

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
For the long-term stability of implant-supported prostheses, a passive fit between the implant fixture and the upper prosthesis should be achieved.12 If the stress is concentrated on prosthesis, as in the absence of passive fit between the upper prosthesis and the implant fixture, it can cause the loosening or fracture of screw, fracture of abutment or fixture, and/or crestal bone loss.234 To obtain a passive fit of the implant and the upper prosthesis, it is necessary to make a precise master cast. The production of an accurate implant master cast starts with the accurate implant impression.567
Several impression techniques have been suggested to make a master cast that will ensure the passive fit of implant-supported prostheses.689 There are two conventional impression methods: pick-up impression technique and transfer impression technique. For the pick-up impression technique, square copings and a tray with an opening are needed, allowing the impression coping screw hole to be exposed. After the impression material is polymerized, the copings are unscrewed to be removed along with the impression. Then the implant analogs are connected to the copings to fabricate the master cast.
For the transfer impression technique, tapered copings and a closed tray are needed. The copings are connected to the implants, and after impression taking, the copings remain connected. Then, the copings are removed and connected to the lab analogs, and the coping-analog assemblies are reinserted in the impression before fabricating the definitive cast.
There have been several studies comparing the accuracy of the pick-up and transfer impression techniques. While some authors reported better results with the pick-up technique,89101112 other authors reported no difference in accuracy between the two impression techniques.131415161718
Both pick-up and transfer techniques require an additional impression of opposite dentition and bite registration after the impression taking. On the other hand, when using the dual arch impression technique in the production of fixed prosthesis, three records can be obtained at the same time. In addition, Parker et al.19 reported that by using dual arch impression technique, the patient's maximum intercuspation is recorded at the time of impression taking, making more accurate prosthesis. However, in the case of conventional implant impression, dual arch impression is impossible because of the height of impression coping. Recently, a new impression coping has been developed to enable dual arch impression by shortening the height of impression coping. This impression coping is basically a transfer impression coping, and has rectangular shape and low height of 4 mm or 6 mm, so impression using a dual arch tray has become possible. If the impression technique using this new impression coping has similar accuracy to the conventional implant impression technique, it will have clinical usefulness because it can reduce the chair time.
Therefore, the purpose of this study was to analyze the accuracy of the dual arch implant impression using newly developed impression coping by comparing with the impressions using conventional impression copings. The null hypothesis of this study is that there is no difference in accuracy between the dual arch implant impression method and the conventional impression method.
Go to : 
MATERIALS AND METHODS
A partial edentulous dentoform with missing maxillary left second premolar and first molar was prepared (Fig. 1A). Internal connection type bone level implants (Luna S, Shinhung Co., Seoul, Korea) with a diameter of 4.5 mm and a height of 10 mm were placed on missing maxillary left second premolar and first molar on dentoform model (Fig. 1B). Impression copings were connected to each implant fixture. The experimental groups were divided into two groups according to the impression techniques (Table 1).

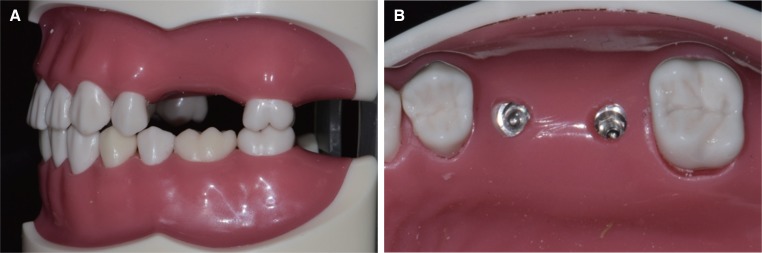 | Fig. 1(A) Reference model with maxillary left second premolar and first molar missing, (B) Implant fixtures placed.
