

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The number of patients undergoing orthodontic treatment has been increasing with time,1 and a major concern for patients is the pain during orthodontic treatment.2 Studies have shown that 71% of study participants experience some degree of pain, regardless of the type of orthodontic appliance.3 Similarly, studies have reported that 91–95% of patients experienced pain when the orthodontic treatment was being performed.456 Patients also reported pain as one of the main reasons for fear and anxiety before the commencement of orthodontic treatment.7 Various types of discomforts experienced by the patients were categorized as pressure, strain, stress, and pain.8
Previous studies have investigated the pain experienced with respect to different orthodontic appliance treatments. Stewart et al.9 and Sergl et al.10 identified that greater levels of pain are reported with fixed orthodontic appliances than with removable appliances. Furthermore, studies have evaluated the intensity of pain after bonding different types of brackets. Miles et al.11 revealed greater comfort with self-ligating brackets than with conventional twin brackets. Similarly, Pringle et al.12 found that patients with passive self-ligating brackets reported significantly lower pain intensity than did those treated with Tru Straight brackets (Ormco Europe, Amersfoort, The Netherlands). Tecco et al.13 also observed significantly reduced pain with the use of self-ligating brackets than with the use of conventional brackets during orthodontic treatment.
On the other hand, Scott et al.14 found no difference in the perception of pain associated with self-ligating brackets and conventional fixed appliance brackets. Similar results were reported by Fleming et al.15 who discovered no difference in pain experience after 4 hours through to 7 days following the bonding of self-ligating and conventional pre-adjusted brackets. However, they observed more discomfort during the insertion and removal of archwires with self-ligating brackets. A recent study by Rahman et al.16 showed that patients treated with self-ligating (3M SmartClip; 3M Unitek, Monrovia, CA, USA) brackets experienced statistically higher pain than did patients treated with a conventional (3M Victory; 3M Unitek) bracket system. These authors concluded there was no clinical difference in pain perception among patients treated with both appliance systems.16
Similar findings were reported by Bertl et al.17 in a split-mouth design study, wherein engagement and disengagement of archwires caused more pain with self-ligating brackets (SmartClip) than with fixed conventional brackets. Increased pain with self-ligating brackets than with conventional brackets can result from full-size manipulation and the method of wire ligation and insertion associated with the design of SmartClip.17
Invisalign® aligners (Align Technology, Santa Clara, CA, USA) offer enhanced aesthetics, reduced pain, and improved oral hygiene during orthodontic treatment.1819 Moreover, a reasonable body of evidence is available on the discomfort and pain experienced by patients treated with Invisalign and fixed orthodontic appliances.182021 Previous studies have investigated patients' experience of pain with Invisalign and conventional fixed orthodontic treatments, including lingual fixed appliances.182021 Similarly, a recent study found greater discomfort and higher consumption of analgesics with conventional fixed brackets than with Invisalign aligners.22
Passive self-ligating brackets have minimal frictional resistance than do conventional and active self-ligating brackets.23 Therefore, self-ligating brackets are assumed to cause less pain than do conventional brackets. In addition, patients treated with conventional fixed brackets, self-ligating brackets, and Invisalign aligners demonstrated different intensity of pain and discomfort during initial orthodontic treatment. However, limited evidence is available on the pain perception of patients treated with Invisalign and passive self-ligating fixed appliances. Therefore, the primary objective of this research was to compare the perception of pain among patients treated with passive self-ligating fixed appliances and Invisalign aligners. The secondary objectives included observing the intensity and duration of pain during the initial phase of treatment, and reporting the use of analgesics for the relief of orthodontic pain.
MATERIALS AND METHODS
Study design, participants, and sample size calculation
A prospective study was conducted using a calculated sample of 64 participants. The sample size estimation involved assuming 0.05 alpha, 0.20 beta, and 80% power of the study, with minimal relevant difference in the groups and variability of the outcome.24 One group of 32 participants was treated with passive self-ligating fixed appliances (Damon Q; Ormco, Orange, CA, USA), and the other group of 32 participants received Invisalign aligners. The participants were recruited from a private dental clinic.
