

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Major objective of the root canal obturation is to provide a hermetic seal that prevents reinfection and recontamination due to leakage of fluid and microorganisms into root canal system [1]. Various types of obturation material are now available for these purposes. Calcium silicate-based, bioceramic sealer (BCS; Totalfill BC Sealer, FKG Dentaire SA, La Chaux-de-Fonds, Switzerland) in a premixed-syringe with intracanal tip has been introduced. According to the manufacturer's instruction, BCS is designed to be used with bioceramic (BC) impregnated gutta percha cone (TotalFill, FKG Dentaire SA), and the use of a single-cone obturation technique is recommended. Matched-master cone is preferred to tightly fit core material to provide tight seal with the sealer. With this technique, the sealer can be forced laterally by the hydraulic force into the irregularities and dentinal tubules. BCS requires remaining moisture within root canal to set by hydration reaction [2]. BCS possesses promising properties, such as excellent biocompatibility and bioactive [345], no shrinkage after setting [6], and containing antimicrobial activity [78].
Microleakage can occur due to small gaps and voids along the obturated root canal, allowing bacterial penetration and repopulation of microorganisms [9]. Thus, aim of root canal obturation is to provide bacterial-tight seal, achieved by good obturation quality with minimal voids/gaps formation in the areas between sealer-dentin and/or sealer-cone. Bacterial leakage test is one of the valid methods to evaluate the quality of obturation that provides biologically and clinically relevant information [101112]. Penetration of endodontic-pathogen bacteria (such as Enterococcus faecalis [E. faecalis]) from the upper chamber through the filled root canal into the medium in the lower chamber is detected by turbidity change of medium. This method is believed to be more reliable and clinically related than the other methods, such as dye penetration or fluid filtration [1314]. For instance, dye penetration could be limited by entrapped air/liquid in the gaps. Other variables, i.e. pH, chemical reaction, immersion time, and molecular size of dye are also contributing factors affecting the leakage result [15], so the validity of dye leakage test is questionable.
Micro-computed tomography (CT) analysis is an accurate method that provides 2 and 3 dimensional (2D and 3D, respectively) views of the filled root canals without damaging the samples. Using micro-CT, adaptation as well as gaps and voids from the obturation can be qualitatively observed [1617]. Quantitative data of these parameters are also obtained from the 3D assessment.
Due to several advantages of bioceramic cone (BCC)-sealer system, superior sealing in root canal obturation is expected. From recent studies, BCS, used with gutta percha (GP) cone had comparable sealing in oval-shaped root canals to other conventional sealers using lateral condensation, continuous wave condensation, and single cone technique [21819]. However, there are limited available information about sealing potential of BCC-sealer system in current literatures.
The purpose of this study was to evaluate bacterial leakage of round-shaped root canals obturated with BCC or GP cone in a combination with BCS or epoxy resin-based sealer (AH Plus [AH], Dentsply-Maillefer, Tulsa, OK, USA), using a matched single-cone technique. Obturation quality in terms of adaptations to root canal walls and volume of gaps and voids, was further assessed using 3D micro-CT analysis.
MATERIALS AND METHODS
Bacterial leakage test
1. Sample preparation
The study protocol was approved by the Ethics Committee of the Faculty of Dentistry/Faculty of Pharmacy, Mahidol University (reference no. MU-DT/PY-IRB 2016/010.1706), Bangkok, Thailand. Ninety-two extracted maxillary molars with intact, straight distobuccal (DB) roots were collected and stored in 0.1% thymol solution. To control variation of root canal anatomy, periapical radiographs were taken in buccolingual and mesiodistal directions, only DB roots with a Vertucci's type I (1-1) root canal [20] were included. DB roots were sectioned perpendicular to the long-axis of root at cemento-enamel junction level using a slow-speed diamond saw with water-coolant (Isomet 1000, Buhler, Lake Bluff, NY, USA). To control working length and leakage distance, the sectioned DB roots with a length of 9–10 mm were further reduced until a uniform length of root at 8 mm was obtained using a high-speed fissure diamond bur. Each DB root canal was negotiated with a size 10 K-file (Dentsply-Maillefer), and the patency was confirmed by passing the file through the apical foramen.