|
Table 1
Impression copings and methods in this study
![]()
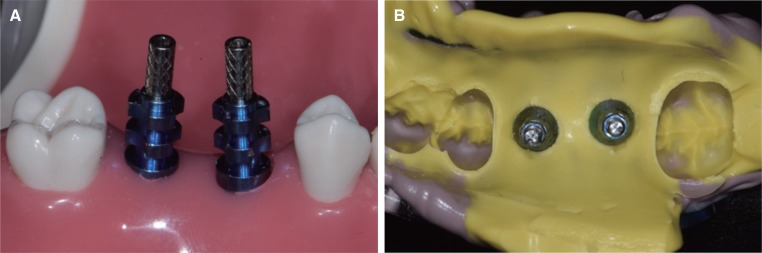
In Group 1 (n = 10), impression was made with pick up impression copings and an acrylic resin custom tray. The custom tray with an opening was fabricated with visible light-curing acrylic resin (Triad TruTray VLC, Dentsply Inc., York, PA, USA). After the pick up impression copings were screwed to the fixture, dual-mix impression was made with low viscosity silicone impression material (Imprint II Garant Light Body, 3M ESPE, St. Paul, MN, USA) loaded on the copings with air blowing for thin spreading and high viscosity silicone impression material (Imprint II Garant Heavy Body, 3M ESPE) placed in the tray. After the impression material was cured, the impression coping was unscrewed and the impression was removed from model (Fig. 2). Implant analogs were then connected to impression coping.
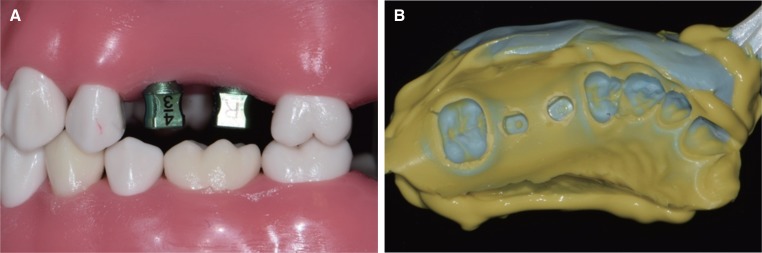
In Group 2 (n = 10), the dual arch impression was made with bite impression copings (Luna S, Shinhung Co., Seoul, Korea) and a plastic bite tray (Triple Tray, Premier Dental Products Co., Norristown, PA, USA). First, the appropriate size of bite impression coping was connected to the implant fixtures on the dentoform model. Because the gingival thickness was 3 mm and the occlusal clearance was 6 mm on the dentoform model, impression coping with a gingival height of 3 mm and a height of 4 mm was selected. After the bite impression copings were screwed to the fixtures, one-step putty/light-body impression was made with low viscosity silicone impression material (Imprint II Garant Light Body, 3M ESPE) loaded on the copings with air blowing for thin and even spreading and putty type silicon impression material (Exafine Putty Type, GC Co., Tokyo, Japan) placed in the tray. The model was occluded with maximum intercuspation during setting of the impression materials. After setting of impression materials was completed, the impression was removed from the model, implant analogs were connected to the impression copings and the coping-analog assemblies were reinserted in the impression (Fig. 3).
After connecting the implant analogs to the impression copings, soft tissue around the implant was formed using additional silicone (GumQuick, DreveDentamid GmbH, Unna, Germany), and a master cast was fabricated by pouring the type IV dental stone (Heraeus Kulzer GmbH, Hanau, Germany). The impression procedures were repeated 10 times in each group, and therefore a total of 20 master casts were fabricated.
