posterior. The prevalence of SLAP lesions is approximately 6% in the patients undergoing shoulder arthroscopy.1) Many studies reported the outcome of SLAP repair using clinical tests, postoperative satisfaction, functional scores, and return to sports or work.12) Despite advancements in imaging technology and surgical techniques for arthroscopic SLAP repair, nearly one third of patients still remain unsatisfied, and significant controversy exists regarding the management of this lesion.1) Burkart et al.3) reported that isolated SLAP repair would not bring sufficient restoration of translation. Schroder et al.4) reported no clinical benefit of SLAP repair over sham surgery. In recent years, the number of surgeons doubting the need for SLAP repair and studies advising biceps tenodesis or tenotomy instead of SLAP repair is increasing.5)
Several studies reported older age, overhead throwers, heavy laborers, and use of tobacco and/or alcohol as the prognostic factors for the revision of SLAP repair and low functional scores.16) However, there is a lack of studies on the prognostic factors of anatomical healing and functional outcomes of SLAP repair and its clinical correlation with healing failure.
The objectives of the current study were (1) to assess the failure rate of anatomical healing using computed tomography arthrography (CTA) after at least 1 year following SLAP repair and investigate its correlation with clinical outcomes; (2) to compare the clinical and radiological outcomes of isolated type II SLAP repair with combined SLAP repair for Type II SLAP lesions combined with Bankart lesions; and (3) to establish the prognostic factors for anatomical and functional failures. This will be the first study that evaluates the prognostic factors for anatomical healing after SLAP repair and correlation of anatomical healing with functional outcomes.
METHODS
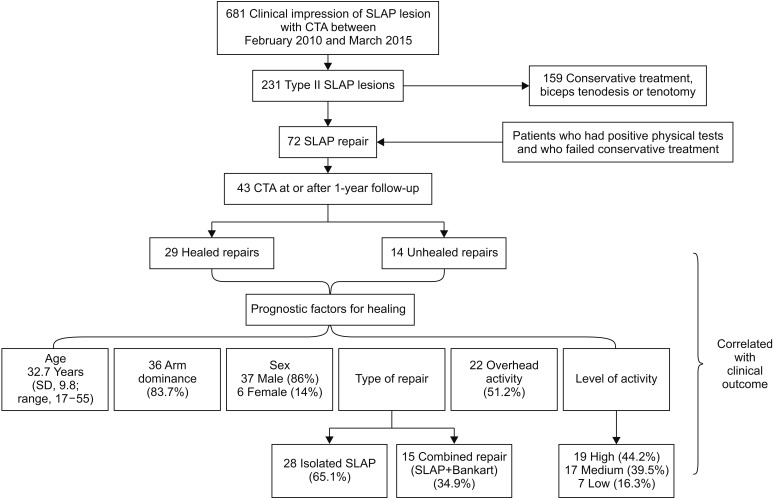
This is a retrospective level 3 evidence therapeutic study. For this type of study, formal consent is not required; verbal consent was obtained from patients for the use of their data without revealing their identity. The study was conducted at the senior author (JHO)'s institute (Seoul National University Bundang Hospital). No human rights were violated, and this study was approved by the Institutional Review Board of the Seoul National University Bundang Hospital (IRB No. B-1609/364-104). A flow diagram was created to illustrate the patient recruitment and data analysis process (Fig. 1).
Inclusion Criteria
Patients who underwent arthroscopic repair of type II SLAP lesions between February 2010 and March 2015 were reviewed. Of those, patients with the lesions evaluated by CT or MRI, confirmed by arthroscopy, and followed up for CTA assessment at 1 year after surgery were included. Preoperative assessment included comprehensive physical tests7) to identify SLAP lesions including the Speed's test, Yergason test, compression rotation test, O'Brien test, modified Jobe's apprehension and relocation test, anterior slide (Kibler) test, Whipple test, and biceps load II test.
In the case of an isolated SLAP lesion, repair was performed only on symptomatic patients with type II SLAP lesions showing positive signs,7) both arthroscopic and radiological findings of type II SLAP lesions, full range of motion, a history of failure of conservative treatment for more than 6 months, and no evidence of labral degeneration.