Working length was determined at 1 mm short from the apical foramen. Next, a smooth glide path was created with a size 15 K-file at the working length. The root canals were shaped with a sequence of RaCe rotary Ni-Ti instruments (FKG Dentaire SA) to an apical size 40/0.06. The canals were irrigated with 2.5% sodium hypochlorite (NaOCl) with a disposable syringe and a 25-gauge needle, and a size 10 K-file was passed through the apex to maintain apical patency. Smear layer was removed by rinsing with 3 mL of 17% ethylenediaminetetraacetic acid (Endo Clean, M Dent, Bangkok, Thailand) for 1 minute, following by a final rinse with 5 mL of 2.5% NaOCl. The canals were dried with three sterile paper points, size 40/0.06 (FKG Dentaire SA). The roots were sterilized by ethylene oxide gas before root canal obturation.
All roots were randomly divided into 4 experimental groups (n = 20 of each) and 2 control groups as the positive and negative controls (n = 6 of each). Each root canal was filled with one of obturation cone/sealer, using a matched single-cone technique. Obturation cones were disinfected by immersing in 2.5% NaOCl for 1 minute followed by 70% ethyl alcohol for 1 minute. Obturation procedure was performed with an aseptic technique in sterile area.
For groups 1 (GP/AH) and 2 (BCC/AH), the root canals were obturated using AH Plus sealer, with size 40/0.06 GP (FKG Dentaire SA) in group 1 and size 40/0.06 BCC (FKG Dentaire SA) in group 2. The root canal wall was lightly coated with the mixed sealer using a master cone. The cone was then coated with the sealer and placed into the canal. For groups 3 (GP/BCS) and 4 (BCC/BCS), the root canals were obturated using BCS (FKG Dentaire SA) with size 40/0.06 GP in group 3 and size 40/0.06 BCC in group 4. Following the manufacturer's instruction, BCS in a syringe with an intra-canal tip was inserted into the canal at the coronal one-third, and a small amount of sealer was gently dispensed into the canals. The cone was coated with a thin layer of the sealer and slowly inserted into the canal to the working length. For positive control, 6 root canals were obturated with a matched single-cone of BCC or GP without any sealer, 3 of each core material. For negative control, 6 root canals were obturated with BCC/BCS or GP/AH, 3 of each, and were completely sealed with 2 layers of nail varnish on the entire root surface.
Coronal end of master cone was removed at the orifice level using an electrical heat carrier (System B Heat Source, SybronEndo, Orange, CA, USA) without further compaction into the canal. All specimens were kept in a container at 37°C with 100% humidity for 7 days to allow complete setting of the sealers.
2. Bacterial leakage model preparation
The root surfaces in four experimental groups (80 roots) and positive control group (6 roots) were sealed with two layers of nail varnish (Revlon Inc., New York, NY, USA), except 2 mm around the apical foramen.
A modified microbial leakage model using the two-chamber method was used. The upper chamber was constructed using a 1.5 mL microcentrifuge tube (Treff Lab., Schweiz, Switzerland). Each obturated root was placed into the cut tube until approximately 5 mm of the root was protruded through the cutting end, while approximately 3 mm of root remained in the upper chamber. The gaps between tube and root were sealed with a cyanoacrylate adhesive (3M Super Glue Gel, 3M Company, Maplewood, MN, USA) and nail varnish. The assembled upper chamber was sterilized with ethylene oxide gas.
For the lower chamber, a 10 mL glass vial was filled with brain heart infusion (BHI) broth (Difco Laboratories, Detroit, MI, USA) and sterilized in an autoclave (Steam Autoclave HV-110, Hirayama, Tokyo, Japan) for 20 minutes. Next, the upper-chamber (centrifuge tube) was placed into the lower chamber (glass vial). Approximately 2 mm of the root tip was immersed in BHI broth without contacting the bottom of glass vial (Figure 1).
 | Figure 1Bacterial leakage apparatus.
E. faecalis, Enterococcus faecalis; BHI, brain heart infusion; DB, distobuccal.
|
The assembled apparatus were further incubated at 37°C for 24 hours to affirm sterile condition. The apparatus was discarded if turbidity of BHI broth was observed due to a contamination.
