

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The use of ceramic veneers has become widespread in dentistry. The success of this practice depends on the quality of the material and the robustness of the connection formed between the tooth structure and ceramic veneer with resin-based cement.1 To achieve best practice, the resin-based cement should be polymerized properly.
Resin cements can be categorized as etch-and-rinse adhesive, self-etch adhesive, and self-adhesive. Their use to bond glass-ceramic and porcelain restorations provides better durability and esthetics and greater stability. Light-cured resin cements (LCRCs) are preferred due to their constant color profiles and durability over time.2 However, light curing cannot provide the maximum degree of conversion (DC). One alternative is provided by dual-cured resin cements (DCRCs).3
The opacity of zirconia-based fixed dental prostheses reduces light irradiance (LI) where composite cement is cured over the restoration.4 This reduced LI affects the mechanical properties and resultant bond, and has been shown to decrease the DC.5 To enhance the mechanical properties of a restoration and to prevent veneer ceramic fracture, which occurs in about 10 – 33% of cases, full-contour zirconia has been developed in parallel with improvements in dental zirconia technology.6 The new zirconia formula is more translucent, which improves the esthetic outcome and light transmission while enabling light-cured luting of the restoration. Data on the light-curing capacity of zirconia-based restorations are scarce.7
The energy emitted by monomers during composite polymerization is a determinant factor. The DC depends on the intensity of light and exposure time, as well as the type and thickness of the structure.89 In this study, the following null hypotheses were tested: the DCs of resin cements would not differ (1) between 1 day and 1 month; (2) between LCRCs and DCRCs; (3) according to the curing light unit (LED Soft Start Mode [LED SS]; QTH, and LED Pulse Delay Mode [LED PD]); or (4) according to the type of crystalline core structure.
Go to : 
MATERIALS AND METHODS
Two resin cements (RelyX Ultimate Clicker Light Cure and RelyX Ultimate Clicker Dual Cure, 3M ESPE Dental Products, St. Paul, MN, USA) were used in this study. Four computer-aided design/computer-aided manufacture (CAD/CAM) blocks (12 × 14 × 18 mm) of the same color (A1) were used; their manufacturers and compositions are provided in Table 1. Disc-shaped ceramic specimens (6-mm diameter, 1.5-mm thickness) were prepared from the monolithic blocks using a CERCON CAD/CAM system (DeguDent GmbH, Hanau-Wolfgang, Germany). The minimum sample size was calculated with a power analysis (n = 10/group) and the groups designed for the study are provided in Fig. 1. Each specimen was irradiated for 40 s with LED Soft-Start and LED pulse-delay units (WOODPECKER LED C) or for 20 s with a QTH unit (MEGALUX-E, MEGADENTA, Radeberg, Germany). The geometric shape of the discs was standardized using 3D design software (TruTops, TRUMPF, Ditzingen, Germany). The coordinates of the designed shape were processed by a computer numerical control (CNC) unit (TRULASER 3530, 4 kW, TRUMPF), and five stainless-steel sample templates were produced to guide the milling of the blocks.
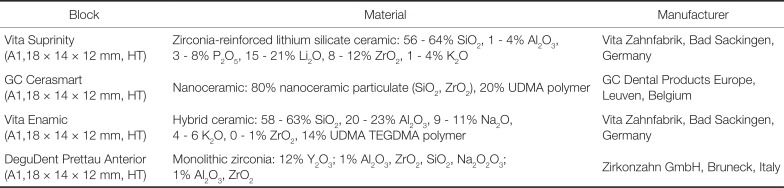
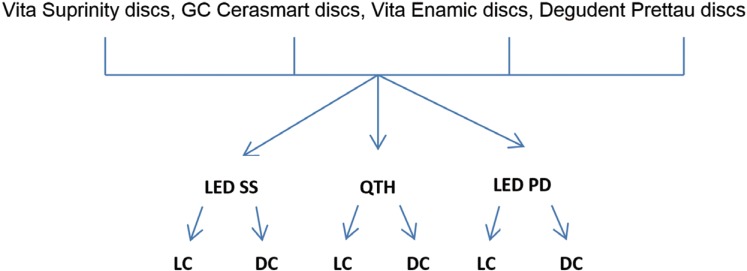
Table 1
Blocks and manufacturers
![]()
Each specimen was placed in a stainless-steel mold with four layers. The bottom layer had a thickness of 2 mm and 2-mm-diameter holes to remove excess cement and to prevent air bubble formation in the structure. The second layer had a thickness of 2 mm and 5-mm-diameter holes for test specimens prepared with the two resin cements. The third layer had a thickness of 1.5 mm and 6-mm-diameter holes for the placement of ceramic discs. The top layer had a thickness of 6 mm and 8-mm-diameter holes in which to settle the tip of the light source. These four layers with 10 holes were fixed with a screw at the corner to ensure the transmission of light through the ceramic disc to the cement. All layers of the mold were manufactured with the CNC unit. Thus, the center points of all holes were identical.