In the case of combined type II SLAP and Bankart lesions, the senior surgeon (JHO) repaired only symptomatic lesions in patients with positive tests for SLAP lesions and positive anterior apprehension test or load and shift test. Any asymptomatic SLAP lesions that were found incidentally in the operation were not repaired.
Intraoperatively, the senior surgeon only repaired the SLAP or Bankart lesion if following findings were additionally observed: unstable labrum that could be easily mobilized with a probe, existence of cartilage crack, and granulation or hemorrhage below the lesion.
Exclusion Criteria
Patients who underwent repair of a concomitant full-thickness rotator cuff tear, subacromial decompression, or distal clavicular resection were excluded. Patients with SLAP and Bankart lesions were excluded if humeral avulsion of the glenohumeral ligament or a bony Bankart lesion exceeding 20% of the glenoid was also observed.
Outcome Evaluation and Statistical Analysis
The level of sports participation and the level of shoulder activity during his or her normal work were graded using a 3-level scale (high, moderate, and low).8) A high level of sports participation and shoulder activity was defined as participation in dynamic or contact sports (e.g., boxing, rugby, basketball, tennis, and volleyball) or heavy manual labor (e.g., construction and manufacturing); a moderate level was defined as participation in static sports (e.g., golf, yoga, swimming, and skiing) or manual labor involving less physical activity (e.g., housework); a low level was defined as rarely engaging in sports or sedentary lifestyle.
According to the study by Eime et al.9) where 83.1% of the population involved in sports were below 35 years of age and the sports participation declined after the age of 35, we performed age subgroup analysis by dividing the patients into < 35 years of age and ≥ 35 years of age.
Patients were contacted by phone at a minimum of 2 years after surgery and asked questions about their ability to return to sports or work. Clinical failure was defined as stiffness, loss of maximum rotation, deterioration of pain and/or need for revision of surgery. Visual analogue scale (VAS) for pain and satisfaction and Constant score were assessed at the final follow-up. Muscle strength, one of the subscales of Constant score, was additionally evaluated.
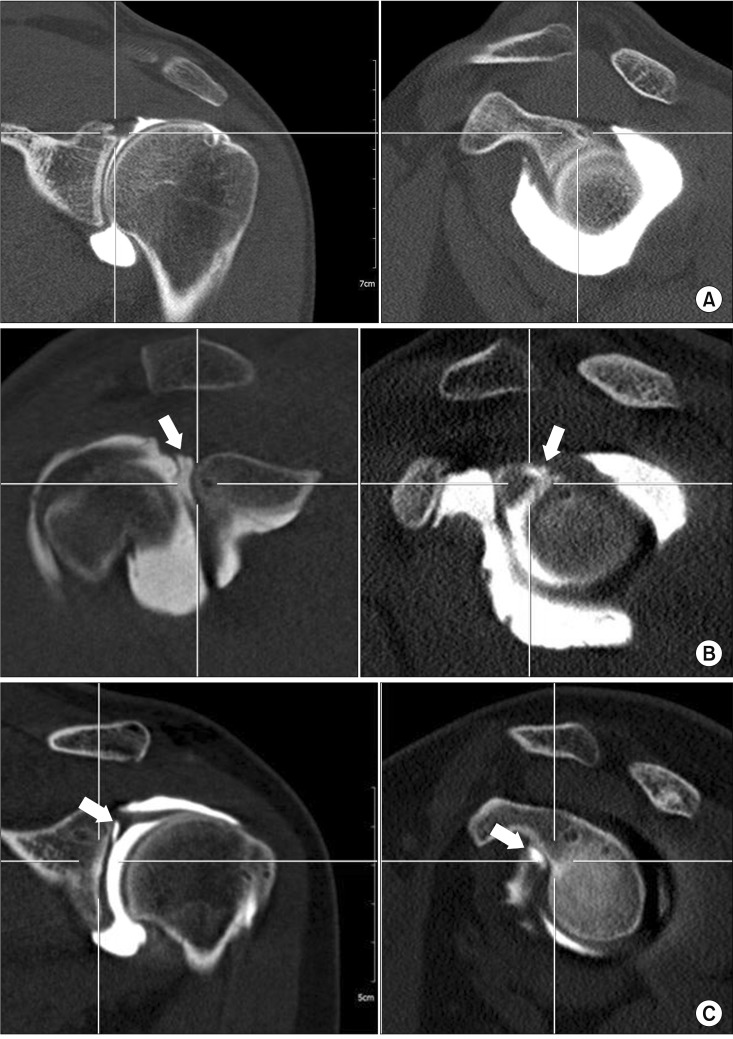
CTA was performed using a 16-multidetector CT scan system (MX8000 IDT; Philips Medical Systems, Best, the Netherlands) and 65% iodinated contrast material (Telebrix 30; Guerbet, Villepinte, France) at 1 year after surgery. CTA was chosen as an assessment tool based on a previous study that assessed failure after SLAP repair at least 1 year after surgery and on another study showing high sensitivity and specificity of CTA for failure of SLAP repair.1011) Furthermore, based on a study showing comparable diagnostic performance of CTA and magnetic resonance arthrography for labral lesions, we chose CTA due to its cost-effectiveness.12) Imaging was done in 0° of abduction with neutral rotation of the shoulder and in 90° of abduction with external rotation of the shoulder. Oblique coronal, oblique sagittal, and axial images with 2-mm thickness were generated at a three-dimensional workstation and analyzed by a musculoskeletal