

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease with diverse clinical manifestations involving variable tissues and organs, such as the skin, hematologic system, cardiovascular system, lungs, musculoskeletal system, and kidneys.1 Recent studies have provided evidence that physical activity should be considered as a crucial factor in understanding disease progression, manifested as disability, fatigue, and quality of life in patients with SLE.2345 Considering the effect of physical activity on disease activity or damage, physical activity was found to be related with an increased risk of organ damage, but not disease activity.67 In contrast, low aerobic activity was not found to be correlated with overall disease activity and organ damage.8 Multiple studies have shown a prevalence of less physical activity in 23–59% of patients with SLE.291011 Given the evidence linking physical activity and unfavorable SLE-related clinical progression, defining the effect of physical activity on disease status in SLE patients should be of great importance.
Various methods have been developed to measure physical activity. Early studies in patients with SLE used self-reported estimates. The International Physical Activity Questionnaire (IPAQ)212 or accelerometer measures1213 were used according to the purposes of each study. Comparing the two methods to assess their association in SLE patients, Ahn, et al.12 concluded that the IPAQ was useful to provide descriptive data and was modestly correlated with accelerometer measurements. This study also suggested that an accelerometer may be helpful in detecting changes in physical activity in therapeutic intervention trials. However, these two estimates have limitations: subjective responses, abdominal adiposity, underestimated reporting in activities, such as swimming and bicycling, and cost-effectiveness in large population studies.
There is insufficient data about the relationship between physical activity and disease activity/organ damage in SLE patients, although debate over this issue remains.678 In our cross-sectional study, we used self-reported IPAQ estimates to investigate the association between physical activity and SLE-specific disease activity/organ damage measurements in patients with SLE.
MATERIALS AND METHODS
Subjects
Patients enrolled in the KORean lupus Network (KORNET) registry were consecutively recruited from rheumatology outpatient clinics at four university-based medical centers between January 2014 and December 2015. A total of 505 patients with SLE who met the 1982 revised and 1997 updated American College of Rheumatology classification criteria for SLE1415 were initially identified from this registry. However, only 415 SLE patients were enrolled in this study: 90 patients were excluded for failure to complete the questionnaire on self-reported measured physical activity. All patients provided written informed consent for enrollment in the registry. The Institutional Review Board of all four medical centers approved the registry protocol (IRB No. CR-14-123-L).
Clinical data collection
The KORNET registry collected clinical information through medical record review and interviews with each patient. Upon enrollment in the KORNET registry, each patient's demographic data and health behaviors, such as smoking and alcohol consumption, were recorded. Body mass index, marital status, and education duration were identified. Questionnaires related to health status were also assessed using Beck's Depression Inventory16 and the 36-item Short Form Health Survey (SF-36).17 Serologic markers included in this study were erythrocyte sedimentation rate (mm/hr), C-reactive protein (mg/dL), complement 3 (mg/dL), complement 4 (mg/dL), and CH50 (U/mL). Positivity for anti-double stranded DNA (anti-dsDNA) antibody was also identified. In addition, anti-rheumatic medications being taken at the time of enrollment, such as hydroxychloroquine, corticosteroids, methotrexate, azathioprine, mycophenolate mofetil, and tacrolimus, were recorded. Enrolled patients with hypertension, ischemic heart disease, myocardial infarction, congestive heart failure, and/or a cardiac arrhythmia were defined as having cardiovascular disease (CVD). The definitions for each CVD were as follows: Hypertension was diagnosed if diastolic blood pressure was over 90 mm Hg or systolic blood pressure was 140 mm Hg or more when not taking or if taking anti-hypertensive medicine. Ischemic heart disease included stable or unstable angina pectoris based on clinical features or laboratory findings. Myocardial infarction was defined as a non-ST segment elevation or ST segment elevation myocardial ischemia diagnosed by abnormal changes in electrocardiogram, chest pain, and elevated cardiac enzymes. Congestive heart failure was diagnosed by echocardiography and clinical findings related with impaired heart function. Cardiac arrhythmia included premature heartbeat, tachyarrhythmia, or bradycardia identified by electrocardiogram.
SLE-related disease activity using the SLE Disease Activity Index 2000 (SLEDAI-2K)18 and organ damage using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index (SDI)19 were evaluated by a rheumatologist (SK Kim). According to disease activity and organ damage scores, this study was classified into two groups: inactive (SLEDAI<2) versus active (SLEDAI≥2) and non-damaged (SDI<1) versus damaged (SDI≥1). The Charlson comorbidity index (CCI) score is defined as the sum of the comorbidity scores.20 CCIa is age-adjusted value of CCI.