The standardization of geometrical shapes of the used discs was modeled at 3D design software (TRUMPF, TruTops, Ditzingen, Germany) in this study. The coordinates of designed shaped was processed by the CNC (Computer Numerical Control) unit (TRUMPF, TRULASER 3530 4 KW, Germany) and the templates of the samples was produced by milling of stainless steel block. Test specimens were formed as a base component, and a mixture of base and catalyst components and light was applied for 40 s with LED Soft-Start and LED pulse-delay units (WOODPECKER LED C) or for 20 s with a QTH unit (MEGALUX-E, MEGADENTA). A total of 300 resin cement specimens (1.5 mm thickness, 6 mm diameter; n = 10/group) were prepared. Three sets of specimens (n = 30) served as controls for each cement and were exposed to the light source directly. The remaining specimens (n = 240, 4 groups) were exposed to the light source through the 1.5-mm-thick ceramic discs.
For light polymerization, the LCRC base was placed in a stainless-steel test setup with the help of a plastic pipe. Transparent tape was placed between the cement disc and stainless-steel layer. The top layer of the test setup (8 mm diameter, 6 mm thickness) was placed above the layer with the cement to ensure direct contact between the cement and light source tip. Light scattering was prevented by using a light source tip with a diameter equal to that of the top layer hole (8 mm; Fig. 2).

The 240 disc-shaped samples of this study was prepared by using CERCON (DeguDent GmbH, Hanau-Wolfgang, Almanya) CAD/CAM system. Four CAD/CAM blocks, which were Vita Suprinity, Vita Enamic, GC Cerasmart and Degudent Prettau Anterior, was used. All blocks have dimensions of 12 × 14 × 18 mm. 5 stainless steel templates were prepared for milling 5 ceramic samples from each block.
The DC of each specimen was measured by Fourier transform infrared (FT-IR)/attenuated total reflection spectroscopy (Spectrum 100, Perkin-Elmer, Waltham, MA, USA) via methacrylate (aliphatic) C=C stretching and polymeric methacrylate (aromatic) C=C stretching. The data were transferred from the time domain to the frequency domain, and the different absorbance values were graphed. Infrared spectroscopy is a basic, reliable, and fast technique for the identification of different functional groups in a structure. The FT-IR process is based on the interaction between an electromagnetic ray and molecules or atoms. DCs were measured after 1 day and 1 month. At the following steps, the spectra of the polymerized specimens were measured in the range of 4000 – 600 cm−1 at 4 cm−1 resolution with four scans. DCs were calculated from data obtained at the frequencies of 1638 cm−1 (C=C stretching of the aliphatic group) and 1608 cm−1 (C=C stretching of the aromatic group) using the following formula:

where (aliphatic C=C) polymer absorption peaked at 1638 cm−1 of the cured specimen, (aromatic C=C) polymer absorption peaked at 1608 cm−1 of the cured specimen, (aliphatic C=C) monomer absorption peaked at 1638 cm−1 of the uncured specimen, and (aromatic C=C) monomer absorption peaked at 1608 cm−1 of the uncured specimen.10
Statistical analysis was performed using SPSS 25. The Mann-Whitney U test was used to compare data from pairs of test groups, and the Kruskal-Wallis H test was used for comparison of three or more test groups. The significance level was set to P < .05.
Go to :
RESULTS
The chemical structures of the resin cements, crystalline core structures of ceramic restorations, and type of light-curing unit affected the success of polymerization. Differences in these parameters resulted in different DC ratios (P < .05). Among resin cement specimens exposed directly to light, DC values were significantly lower for specimens cured with the LED pulse-delay unit (P < .05; Table 2, Fig. 3, Fig. 4, Fig. 5). Among specimens cured with ceramic discs, DC values were significantly higher for those cured with the LED Soft-Start unit (P < .05; Table 3, Fig. 5). DC values were significantly higher for Vita Suprinity than for the other restoration materials (P < .05; Table 3, Fig. 6). DC values were greater for the RelyX Ultimate Clicker DCRC than for the RelyX Ultimate Clicker LCRC. In addition, DC ratios were larger at 1 month than at 1 day, regardless of the the type of light-curing unit or resin cement (Table 3, Fig. 6).