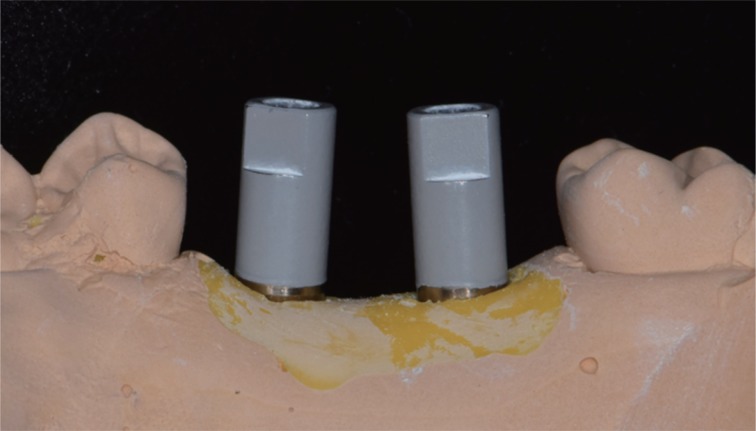
The accuracy measurement procedure was carried on digital 3D scanning and computer program analysis. The implant scan body was connected to the implant fixtures of the dentoform model and scanned using a laboratory 3D scanner (7Series, Dental Wings Inc., Montreal, Canada). The digital scanning standard tessellation language (STL) dataset was obtained from reference model and it was used as control. Scanning was also performed on master casts of Group 1 and 2. Scanbodies were connected to the analog of the master casts and scanned in the same way (Fig. 4). In all the procedures, the same scanbodies were connected to the same position to eliminate the effect of scanbody variances. Each of STL datasets obtained from test groups were superimposed with the STL dataset of the reference model using superimposition software (Geomagic control X, Geomagic, SC, USA). To ensure a precise superimposition, parts other than implant scanbodies were removed from digital model using image processing. After scanbody in maxillary left second premolar implant was selected as a reference to superimpose, control and test STL datasets were aligned by bestfit algorithm. The three-dimensional differences between a control and test STL datasets were illustrated in a color-coded map.
A statistical analysis was performed with SPSS software (SPSS statistics 21.0, SPSS Inc., Chicago, IL, USA) with 95% confidence interval to investigate the volumetric deviations from the comparisons. The normality of the measured values was tested using the Kolmogorov-Smirnov test and the Shapiro-Wilk test. Because of normal distribution of the measured values, the accuracy of 3D deviations was analyzed using the independent samples T-test.