radiologist (JMA) with 16 years of experience at our institution. Anatomical healing of the SLAP lesion was defined as no leakage of contrast media through the biceps anchor and firm attachment of the anchor to the bony glenoid (Fig. 2A). Complete superior dye leak at 10–12 o'clock was considered anatomical failure (Fig. 2B). Dye filling beyond 12 o'clock was considered as false positive anatomical failure because it mostly could be superior labral cleft frequently seen as a postoperative change on CTA images after SLAP repair.13) Moreover, we considered dye filling beyond 12 o'clock as false positive because the senior surgeon never repairs SLAP lesions anterior to 12 o'clock as he believes that it causes external rotation stiffness and leads to inferior outcome (Fig. 2C).14)
Surgical Technique
All surgeries were performed in the lateral decubitus position. All procedures were done using anterior, posterior, and trans-rotator cuff portals. In the case of combined SLAP repair, anteroinferior capsulolabral repair was performed first, followed by SLAP repair. Subchondral bone of the superior glenoid rim was prepared as bleeding surface using a burr and a shaver to enhance healing. The posterosuperior labrum at the base of the biceps tendon was penetrated using a suture hook loaded with no. 2 polydioxanone (PDS; Ethicon, Somerville, NJ, USA) through the trans-rotator cuff portal. Then, through the anterior portal, a strand of the PDS was pulled. By using the shuttle relay technique with PDS, an open utility loop of bioabsorbable knotless suture anchors (Bioknotless; Mitek, Norwood, MA, USA) was retrieved from the transrotator cuff portal through the anterior portal. Proper tension of the utility loop and balance loop (no. 2 PDS) was critical when inserting the anchor through the transrotator cuff portal, and if the tension of both loops was adequate, the anchor was inserted into the drilled hole by capturing one strand of the closed anchor loop. Typically, two bioabsorbable knotless suture anchors (Bioknotless, Mitek) were used to fix the lesion between 10 and 12 o'clock positions (Fig. 3). Fixation beyond 12 o'clock was never performed in order to avoid postoperative stiffness.
Postoperative Rehabilitation
After an isolated SLAP repair, the shoulder was supported in neutral rotation in a brace with a pillow (Acro Assist 50A1; Ottobock, Duderstadt, Germany) for 4 weeks. Patients could remove the brace intermittently for passive shoulder exercises (forward flexion, abduction, and external rotation) in the supine position starting from the 2nd day after surgery. Active shoulder exercises were started after 4 weeks, but the attainment of full range of motion was discouraged until 2 months postoperatively. The muscle strengthening exercises were allowed after 2 months using Thera-Band (Hygenic Corp., Akron, OH, USA). Sports activity was allowed 5 to 6 months postoperatively.
In the case of combined type II SLAP and Bankart lesions, the shoulder was supported in a brace with a pillow for 6 weeks in neutral rotation. Passive motion was restricted during brace wearing, and active shoulder exercises were started after brace removal. Isometric strengthening, scapulothoracic exercises and strengthening exercises with the Thera-Band were started 3 months postoperatively. Regular sports were permitted after 6 months.