Assessment of physical activity
The IPAQ, developed by the World Health Organization in 1998 (https://sites.google.com/site/theipaq/scoring-protocol), was utilized as a self-reported questionnaire for physical activity surveillance.21 For recording physical activity for seven days, patients used the 7-item short-form IPAQ instead of the 27-item long form. A Korean version of the short-form IPAQ has been confirmed through validation against both the long-form IPAQ and accelerometer measurements.22
Metabolic equivalent of task (MET) values and formula for computation of MET-minutes/week were measured from the IPAQ assessment. The short-form IPAQ was categorized as follows: walking MET-minutes/week (3.3×walking-intensity activity minutes×walking-intensity days), moderate MET-minutes/week (4.0×moderate-intensity activity minutes×moderate-intensity days), and vigorous MET-minutes/week (8.0×vigorous-intensity activity minutes×vigorous-intensity days).23 Total physical activity MET-minutes/week was the sum of walking, moderate, and vigorous MET-minutes/week scores. In addition, we assigned three categorical scores: category 1 low, category 2 moderate, and category 3 high, according to levels of physical activity.
Statistical analysis
Statistical analysis for continuous variables was assessed by two normality tests: the Kolmogorov-Smirnov and Shapiro-Wilk tests. The data were not normally distributed and were described as median±interquartile range (IQR) for continuous variables. For categorical variables, data are expressed as a number (%). The statistical differences between two groups [lupus nephritis (LN) (+) vs. LN (−), CVD (+) vs. CVD (−), SLEDAI-2K<2 vs. SLEDAI-2K≥2, and SDI=0 vs. SDI≥1] were calculated using the chi-square test or Fisher's exact test for categorical variables and the Mann-Whitney U test for continuous variables. Binary logistic regression analysis was used to determine risk factors related to LN and CVD. All statistical analyses were conducted using IBM SPSS Statistics 19.0 (IBM Corp., Armonk, NY, USA). Statistical significance was considered at a p value less than 0.05.
RESULTS
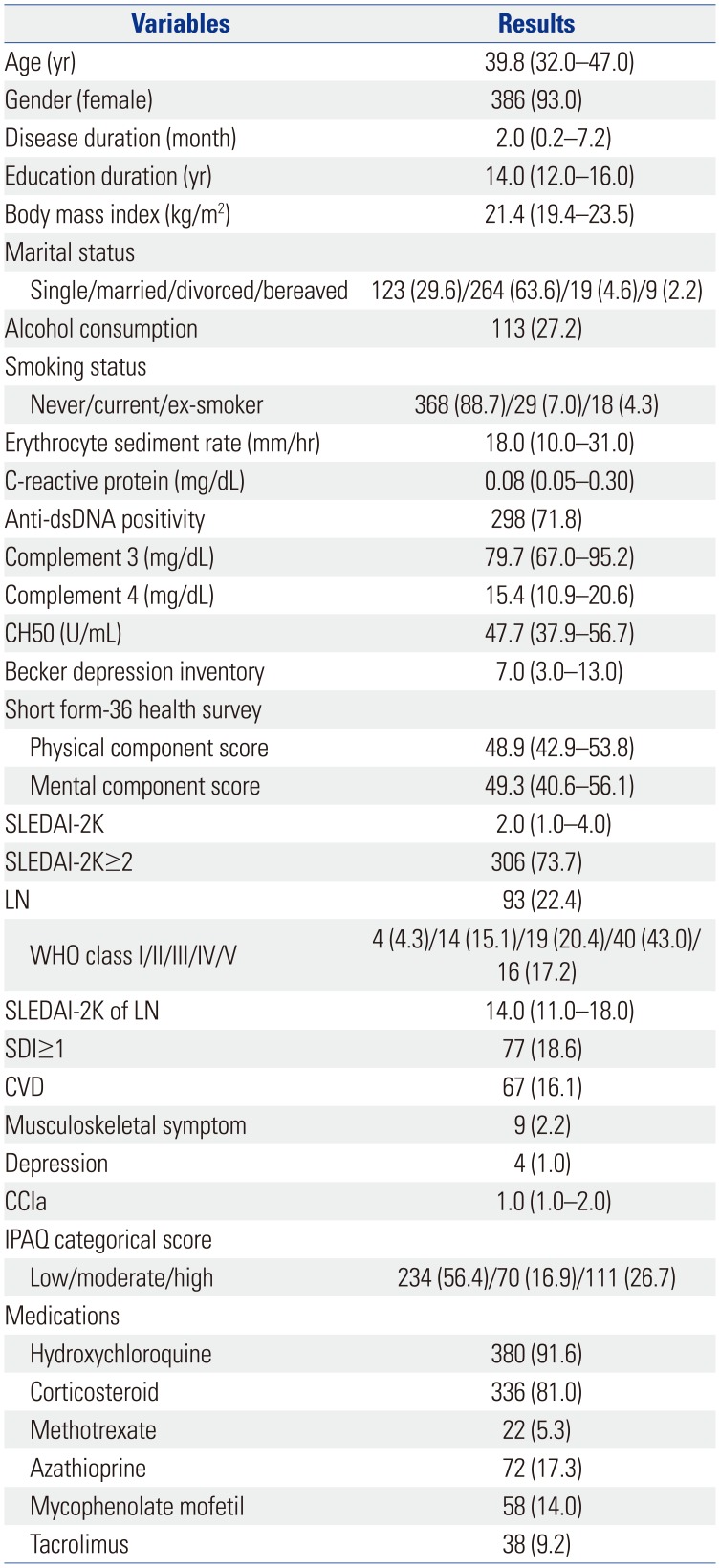
Table 1 shows the baseline demographic data, clinical features, and laboratory findings in the 415 SLE patients. Median age at enrollment was 39.8 years (IQR 32.0–47.0) and 93.0% were female (n=386). Notably, 93 patients with LN (22.4%) were identified, all of whom were pathologically diagnosed in the course of the disease. Median SLEDAI-2K of all patients was 2.0 (IQR 1.0–4.0). The percentage of patients with SLEDAI-2K≥2 and with at least one organ damaged (≥1 of SDI) was 73.7% (n=306) and 18.6% (n=77), respectively. In total, 16% of patients (n=67) had at least one manifestation of CVD.
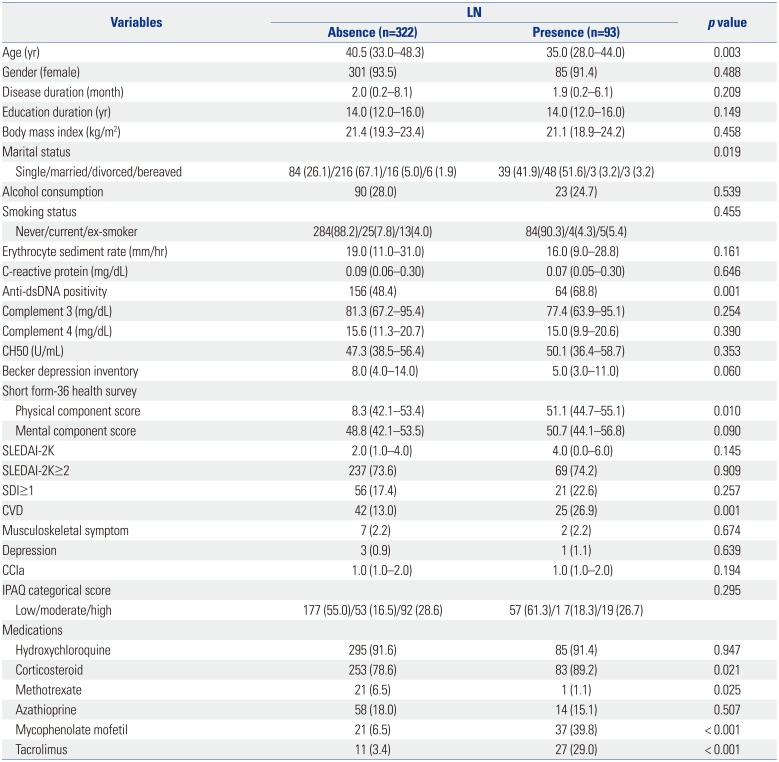
Comparison of characteristics between patients with and without LN is illustrated in Table 2. There were significant differences in age, marital status, anti-dsDNA positivity, physical component summary of SF-36, frequency of CVD, and use of corticosteroid, methotrexate, mycophenolate mofetil, and tacrolimus between the two groups. However, the frequency for some disease activity and damage-related variables including SLEDAI-2K ≥2 and SDI ≥1 were similar between the two groups.