Go to :
RESULTS
Each dataset obtained by scanning master casts was superimposed with control dataset of the scanned reference model, and 3-dimensional deviation was calculated (Table 2). The 3-dimensional deviation between the two superimposed scanned images was represented as a color-coded map (Fig. 5). The overall mean values of 3D deviations from the digital scanning and superimpositions are shown in Fig. 6. The mean 3D implant deviations of the pick up impression group (group I) and the dual arch impression group (group II) were 0.029 mm and 0.034 mm, respectively. The difference between groups I and II was not statistically significant (P = .075). Hence, the null hypothesis of this study that there would be no clinical difference on the accuracy of casts produced by different implant impression technique was corroborated.
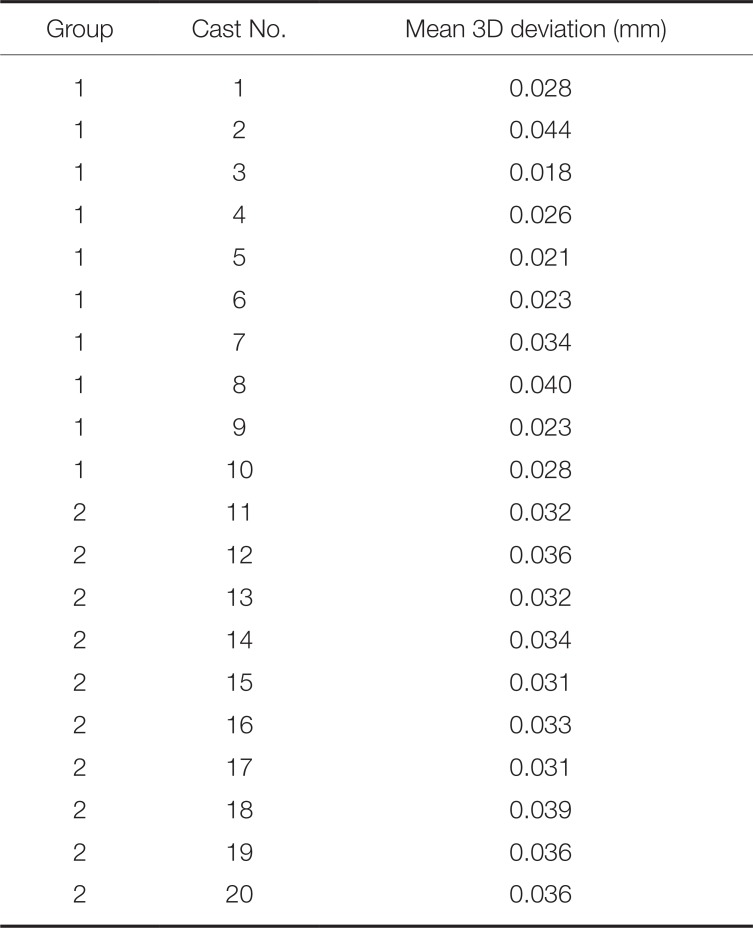
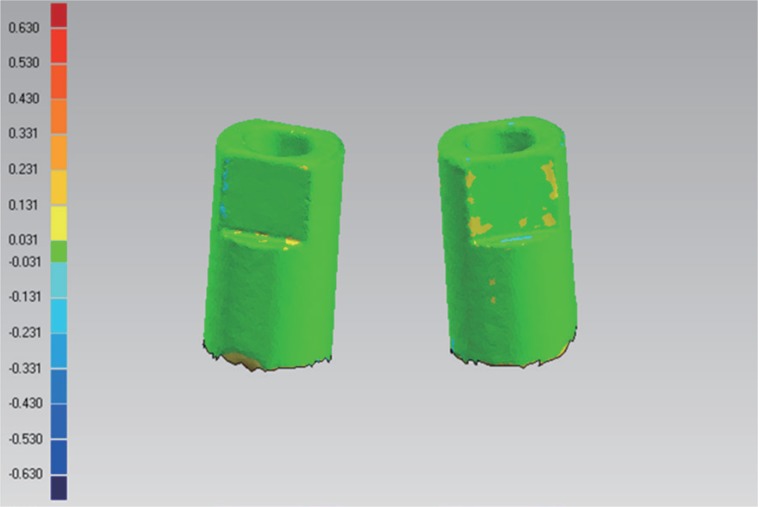
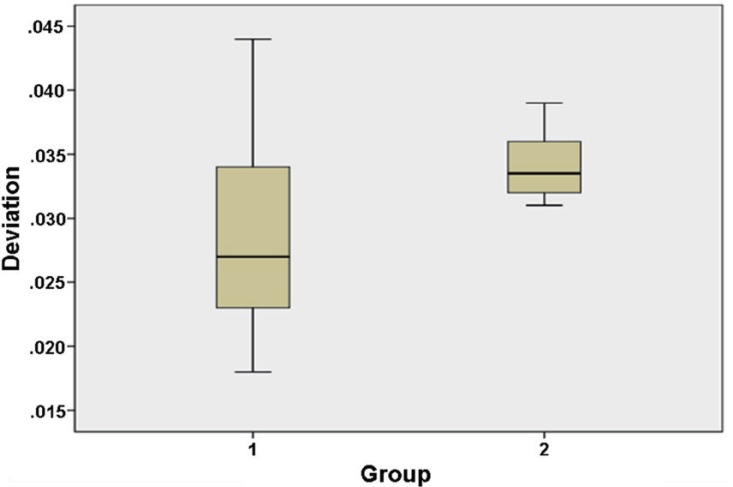
Table 2
3D implants deviation (in mm) of each master cast
![]()
Go to :
DISCUSSION
The null hypothesis of this study, which stated no difference in accuracy between the dual arch implant impression method and the conventional impression method, has been corroborated. The results of this study indicate that the dual arch implant impressions have similar accuracy when compared with the conventional pick up impressions. In addition, the mean value of the 3D deviation was smaller in group 1 than in 2, but the variance in group 1 was greater than 2. This means that the dual arch impression group has more consistent results than the pick up impression group.