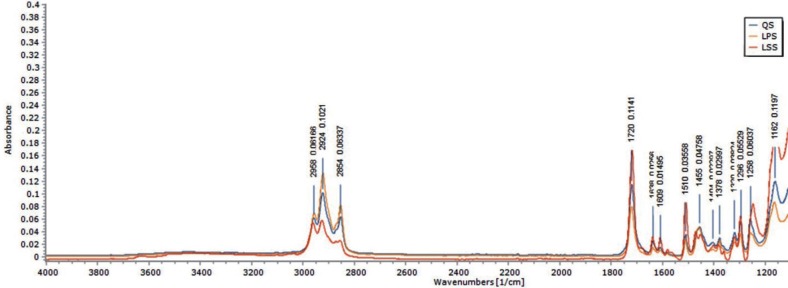 | Fig. 3Absorbance of RelyX Ultimate Clicker light-cure and dual-cure cements exposed to direct light.
|

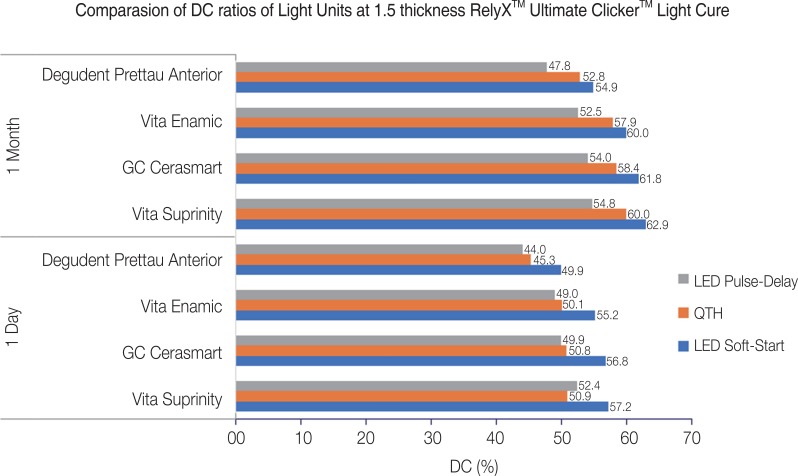 | Fig. 5DC ratios of RelyX Ultimate Clicker light-cure cement according to light unit and restorative material.
|
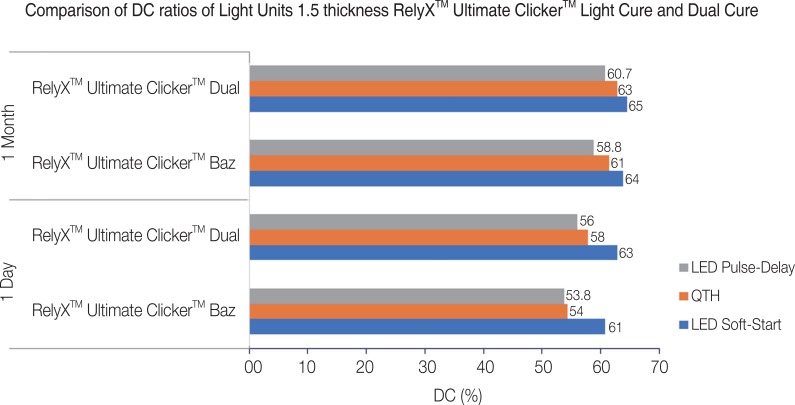 | Fig. 6DC ratios of RelyX Ultimate Clicker light-cure and dual-cure cements according to curing light.
|
Table 2
Degrees of conversion of RelyX Ultimate Clicker cements exposed to direct light
![]()
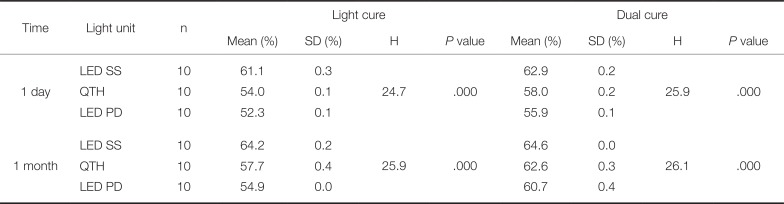
Table 3
Degrees of conversion of RelyX Ultimate Clicker cements cured with different light units (n = 10/group)
![]()
The DCs for the RelyX Ultimate Clicker DCRC and LCRC were 63.0% and 60.8%, respectively, with no specimen attenuating the light (Table 3, Fig. 6). The DC decreased significantly with the change in LI, regardless of the brand (P < .05; Table 4, Fig. 6).