Adult patients were included in this study as long as they had no deciduous teeth, no previous orthodontic treatment, no missing teeth, were free from mucosal and periodontal diseases, demonstrated good general health, had mild to moderate crowding (Little's irregularity index [LII] between 3 and 5), and Class I molar relationship. The expression of pain can be affected by emotional and cognitive factors, family surrounding and behaviors, and other influences.2526 Patients who exhibited dental anxiety and were on psychotropic drugs were excluded from the study. In addition, hygienists, dentists, and dental students were excluded from the study because of their knowledge of pain during their orthodontic treatment. The patients undergoing passive self-ligating fixed appliance therapy and Invisalign treatment who were willing to participate in the study were recruited from the respective clinic. In this prospective interventional comparative clinical trial, participants received orthodontic treatment from an experienced orthodontist, who offered both types of treatments to his eligible patients and administered a close-ended and coded self-administered questionnaire to the study participants.
Outcome measurement instruments
The visual analog scale (VAS) is the most commonly used instrument in scientific research as it allows using parametric tests.27 Therefore, the patients' pain experience was assessed using a VAS in the form of an unmarked 10-cm horizontal line with “no pain” at its left end (score 0) and “very severe pain” at its right end (score 100). The assessor of the VAS was blinded to minimize the bias in the measurement of pain. Both groups were in the initial alignment stage of orthodontic treatment. The patients treated with passive self-ligating fixed appliances had an initial archwire (0.014-inch copper nickel-titanium) while those treated with Invisalign aligners were provided initial-stage aligners (first aligners). In both groups, the patients had minimal to moderate crowding, which was assessed using LII (range, 3–5).
A previous study recorded the pain experiences of patients treated with self-ligating appliances and conventional fixed braces at 4 hours, 24 hours, day 3, and day 7.15 Therefore, after fitting the orthodontic appliance, each patient was asked to place a mark on the line that best matched the level of pain he/she experienced at 4 hours, 24 hours, day 3, and day 7. The mark was measured using a millimeter scale to record pain intensity, and a value ranging from 0 to 100 was recorded. The pain was recorded for 1 week after initial appliance therapy, because a previous study reported no pain after initial orthodontic treatment for 7 to 9 days.13 In addition, other studies reported the presence of pain in the first week of orthodontic treatment.828 The study participants also responded to the questionnaire about the type and frequency of analgesics used, if any, to relieve pain.
Ethical considerations
The study protocol was approved by the Institutional Review Board of the Imam Abdulrahman Bin Faisal University, Dammam (IRB-2017-02-154). The study participants were informed about the possible risks and benefits of participating in the comparative clinical trial. The investigator ensured that participants understood the purpose and methods of the study by informing them individually. The participants were briefed about their voluntary participation in the study and their right to withdraw from the research. Similarly, the privacy and confidentiality of the participants were assured, and finally, those willing to participate gave their written informed consent.
Statistical analysis
Data from the VAS and questionnaire were transferred to a spreadsheet and analyzed using IBM SPSS Statistics for Windows, version 22.0 (IBM Co., Armonk, NY, USA). The Mann-Whitney U-test was performed to compare the mean ranks of the VAS scores between the two groups of participants. The Kruskal-Wallis test was performed to observe the differences in VAS scores among all the participants at 4 hours, 24 hours, day 3, and day 7. Pearson's chi-square test (or Fisher's exact test as appropriate) was used to observe the differences between the two groups of participants in the use of analgesics and the intensity of orthodontic pain at different time intervals. Statistical significance was set at p-value ≤ 0.05.
RESULTS
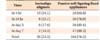
The mean age of the study population was 26 years (standard deviation, ± 7.31). The patients included 22 men (34.4%) and 42 women (65.6%) (Table 1). Table 2 demonstrates the presence of pain between the groups at different intervals in the first week of orthodontic treatment. A lower percentage of patients treated with Invisalign aligners reported pain than did those treated with passive self-ligating fixed appliances at 4 hours, 24 hours, day 3, and day 7, and these differences were statistically significant (p = 0.001). Overall, the largest number of participants (n = 44) reported having pain at 4 hours, and the lowest number (n = 19) experienced pain on day 7.