Statistical Analysis
Data regarding patient demographics, clinical outcomes, functional scores, and anatomical healing were analysed using unpaired t-test and Fisher exact test using SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA). A p-value of < 0.05 was considered statistically significant. Risk ratios and 95% confidence intervals (CIs) were calculated.
RESULTS
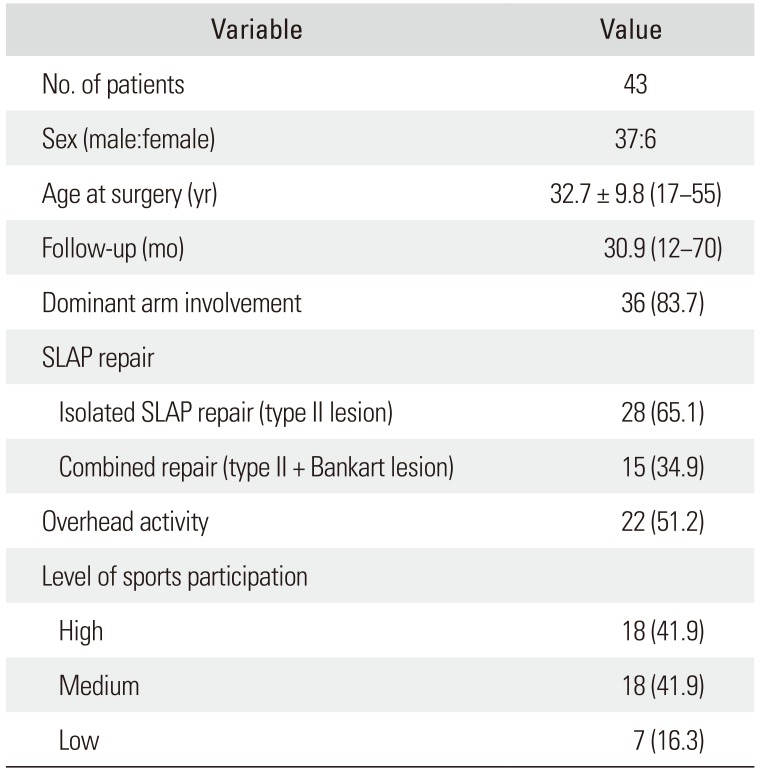
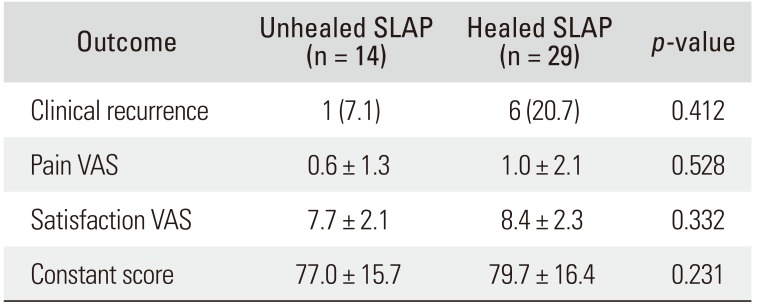
A total of 43 patients with 43 shoulders were enrolled. Their demographic data are presented in Table 1. CTA was performed at 13.4 ± 2.3 months after surgery, which revealed anatomical failure in 32.6% of patients (14/43), anatomical healing in 67.4% (29/43) of patients (no leak, 22; false positive, 7), and clinical failure in 16.3% (7/43) of patients. Clinico-radiological assessment revealed clinical failure only in 7.1% of patients (1/14) with unhealed SLAP lesions compared to 20.7% (6/29) in patients with healed SLAP lesions (p = 0.412). The mean pain VAS was 4.3 ± 2.5 preoperatively and 0.8 ± 1.8 postoperatively (p < 0.001). The mean satisfaction VAS was 8.2 ± 2.2. The mean Constant score was 62.1 ± 17.8 preoperatively and 78.8 ± 16 postoperatively (p < 0.001). Clinical outcomes were not significantly different between unhealed and healed repairs (Table 2). Regarding the muscle strength component of Constant score, patients aged below 35 years showed better strength at 90° of abduction than patients aged above 35 years (21.5 ± 2.6 vs. 18.7 ± 4.4, p = 0.050). No other difference was found regarding healing, isolated or combined SLAP repair, overhead activities (OHA), and high level of activity (HLA) (p = 0.786, p = 0.384, p = 0.436, and p = 0.740, respectively).