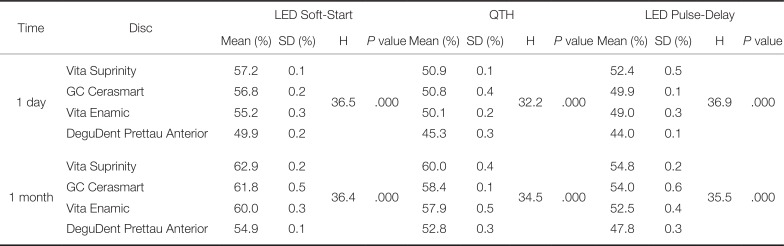
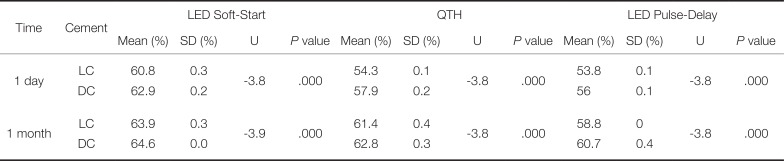
Table 4
Degrees of conversion of RelyX Ultimate Clicker light-cure cement according to curing light and ceramic restoration material (n = 10/group)
![]()
Go to :
DISCUSSION
In this study, the DC and surface characteristics of two different types of resin cements were determined under the conditions of different type of crystalline core structures. The DC was affected by the type of crystalline core structures, which were Vita Suprinity (a zirconia-reinforced lithium silicate ceramic), GC Cerasmart (nanoceramic), VitaEnamic (hybrid ceramic), and Degudent Prettau Anterior (monolithic zirconia block) at 1.5 mm thickness. The type of light-curing unit significantly affected the success of polymerization of resin-based luting cements. The power of the light unit, as well as exposure time and distance, must be considered carefully.11 The DCs of resin cements were also affected by the type of crystalline core structure.
The polymerization of resin cement is affected by various conditions, including the structure, thickness, color and translucency of restorative materials; the effective area in which the restoration is applied; the LI and exposure time of the light source; and the diameter of the light source tip and its distance from the restorative material.11213
The chemical, the light, and the dual cure polymerizing resin cements are chosen for bonding of all ceramic restorations. Among these three types of cements, the light and the dual cure polymerizing resin cements are preferable due to their color stabilities, better mechanical properties, and longer durability.14 The DC of LCRCs depends on the power, density, and wavelength of the curing light. To ensure optimum polymerization, the light density should be 300 mW/cm2. The resin material contains the photoactivator camphoroquinone, which is activated at wavelengths of 420 – 470 nm. When these conditions are not met, polymerization is inhibited to various degrees, leading to defects in the physical and chemical properties of the cement.1516 LCRCs are never fully polymerized in zones where light is cannot be applied. Insufficient polymerization results in decreased toughness and durability, leading to fragility and loss of adhesion.17 DCRCs, which can be polymerized by light or chemically, were developed to solve the problem of insufficient polymerization due to thickness. They are used when the thickness exceeds 2 mm and in interproximal zones where light application is difficult.18 The resulting increase in the DC ratio reduces the ratio of residual monomers and significantly increases biocompatibility.3
The C=C double bonds in monomer chains should react in the reaction to assess full polymerization. In parallel with this reaction, viscosity increases and monomer-to-polymer conversion slows during polymerization; residual monomers remain.1920 Direct FT-IR is the most commonly used method for calculation of the DCs (or degrees of monomer conversion) of resin-based restorative materials. Hardness tests measure polymerized samples at defined points, whereas FT-IR measures the DC of the entire structure.10 Therefore, FT-IR generates more consistent and representative DC results than do hardness tests.