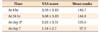
The comparison of pain levels in the two groups at different time intervals is presented in Table 3. Patients treated with Invisalign aligners had significantly lower pain levels (mean VAS scores) than did those treated with passive self-ligating fixed appliances at 4 hours, 24 hours, day 3, and day 7 (p = 0.001). The highest pain levels for both groups of patients were recorded at 24 hours (mean VAS scores of 1.38 and 6 for the Invisalign aligner and passive self-ligating fixed appliance groups, respectively) after the initial placement of orthodontic appliances.
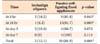
The Kruskal-Wallis test was performed to observe the difference in pain among all patients in both treatment groups (Table 4). The mean VAS scores for all participants at different time intervals during the first week of orthodontic treatment also showed statistically significant differences (p = 0.001). The highest mean VAS score (3.68) among the study participants was observed at 24 hours.
Table 5 shows the use of analgesics (acetaminophen/paracetamol) among the study participants. Fewer participants with Invisalign aligners used analgesics at 4 hours and 24 hours than did those treated with passive self-ligating fixed appliances, and these differences were statistically significant. No participant treated with Invisalign aligners reported taking analgesics on day 7. The highest number of participants (n = 12) used analgesics at 24 hours, and four consumed analgesics at day 7. Compared to 28 patients (84.8%) treated with passive self-ligating fixed appliances, only five (15.1%) treated with Invisalign aligners took analgesics.
DISCUSSION
This study found that a greater proportion of patients treated with passive self-ligating fixed appliances reported pain than did patients treated with Invisalign aligners. Similarly, the intensity of pain recorded using the VAS was higher in the passive self-ligating fixed appliance group than in the Invisalign group. For both groups, the intensity of pain progressively decreased during the first week of fitting the orthodontic appliances. Moreover, the use of analgesics was lesser among patients treated with Invisalign aligners than among those treated with passive self-ligating fixed appliances.
Previous studies have compared the intensity of orthodontic pain after the insertion of different orthodontic appliances. Bondemark et al.29 compared the level of pain associated with the use of elastomeric and spring separators and observed the highest degree of pain occurring on day 2 and disappearing by day 5. Jones30 stated that the pain was experienced at 4 hours after the placement of an archwire, reached its peak at 24 hours, and then steadily declined. Jones and Chan28 reported maximum pain on the morning after archwire insertion and it continued until day 5 or day 6 of the treatment. A recent study by White et al.22 found that pain peaked between the first and third days of conventional treatment and gradually decreased over the fourth and fifth days. However, some studies have found no significant differences in the prevalence, intensity, frequency, and duration of pain with orthodontic treatment using different archwires.3132
In the present study, the highest number of patients reported pain at 24 hours after fitting the passive self-ligating fixed appliance, and the largest number of patients treated with Invisalign aligners experienced pain at 4 hours. These findings are inconsistent with the results of Shalish et al.20 who found that the highest percentage of participants in the Invisalign group reported pain on day 1. These authors described that the application of greater mechanical force in the Invisalign group and the use of a flexible wire and lighter force in the conventional buccal group during the first week of treatment could have accounted for the difference in pain.20
Although the mean VAS scores for both appliances in the present study were highest at 24 hours, a statistically significant difference was observed between the two groups. Fujiyama et al.21 compared the VAS scores among three groups of patients and found the peak VAS score at 24 hours. Shalish et al.20 reported the highest mean pain score on day 1 of treatment with buccal fixed appliances and on day 2 for the Invisalign group. White et al.22 observed similar patterns of discomfort that peaked after the first day and decreased over the week in both the conventional appliance and aligner groups. Increased pain or discomfort within the first 24 hours of the placement of orthodontic appliances could result from an acute inflammatory response to the orthodontic forces.33
Miller et al.18 found that patients experienced reduced pain with Invisalign aligners than with fixed appliances during the first week of orthodontic treatment. Later, Shalish et al.20 compared the pain levels among three groups of patients: the first group received lingual fixed appliances, the second received buccal fixed appliances, and the third received Invisalign aligners; the most severe level of pain was observed with the lingual appliance. Fujiyama et al.21 evaluated the perception of pain among three groups of patients: one group received Invisalign aligners, the second group was treated with conventional fixed orthodontic appliances, and the third group received both Invisalign aligners and fixed appliances. The intensity and duration of pain during the initial stages of treatment were pointedly lower among patients treated with Invisalign aligners than among those treated with an edgewise orthodontic appliance. Similarly, White et al.22 also indicated that patients treated with conventional appliances had significantly higher pain than did patients treated with aligners during most of the first week of orthodontic treatment.