Two patients underwent revision surgery. Both patients had knot-induced arthropathy showing glenoid and humeral head erosion due to the impingement of the tied knot. All anchors were removed arthroscopically. One patient (no. 5) had knot protrusion at the capsulolabral repair site and the other patient (no. 33) at 7 o'clock position. Both patients had completely healed SLAP and Bankart repairs, and their functions were improved postoperatively. Remaining five patients with clinical failure (no. 8, 10, 17, 20, and 26) improved with medication, stretching exercises, and local steroid injections. One patient (no. 26) was diagnosed with a fresh biceps tear on CTA and was treated conservatively.
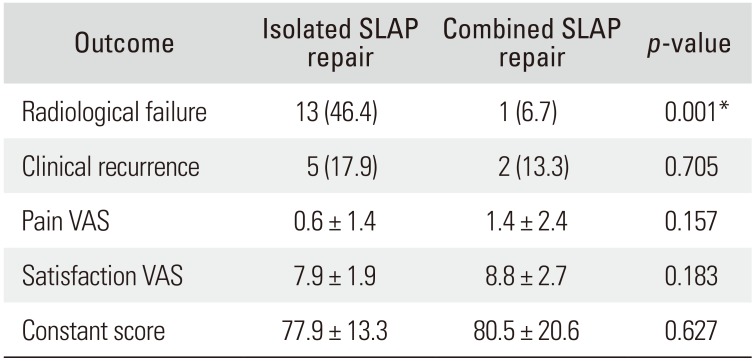
Clinico-radiological outcome comparison between isolated SLAP repair and combined SLAP repair is shown in Table 3. All of the patients who had combined SLAP repair had a separate type II SLAP lesion and a Bankart lesion. Isolated SLAP repair showed seven times greater risk of anatomical failure (risk ratio, 7.0; 95% CI, 1.2 to 141.9) than combined SLAP repair (p = 0.015). Clinical failure was also higher in isolated SLAP repair, but the difference was not statistically significant (p = 0.705).
In the current study, the failure rate increased with age. Anatomical failure occurred in 16% of patients (4/25) aged below 35 years compared to 55.6% of patients (10/18) aged above 35 years. This indicates 3.5 times higher risk of failure (risk ratio, 3.5; 95% CI, 1.2 to 11.5; p = 0.010) in patients above 35 years of age. In addition, clinical failure occurred in 20% of patients (5/25) below 35 years, as compared to 11.1% of patients (2/18) above 35 years (p = 0.712).
In terms of sex, 27.0% of male (10/37) and 66.7% of female (4/6) patients failed to heal (p = 0.082). The failure rate of dominant arm lesions was 33.6% (11/36) compared to 50% (3/6) in the nondominant arm lesions (p = 0.413). Patients who received preoperative steroids during initial management had a failure rate of 25% (4/16) as compared to 37.0% (10/17) in patients without steroids (p = 0.504).
Regarding activities, patients with non-OHA showed 47.6% (10/21) of healing failure, while patients with OHA showed 18.2% (4/22) of healing failure (p = 0.042). Patients with non-HLA showed 41.7% (10/24) of healing failure, while patients with HLA showed 21.1% (4/19) of healing failure (p = 0.157). In terms of clinical failure, patients with non-OHA had 14.3% (3/21) of failure, while patients with OHA had 18.2% (4/22) of failure (p = 0.732). Patients with non-HLA had 12.5% (3/24) of failure, while patients with HLA had 21.1% (4/19) of failure (p = 0.456). Non-OHA (risk ratio, 2.9; 95% CI, 0.7 to 7.4; p = 0.041) and non-HLA (risk ratio, 1.6; 95% CI, 0.6 to 4.4; p = 0.213; not significant) showed higher risk of healing failure. The anatomical failure rate decreased as the level of activity increased although there was no statistical significance (p = 0.317). These findings were opposite to clinical failure rates, which were higher in patients with OHA and HLA; however, these findings were not statistically significant (p = 0.901 and p = 0.891, respectively).