3. Bacterial leakage test with E. faecalis
E. faecalis strain (ATCC 29212, ATCC, Manassas, VA, USA) from the frozen stock cultures was used. The entire pellet was rehydrated with 0.5 mL of BHI broth and incubated at 37°C for 24 hours. E. faecalis was maintained by sub-culturing in BHI agar. Prior to the experiment, the colonies were aseptically transferred to a 3mL tube of BHI broth and incubated at 37°C for 24 hours.
The upper chamber was filled with 0.4 mL of 24-hour growth of E. faecalis in BHI broth (0.5 McFarland, corresponding to 1 × 108 cells per mL) and incubated at 37°C during the experiment. To ensure the viability of bacteria, 24-hour growth of E. faecalis broth in the upper chamber was changed every 3 days using sterile technique. A sign of bacterial leakage was daily checked by monitoring turbidity of BHI medium in the lower chamber up to 60 days. Gram staining was carried out from BHI medium with turbidity to confirm cell morphology of E. faecalis. Bacterial growth on BHI agar was identified by appearance of smooth, cream or white colonies of E. faecalis.
Time-to-leakage (days) was determined and recorded. Non-leaked samples over the 60 days were analyzed with the event time of 60 days. Survival analysis was used to compare bacterial leakage of four experimental groups with a Kaplan-Meier survival plot and a log-rank test. A statistically significant level was set at p value < 0.05.
Micro-CT analysis
Four samples were randomly selected after bacterial leakage test from each experimental group (n = 2 of either leaked or non-leaked samples) to obtain a total of 16 samples. The samples were sterilized with ethylene oxide gas, dried and mounted on custom stubs. Each sample was fixed on a positioning stage and scanned using a high-resolution, micro-CT scanner (Bruker micro-CT, Bruker MicroCT, Kontich, Belgium). Micro-CT settings were at 80 kV, 100 µA, and an isotropic pixel size of 6 µm.
The 2D slices of axial-sections were reconstructed using NRecon software (NRecon 1.6.8.0, Bruker micro-CT) and obturation materials, dentin, gaps, and voids were analyzed using CT analyzer software (CTAn, 1.16, Bruker micro-CT), by which volume of cone/sealer, gaps and voids were calculated. The 3D visualization was created using CT volume software (CTVol 2.3.2.0, Bruker micro-CT).
RESULTS
Bacterial leakage analysis
Turbidity of broth in the lower chamber of all positive controls was detected within 24 hours from bacterial leakage. All negative controls presented the uncontaminated condition throughout the experiment. The results of bacterial leakage in the four experimental groups are presented in Table 1.
Table 1
Numbers of teeth and percentages of bacterial leakage of obturated root canals in each experimental group (n = 20 each) after exposure to Enterococcus faecalis for 60 days

The values in the column of ‘Time to leakage’ are shown as means ± standard deviations in days.
GP, gutta percha; AH, AH Plus; BCC, bioceramic-impregnated gutta percha cone; BCS, bioceramic sealer.
*Using the log-rank test (α = 0.05), no significant difference of bacterial leakage was found among the 4 groups.
![]()
Table 1 shows the number of roots and percentage of bacterial leakage after exposure to E. faecalis for 60 days. None of experimental groups completely resisted bacterial leakage. However, less than 50% of samples in each group showed turbidity of media due to the leakage. The amount of leaked samples (45%; 9 samples) was highest for groups 2 (BCC/AH) and 3 (GP/BCS), whereas a lower amount of 4 leaked samples (20%) in group 1 (GP/AH) and 5 leaked samples (25%) in group 4 (BCC/BCS) were recorded. Contaminated medium from the lower chamber was taken, and the presence of E. faecalis was confirmed in the culturing procedures.
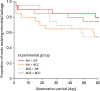
Time to leakage of samples are listed in Table 1, and Kaplan-Meier survival curves for all experimental groups are presented in Figure 2. Bacterial penetration was mostly observed at the early period of the experiment in group 2 (BCC/AH; 6 samples, within 1–20 days), whereas most of leaked samples in group 3 (GP/BCS) were detected in the middle period (4 samples, within 20–40 days). Bacterial leakage was similar in groups 1 (GP/AH) and 4 (BCC/BCS), which leaked samples were gradually presented from 1 to 60 days. Means of time to leakage were 52.40, 41.80, 46.05, and 50.25 days for groups 1, 2, 3, and 4, respectively. The shortest time of bacterial leakage detection at day 1 was observed in all groups (1 sample in groups 1, 3, and 4, and 3 samples in group 2). Using the log-rank test, there was no statistically significant difference in bacterial leakage among the experimental groups (p > 0.05).