The dual arch implant impression technique used in this study is a slight modification of the transfer impression technique. This impression coping is available in a variety of sizes to choose gingival height and occlusal height for each clinical situations. In this study, a coping with a gingival height of 3 mm and an occlusal height of 4 mm was selected. Because of its shortened height, impression coping does not connect with the opposite dentition; impression using the dual arch tray became possible. Since the height of the impression coping is short, it is easy to use when there is limited interocclusal space. It also becomes useful when the implantation angles of the implants are not parallel. Furthermore, the overall chair time can be reduced because the technique does not require the opposing dentition impression and interocclusal record.
The transfer impression technique is known to be less accurate than the pick up impression technique because the coping needs to be repositioned within the impression material after connecting the coping and fixture analog.9 However, many researches prove that there is no difference in the accuracy between the pick up impression technique and the transfer impression technique.151617181920 The present study also supports previous findings that there is no difference in those two techniques. Indeed, transfer impression technique is considered efficient and convenient; it is widely used in clinics because the technique does not require an open tray.2021 In addition to this advantage, dual arch implant impression techniques presented in this study have more merit, since impression of implant, opposing teeth, and interocclusal record can be obtained at once.
It is considered that implant impression accuracy also depends on the design of the impression copings.2223 Research suggests that a more retentive design of impression coping would result in a more accurate impression. The bite impression coping used in this study was designed to have enough retention with the rectangular body and side indentation despite its short height, compared to the tapered design of the conventional transfer impression coping.
When fabricating the articulated cast, using dual arch impression technique is considered to be more accurate when comparing the techniques that require manual repositioning of upper and lower cast with interocclusal record.1924 Under the forces of occlusion, the tooth shifts physiologically with the presence of the periodontal ligament, and mandible bends as masseter muscle pulls.2526 As dual arch impression technique records such changes, it has additional advantage over conventional impression techniques. Previous studies evaluating the dimensional accuracy of casts made with the dual arch impression technique showed a clinically valid accuracy compared to casts made with conventional full arch impression techniques using custom trays.2427 In those studies, it was recommended to use more rigid impression materials and trays. In this study, light body impression material was loaded on impression coping and spread thinly by air blowing and putty type impression material was loaded on tray to obtain rigidity and accuracy of impression.
In this study, digital scanning was used as an evaluation method of impression accuracy. Conventional methods of assessing implant impression accuracy include use of a coordinate measuring machine or a microscope. A method using a coordinate measuring machine is expensive and the process is complicated. A method using a microscope may cause errors because the measurement is done manually. Recently, there have been many studies comparing the 3D deviation calculated by superimposing the digital images obtained from the optical scanner to measure the accuracy of implant impression technique.2829303132 This method is efficient and convenient, and can be used to intuitively evaluate 3D deviations using a color map.
This is the first study to evaluate the accuracy of fixture level implant impression using a dual arch tray. The results of this study show that implant impression technique using a dual arch tray is a clinically valid option when fabricating single or two unit implant-supported fixed prostheses in stable occlusion state. The limitation of this research is that it was an in vitro study. In this study, we focused on the impression accuracy of the impression coping because it is impossible to reproduce the minute changes in the oral cavity under occlusal force. In addition, the indication of this method can be limited to cases of the partially edentulous patient with stable occlusion. However, it is considered that the bite impression copings are available for checking a bite in the more extended missing cases. Further clinical studies will be required to evaluate not only the accuracy of impression but also the accuracy of interocclusal record.
Go to :
CONCLUSION
Within the limits of this study, the accuracy of the master cast made by the dual arch implant impression technique using newly developed impression coping was similar to that of the master cast made with the conventional pick up impression technique. Therefore, the dual arch implant impression technique will be a method to reduce the chair time while achieving similar accuracy to the conventional implant impression technique in the partially edentulous patient with stable occlusion.
Go to :
 XML Download
XML Download