Regarding questionnaires on return to sports or work by phone, 41 patients were available to contact (26 patients who had isolated SLAP repair and 15 patients who had combined SLAP repair). All patients had returned to sports or work, with 82.9% (34/41) of patients had a return to their previous level of sports or work (22 out of 26 patients who had isolated SLAP repair, and 12 out of 15 patients who had combined SLAP repair). The mean time to return to sports or work after surgery was not statistically different between isolated SLAP repair and combined SLAP repair (13.1 ± 3.3 months vs. 12.9 ± 2.8 months, p = 0.873). There was no significant difference in returning to previous level of sports or work according to anatomical healing, isolated or combined SLAP repair, patient's age, OHA, and HLA (p = 0.872, p = 0.644, p = 0.325, p = 0.217, and p = 0.899, respectively).
DISCUSSION
In our study, 32.6% of SLAP lesions failed to heal, whereas 16.3% of patients had clinical failure. The mean pain VAS, mean satisfaction VAS, and mean Constant score improved significantly. Muscle strength, the subscale of the Constant score, at the final follow-up was significantly better in the patients aged below 35 years. The favorable outcome measures for anatomical healing were combined SLAP repair, OHA, male sex (near significance, p = 0.082), and the age under 35 years. Level of activity, dominance of arm, steroid therapy, and local steroid injections had no effect on anatomical healing. Although the failure rate decreased as the level of activity increased, the correlation was not statistically significant. Anatomical healing of SLAP lesions was not related to clinical outcome; clinico-radiological mismatch in the outcome of SLAP repair was found.
The current results of failure to heal (i.e., 32.6% of anatomical failure and 16.3% of clinical failure, and comparable clinical outcomes between anatomical healing and anatomical failure cases) may raise the question whether repair of SLAP lesions is indispensable. In general, SLAP lesions do not heal without surgery,2) and our data show that irrespective of anatomical healing, patients could have significant clinical improvement after surgery. Furthermore, in a double blinded randomized clinical study by Schroder et al.,4) SLAP repair did not show any clinical benefit over sham surgery. Moreover, the pathomechanism of SLAP lesions and biceps tendon lesions would be different. However, it is difficult to differentiate them due to the anchoring of the biceps tendon to the superior labrum. Considering several articles showing superior outcomes of biceps tenodesis or tenotomy to SLAP repair and the present data showing discrepancy between anatomical healing and clinical outcome,15) SLAP lesions might be a less important pathological finding than biceps tendon lesions. Thus, we attempted to address the trend of biceps tenodesis or tenotomy over SLAP repair.
It is widely accepted that combined repair of a SLAP lesion and a Bankart lesion produce better clinical outcome than isolated repairs.21516) Furthermore, in a study by Waterman et al.,17) SLAP repair combined with Bankart repair showed a higher rate of functional return than isolated SLAP repair. Burkart et al.3) reported in their biomechanical study that the repair of type II SLAP lesions only partially restored translations to the same degree of an intact shoulder joint. They suggested that improved repair techniques or an anteroinferior capsulolabral procedure in addition to the type II SLAP lesion repair might be needed to restore normal joint function. According to the Burkhart's study,3) one can predict low functional outcome and high risk of anatomical failure in isolated SLAP repair due to insufficient restoration of translation. Moreover, for those with combined SLAP lesions, fixation of both lesions to restore primary shoulder stability and to reduce pain due to symptomatic SLAP lesions might have resulted in better subjective outcome after combined SLAP repair.
In the present study, isolated SLAP repairs had seven times more risk of anatomical failure than combined SLAP repairs (p = 0.015). This could be due to insufficient restoration of translation in the isolated SLAP repair group compared to the combined SLAP repair group,3) which in turn have resulted in less stability of the glenohumeral joint and higher healing failure. In this study, we hypothesized that the high rate of healing failure would be the cause of poor clinical outcome in isolated SLAP repairs. However, as some studies suggested inconsistency in the association between isolated repair and poor clinical outcome,1819) the superior clinical outcome in the combined SLAP repair group was not of statistical significance in spite of the lower radiological failure rate (p > 0.05) in this group. Therefore, we failed to confirm our hypothesis.