In accordance with the findings of previous studies, the findings of this study revealed that patients treated with Invisalign aligners had significantly lower perception of pain than did those treated with passive self-ligating fixed appliances during the first week of treatment. The high acceptance of the Invisalign system could be attributed to the great adaptability of patients to the appliance and high satisfaction with the progress and result of treatment.34 Moreover, previous studies have shown that Invisalign aligners have lower irregularity and complexity indexes than do buccal fixed appliances, and this might minimize the patients' perception of pain with Invisalign aligners.20 Significantly lower pain in the Invisalign group than in the passive self-ligating fixed appliance group in the present study, could be because the attachments placement were delayed until commencing the insertion of the third set of aligners.
The use of analgesics was related to the intensity of pain in our study, as more patients treated with passive self-ligating fixed appliances used them than did those treated with Invisalign aligners. At 24 hours, more patients treated with passive self-ligating fixed appliances used analgesics than did those treated with Invisalign aligners, and the difference was statistically significant; moreover, no patient in the Invisalign group took analgesics on day 7 of the treatment. A similar pattern of analgesic use was reported by Shalish et al.,20 with the highest intensity of pain being observed on day 1 of the treatment with fixed orthodontic appliances and no analgesic consumption being reported until day 6 in patients treated with Invisalign aligners. Miller et al.18 also found that 67% of patients treated with fixed appliances took analgesics as compared to 42% of patients treated with Invisalign aligners. White et al.22 reported that a greater proportion of patients in the conventional group took pain medication than did patients in the aligner group. The highest percentage of patients in the aligner group consumed pain medication on the first day, while the greatest percentage of patients in the traditional group consumed pain medication on the second day.22
In the present study, appropriate sample size calculations were performed. Both groups had a similar degree of crowding, and patients in both groups were in the first stage of initial alignment. These measures may have helped ensure similar amounts of tooth movement in both groups. The patients in the Invisalign and passive self-ligating fixed appliance groups were matched for age, sex, and degree of crowding. Moreover, patients in both groups received treatment by an experienced orthodontist; hence, their pain perception could not have been influenced by the treatment received from an inexperienced orthodontist or any variable related to variation among orthodontists. Similarly, the assessor was blinded during the evaluation of the patients' responses to reduce the bias in this study. In addition, inclusion and exclusion criteria were applied to recruit the most suitable participants and to obtain valid study results. All the efforts were made to ensure that both groups were similar in all areas other than the different interventions. However, the limitation of the study may be the non-randomization of participants to the interventions. In accordance with previous studies,1535 the present study evaluated pain during the first week of orthodontic treatment. Nevertheless, reporting of pain after subsequent monthly appointments could have provided more meaningful data. Further, as the participants were recruited from a private dental clinic, it is likely that more affluent patients were represented in the study. Future studies should include study participants from both private and government dental clinics.
CONCLUSION
The patients treated with Invisalign aligners observed significantly lower pain than did those treated with passive self-ligating fixed appliances. The intensity of pain was the highest at 24 hours and diminished to the lowest levels by day 7 in both groups of patients. The patients treated with Invisalign aligners reported a lower intensity of pain than did those treated with passive self-ligating fixed appliances during the first week of orthodontic treatment. The use of analgesics also peaked at 24 hours; however, fewer patients treated with Invisalign aligners were found to use medication to relieve their pain.


 XML Download
XML Download