Micro-CT analysis
From the leaked and non-leaked samples, volumes of gaps and voids (ranges of percentage) in obturated root canals are shown in Table 2. Micro-CT analysis showed very low percentages of volumes in all groups at less than 0.9%. Volumes of voids were frequently detected in coronal third of the root canals, rather than those in middle and apical third. Representative 3D images and 2D slices of axial cross-sections of obturated root canals are shown in Figures 3 and 4.
Table 2
Total gaps/voids of leaked and non-leaked samples (percentage, in range), evaluated by micro-computed tomographic analysis

GP, gutta percha; AH, AH Plus; BCC, bioceramic-impregnated gutta percha cone; BCS, bioceramic sealer.
![]()
 | Figure 3Micro-computed tomographic images in 3 dimensions of the obturated roots. Obturation cones and sealers are in the orange colour. The blue color within the obturation materials indicates gaps/voids at coronal and apical third levels. (A) Mesiodistal view; (B) Buccolingual view.
|
 | Figure 4Two-dimensional slices from micro-computed tomographic scanning of axial cross-sections of obturated root canals from coronal third to apical third level (left to right) in each experimental group. Group 1 (G1), GP/AH; Group 2 (G2), BCC/AH; Group 3 (G3), GP/BCS; Group 4 (G4), BCC/BCS.AH, AH Plus; GP, gutta percha; BCC, bioceramic-impregnated gutta percha cone; BCS, bioceramic sealer.
|
Regardless of the cone-sealer combinations, all samples displayed good adaptability to the canal walls of the obturation cones with thin layer of sealers observed along the length of root canals. Overall obturation quality among the experimental groups were not different.
DISCUSSION
None of cone-sealer combination groups completely resisted bacterial leakage throughout the experiment. Microbial leakage with an endodontic pathogen, E. faecalis, occurs in obturated teeth without intact coronal seal [2122]. However, more than half of samples in each experimental group did not present a turbidity change throughout the studied period at 60 days. It seems that bacterial seal can be adequately obtained in the well-prepared round-shaped root canals with the matched-single cone obturation technique, regardless of obturation materials. In DB-root, small canal was prepared to a final apical size 40/0.06, so that the prepared canal might have a circular shape to achieve tight seal and good adaptation with a round obturation cone. This may partly explain why there is no significant difference of sealing performance between material combination groups.
Thin layer of root canal sealer is preferred to reduce potential of leakage from shrinkage during setting or dissolving of sealer over time [23]. In general, high volume of sealer is normally presented with non-matched, single-cone obturation technique, leading to sub-optimal sealing [24]. In addition, dissolution of thick sealer layer is expected if there is coronal leakage. With the matched single-cone technique, master cone is fitted to the prepared canal especially in a round-shape canal and leaves minimal spaces for sealer. In oval or irregular-shaped root canal, poor adaptation of master cone can occur that decreases root canal sealing when using the single cone technique.
By the concept, BCS has been developed for using with BC impregnated gutta-percha cone to obtain single-unit of root canal obturation. However, sealing effectiveness of BC impregnated cone-sealer system was not superior to that of GP-sealer combinations at the determined 60-day period in this study. Even BCS has an excellent flow capacity [25], the minor gaps could still be observed in the obturated root canals from the micro-CT image. It seems that irregularities in the prepared root canals could not be completely filled with the sealer, and this might be a pathway of bacterial leakage. In contrast, the good adaptation between BCC and sealer was generally observed in the micro-CT image.
Epoxy resin-based AH Plus sealer is considered as one of the standard sealers in modern endodontics. In this study, AH Plus did not completely resist bacterial leakage, regardless of using GP cone or BCC. The results are in agreement with the previous findings, which showed bacterial penetration in root canals obturated with GP and AH Plus [1026]. Epoxy resin sealer tends to shrink during setting, and this might disintegrate adaptation and causes de-bonding from root canal wall [627]. Lack of adhesion between this sealer to GP cone might be another contributing factor associated with bacterial leakage [28]. However, the gap areas in the obturated roots were commonly present at between sealer and dentin in the micro-CT image of our study.