Since over 80% of the population involved in sports are under 35 years of age, and the sports participation declines after the age of 35, we performed age subgroup analysis between those over 35 years and less than 35 years of age.9) In this study, we found a 3.5 times higher risk of anatomical failure in patients above 35 years (p = 0.010). One of the explanations for this may be the decrease in healing potential and labral vascularity with the advancing age.20) The clinical outcome of SLAP repair has been reported to be either the same or worse in older patients.122122) However, clinical failure in the current study was higher in patients below 35 years although the difference was not significant (p = 0.712). Hence, the correlation between age and with failure rate could not be determined. Based on the results, we carefully suggest that SLAP repair surgery in patients more than 35 years should be seriously reconsidered. In addition, unlike younger patients, older patients with a SLAP lesion might have more comorbidities including biceps lesions. Considering the results showing discrepancy between the anatomical failure rate and clinical failure rate, the surgeon should investigate other causes of symptoms first such as biceps lesions, stiffness, or impingement syndrome before treating SLAP lesions. Furthermore, if surgical treatment for a SLAP lesion was decided, the patient's age should be taken into account before reattachment of the SLAP lesion due to the high anatomical failure rate. Furthermore, we carefully suggest that the treatment should be more focused on the concomitant biceps lesion to perform tenotomy or tenodesis rather than the SLAP lesion itself.
OHA sports are well-known causes of SLAP lesions and clinical outcomes are comparatively poor in these patients which might be attributable to higher expectations and greater demands postoperatively.623) However, surprisingly, patients with non-OHA (p = 0.041) had higher rates of failure in the current study. Vascularity is less in the anterior and superior glenoid.24) Basic science studies have shown that vascularity increases at the site of stress due to stress-induced angiogenesis.2526) Thus, we assumed that the long head of biceps in OHA patients exert increased stress at the superior glenoid attachment and the vascularity of superior glenoid may be better in these patients due to angiogenesis-related improvement of blood flow perfusion.27) This fact may be responsible for better healing in OHA patients; however, the data supporting this theory are not available at present in the literature. Further studies including animal experiments are needed to confirm the impact of level of activities on vascularity. However, the two contradicting findings, better healing but more clinical failures in OHA patients, seriously question the need for repair in SLAP lesions and support the trend towards biceps tenodesis and tenotomy instead of SLAP repair.
Women in the present study seemed to have an increased risk of failure; but the majority of them underwent isolated repairs, was aged more than 35 years, and were involved in non-OHA and non-HLA. Thus, although the results were close to significance (p = 0.082), the possibility of selection bias could not be ruled out.
Several strengths should be noted in the current study. This is the first study that evaluates the reasons of SLAP repair failure. It helps us to understand the recent trend in the management of SLAP lesions and repair options that should be based on age, functional demands, level of activities, and presence of concomitant intra-articular lesions.
Several limitations of the study should be also mentioned. It is a retrospective study. Hence, it has all the inherent disadvantages of the retrospective model. The strict inclusion criteria reduced the number of eligible patients, leaving a small sample size for the evaluation. Furthermore, this small number of patients was divided into subsets according to age, sex, concomitant lesions, and activities, which would dilute the impact of the main findings. Return to sports or work was not reported in the hospital information system, and these data could only be evaluated by phone survey at a minimum of 2 years after the surgery, thus some patients were lost to contact. CTA was taken as an alternative to arthroscopy for the evaluation of anatomical healing, which is inferior to direct arthroscopic evaluation (gold standard). CTA has its own limitations (95% sensitivity and 88% specificity). Therefore, the observer's bias cannot be excluded.10) Lastly, comparison of the two different disease entities (isolated type II SLAP lesion and SLAP lesion combined with Bankart lesion) could be another limitation of the study.
Since patients with unhealed SLAP lesions had less clinical failure than the healed SLAP lesion patients, anatomical healing does not seem essential for better clinical outcome of the repair of a type II SLAP lesion, especially in patients with a higher risk of healing failure due to isolated SLAP repair, non-OHA, and age over 35 years. Therefore, we believe the indications of SLAP repair should be narrowed to prevent overtreatment.

 XML Download
XML Download