Using FT-IR, Moraes et al.21 determined that exposure of RelyX ARC resin cement samples to a QTH light source for 40 s increased the DC (82.1% vs. 61.1%) and reduced the number of residual monomers in comparison with chemical polymerization. In another study, Moraes et al.22 assessed the effect of the same (dual-cure) light exposure relative to auto-polymerization on the DCs of BisCEM, Maxcem Elite, RelyX Unicem, seT, SmartCem 2, and RelyX ARC resin cements using FT-IR at 15 and 30 minutes. The DC ratios after dual polymerization and chemical polymerization were as follows: BisCEM, 46.6% – 7% and 51.0% – 10.5%; Maxcem Elite, 54.2% – 44.7% and 60.5% – 53.6%; RelyX Unicem, 49.1% – 31.5% and 50.8% – 34.6%; seT, 71.4% – 23.8% and 73.1% – 34.7%; SmartCem 2 , 37.8% – 35.1% and 47.7% – 39.9%; and RelyX ARC, 74.0% – 58.9% and 75.1% – 62.4%, respectively. The difference in DC ratios among resin cements was explained by the difference in the chemical specifications of luting cements.22 In both studies, the researchers used RelyX Unicem resin cement with 40 s QTH light exposure and measured DC ratios using direct FT-IR. They explained the difference in DC ratios between studies in relation to the chemical specifications of luting cements and environmental effects. In this study, RelyX Ultimate resin cement was light cured and dual cured, and the degree of polymerization was measured by direct FT-IR. The LED Soft-Start light source was more effective than the other light sources, according to the DC ratios (%) was measured for LED SS regardless of the cement type. As given in Table 4 the effect of LED SS light source is significantly higher than other light sources (P < .05). The difference in DC ratios between resin cements can be explained by the density of the QTH light unit and the chemical specifications of luting cements.
In this study, a resin based luting cement which has a capability of both light cure and dual cure polymerization was exposed with LED SS, QTH and LED PD light units to assess the effect of light units on DC. For both, DC ratios for the RelyX Ultimate LCRC and DCRC were higher at 1 month than at 1 day, regardless of light source. Thus, the first null hypothesis was rejected.
In the present study, the polymerization characteristics of RelyX Ultimate resin cement was analyzed as RelyX Ultimate LCRC and RelyX Ultimate dual cure polymerization with LED SS, QTH and LED PD. The DC of RelyX Ultimate LCRC exposed with LED SS, QTH, LED PD was measured at 1 day and results were 62.9 ± 0.3, 54.3 ± 0.1, and 53.8 ± 0.1, respectively (P < .05) (Table 4). RelyX Ultimate DCRC exposed with LED SS, QTH, LED PD was measured at 1 day and results are 63.0 ± 0.2, 57.9 ± 0.2, and 56.0 ± 0.1, respectively (Table 4). In addition, DC ratios were significantly higher for DCRC than for LCRC specimens. Thus, the second null hypothesis was rejected. In a comparison of light and dual cure polymerization characteristics of RelyX Ultimate resin cement, a dual cure had significantly higher ratios than light cure (P < .05). This finding is in agreement with those of similar studies, which have shown that polymerization of DCRCs continues in the absence of light.11 Another explanation for this difference between LCRCs and DCRCs is the lesser photo-activator content of the latter.1 Therefore, the second null hypothesis was rejected.
Souza et al.23 used direct FT-IR to measure DCs in two types of A2-colored crystalline core structure cemented with RelyX U-100 DCRC and LCRC and exposed to 40 seconds curing with an LED Soft-Start unit or 20 seconds curing with a QTH unit, respectively. The DCs obtained with LED Soft-Start and QTH curing were 59.98% ± 2.93%, 49.84% ± 1.91%, 52.36% ± 2.5%, and 43.93% ± 1.64%, respectively. The researchers stated that the LED Soft-Start, or any LED-based light unit, achieved greater polymerization depth than did the QTH unit, as the LED wavelength is in the range required by the starting agent camphoroquinone.23 Tarle et al.24 measured the DCs of three types of composite resin polymerized for 40 seconds with LED and QTH units using indirect FT-IR. The DC ratios for specimens cured with the LED and QTH units were 54.9 – 65.4% and 63.5 – 73.5%, respectively. Thus, the QTH unit performed better than the LED unit. The researchers explained this unexpected situation with reference to the technology of the 1 generation LED unit, which results in lesser polymerization depth.24 Bala et al.25 measured the DCs of three types of composite material polymerized with LED and QTH units using direct FT-IR. The maximum and minimum DCs were 61.1% ± 0.4% and 50.6% ± 0.6%, and 55.6% ± 0.7% and 47.4% ± 0.5%, respectively. In our study, the DC ratios for RelyX Ultimate resin cement cured with LED and QTH units at 1 day were 63.4 – 62.6% and 54.5 – 53.7%, respectively. The difference in DC ratios between studies can be explained by differences in the chemical properties of the resin and composite materials. Resin cements have more filler with bigger size than has composite materials. The power of the light units and the light density also had significant effects on the DC. Therefore, the third null hypothesis was rejected.