In this study, the period of 7 days after obturation was chosen prior to the beginning of bacterial leakage experiment. This is based on long setting time of BCS in dry condition [29]. Moreover, this period was selected to avoid the confounding effects of remaining antibacterial effects of tested sealers. BCS and AH Plus had strong antibacterial effect at the early period after setting [78], which can limit the ingress of bacteria. However, the antibacterial action did not contribute to the results of bacterial leakage in this study since the short-term antibacterial effects of sealers were diminished within 7 days after setting [78]. In this study, sealing to bacterial leakage was primarily associated to physical adaptation of obturation and might be considered as the most important factor.
Limitations must be concerned in bacterial leakage test [30]. Firstly, variations of root canal anatomy, shape and length in the obturated roots must be controlled. In this study, the sectioned single-canal DB roots with a total length of 8 mm were used in an attempt to reduce the variation. In addition, the narrow DB canals were prepared using the nickel-titanium rotary instruments up to size 40/0.06, so that the prepared root canals were uniform in circular-shape and apical size. Even though using the contralateral tooth from the same individual is the best way to control the variation, but collecting of the paired molars is not practical in our circumstance. Secondly, the bacteria used for testing should be correlated to endodontic infection, such as E. faecalis, not periodontal or other infection. Finally, bacterial leakage test should be accompanied with the other testing method to confirm the route of contamination, for instance, histological section [31] or high-resolution micro-CT [32].
In this study, micro-CT was performed to reveal gap and gap-free regions in the obturated root canals. None of the obturated canals were void or gap free. This is consistent with other previous findings, which reported detection of minor voids in all obturated root canals with different obturation techniques [323334]. Based on the results, all experimental groups displayed good adaptation of the obturation materials to root canal walls with low percentage volumes of gaps and voids. Small round-shape canals like DB canal tend to achieve a fit of obturation cone in 3D with thin sealer layer. In addition, distribution and penetration of sealer into dentinal tubules was expected by the hydraulic force when placing a fit cone into the canal. Adequate obturation quality in all experimental groups is likely to have a positive effect to sealing performance [3536]. This can explain indifferent bacterial leakage results with the low amount of leaked samples among the experimental groups.
Correlation between gaps and bacterial leakage might be expected [31]. However, gap formation was usually found in the coronal portions of the obturated root canals from the micro-CT images. In contrast, few gaps were observed in the apical portion of root canals. In addition, these gaps were commonly interrupted and not along the obturated root canals. Basically, bacterial leakage could occur through the pathway from the coronal to apical portion. It seems that there were still some minute gaps undetected by micro-CT since the resolution of micro-CT scanner in our study was not able to detect a gap that was smaller than 10–20 μm.
Further studies are needed to verify long-term sealing ability of BC materials. In this study, 60-day period was chosen since it was practical with less chance of contamination and enough to detect early-stage leakage. However, more than half of specimens were still not leaked at 60 days. Interestingly, chemical adhesion between BCC and BCS [37] might be helpful in resisting the long-term leakage, which would be superior to the conventional obturation material. Bacterial leakage test with a longer period should be further studied. In addition, it is beneficial to extend in vitro testing to oval-shaped root canal or other obturation techniques to confirm their benefit on sealing ability.
Finally, it must be considered that the clinical implication from bacterial leakage test is limited. From the in vitro study, amount of leaked bacteria causing the turbidity of medium would be varied from hundred to million. The result was then reported as the leaked sample of root canal obturation material. This limitation of laboratory-based microbial leakage studies does not completely predict the occurrence of periradicular inflammation in clinical situations. Leakage of bacteria into filled root canal does not always induce a periapical disease [38]. It depends on amount and virulence of bacteria as well as immunological response of patient. Clinical studies are necessary to confirm the application of BC materials using the matched-single cone obturation technique.
CONCLUSIONS
Within the limitations of this study, root canal obturation with BC or GP master cone in combination with BC or AH Plus sealer using matched-single cone technique showed no difference in bacterial leakage and 3D obturation quality in round-shaped canals at 60 days. BCC-sealer system was not superior to conventional GP/epoxy resin-based sealer in terms of resistance to leakage and 3D compaction.
 XML Download
XML Download