Sulaiman et al.26 polymerized RelyX Ultimate DCRC specimens (40 µm thickness) through Prettau Anterior, Bruxir Zirconia, Wieland Zenostar Translucent, and Katana High Translucency discs for 20 seconds using an LED Elipar S10 light unit, and then measured DCs using direct FT-IR. The DCs were 60.40% ± 0.43%. 57.73% ± 0.77%. 58.29% ± 62% and 60.87% ± 1.03%, respectively. In our study, the DC of 2-mm-thick specimens cured with the LED unit was 52.9% ± 0.5%. This difference is attributable to the difference in specimen thickness.
RelyX Ultimate LCRC was exposed with LED SS and QTH, and 1 day DC was recorded for Vita Suprintiy (a zirconia-reinforced lithium silicate ceramic) as 57.2 ± 0.1% and Degudent Prettau Anterior (monolithic ceramic) disk as 45.3 ± 0.3% (Table 3, Fig. 5).
RelyX Ultimate LCRC was exposed with LED SS and LED PD and 1 day DC was recorded for Vita Suprintiy (a zirconia-reinforced lithium silicate ceramic) as 57.2 ± 0.1% and Degudent Prettau Anterior (monolithic ceramic) disk as 44.0 ± 0.1% (Table 3, Fig. 5). RelyX Ultimate LCRC was exposed with QTH and LED PD and 1 day DC was recorded for Vita Suprintiy (a zirconia-reinforced lithium silicate ceramic) as 50.9 ± 0.1% and Degudent Prettau Anterior (monolithic ceramic) disk as 45.3 ± 0.3% (Table 3, Fig. 5).
Sen and Us27 measured the translucency of Lava Ultimate (nanoceramic), Vita Enamic (hybrid ceramic), Vitablocs Mark II (feldspathic ceramic), Vita Suprinity (reinforced lithium-silicate ceramic), and IPS e.max CAD (lithium disilicate ceramic) CAD/CAM discs with 12-mm diameters and 1.2-mm thicknesses using a Colour Eye 7000A (X-Rite) spectrophotometer. The translucency values were 30.0 ± 0.9, 16.0 ± 0.6, 29.0 ± 0.7, 31.0 ± 1.0, and 26.0 ± 0.6, respectively. In our study, the highest DC ratio was obtained for cement polymerized under Vita Suprinity, which was the most translucent material tested. Thus, the fourth null hypothesis was rejected. The difference in DC ratios can be explained by differences in crystal structure and resin cement. DeguDent Prettau Anterior, the least translucent material, has an opaque polycrystalline structure. However, DC ratios differed significantly between GC Ceresmart and Vita Enamic, which have similar filler profiles and organic and inorganic contents. This difference is attributable to the nanoparticle and aluminum contents. The translucency of all-ceramic restorations increases with particle size. The pores in the hybrid ceramics were filled with the polymer resin. Resin matrix and nanoceramic particulates bond to each other with strong cross-linking, and the pores filled with nanoparticles in ceramic matrix shows homogenous structure. Nanoceramics have nanoparticles, whereas hybrid ceramics have macroparticles. Hybrid ceramics contain 20 – 23% aluminum, whereas nanoceramics have no aluminum content.2829
The success of polymerization depends on proper disc selection and cementation. The success of cementation is affected by the light source, type of crystalline core structure, ceramic disc thickness, and all-ceramic restoration color. It also depends on the cement type, exposure time, and technique.
Go to :
CONCLUSION
Within the limitations of this laboratory study, the following can be concluded: the DC of an all-ceramic restoration is affected by the amount, size, and type of crystal; the structure and chemical content of the resin-based luting cement; and the type of curing light unit. The curing light unit (in this study, LED Soft-Start, QTH, and LED pulse delay) is a determinant factor for the DC ratio. Also, DC ratios for all combinations of crystalline core structure and curing light were greater at 1 month than at 1 day. The type of light unit, density of light, exposure time, and distance between the light unit tip and the restorative material are very significant. They should be considered carefully before light curing is performed.
Go to :
 XML Download
XML Download