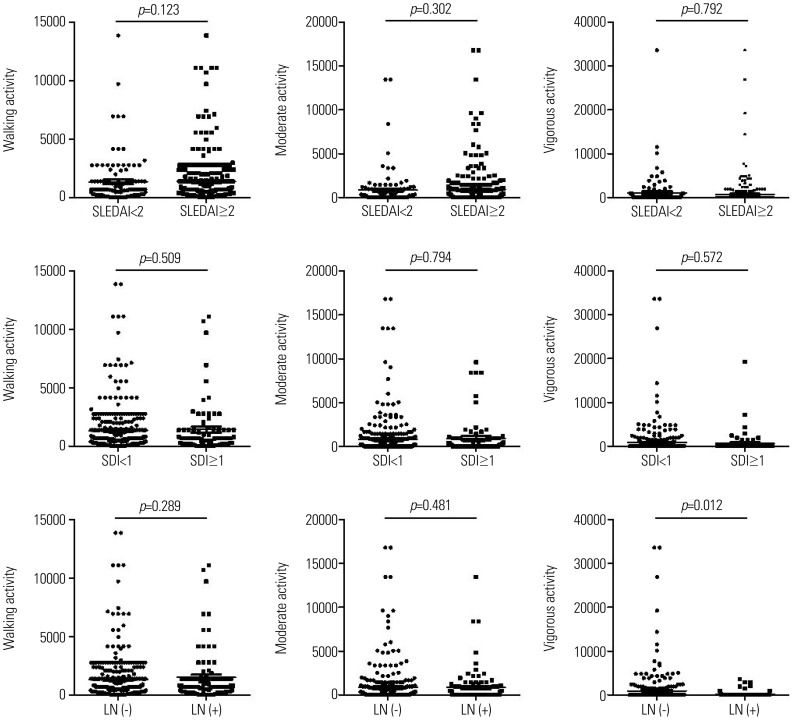
The differences in physical activity based on IPAQ scores according to SLEDAI-2K (<2 vs. ≥2), SDI (<1 vs. ≥1), and LN (presence vs. absence) were assessed (Fig. 1). There were no significant differences in walking, moderate, and vigorous physical activity between active (SLEDAI-2K≥2) and inactive (SLEDAI-2K<2) (p>0.05) patients. Similarly, there were no differences in each physical activity score between organ-damaged (SDI≥1) and non-organ-damaged (SDI<1) (p>0.05) patients. Walking and moderate activity showed similar levels despite the presence or absence of LN. However, patients with LN showed less vigorous activity, compared to those without LN (p=0.012). In addition, there were no differences in numbers of patients in low, moderate, and high categories between patients with and without LN (p>0.05). Patients with CVD also showed similar levels of each physical activity score, compared to those without CVD (p>0.05 of all, data not shown).
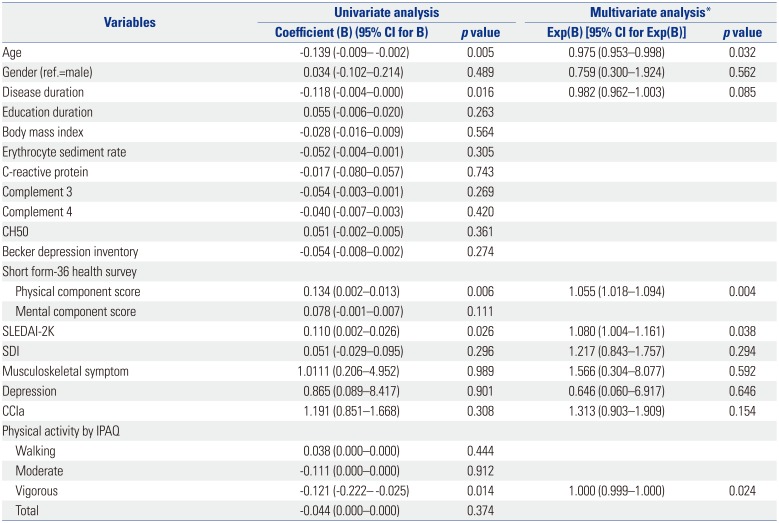
Logistic regression analysis was performed to determine the risk factors associated with LN (Table 3). Younger age, shorter disease duration, higher physical component score (PCS) of SF-36, higher SLEDAI-2K, and less vigorous physical activity were significantly associated with the presence of LN in univariate logistic regression analysis. However, multivariate logistic regression analysis showed that younger age, higher PCS of SF-36, higher SLEDAI-2K, and less vigorous physical activity were associated with LN. Age, gender, and BMI were noted to be related to CVD in multivariate logistic regression analysis (data not shown). Remarkably, physical activity measured by the IPAQ estimate was not related to CVD.
DISCUSSION
Studies have established that physical activity could be limited by a high level of disease activity, poor functional disability, and organ damage in patients with SLE.2567 Nevertheless, there has been insufficient data about the relationship between physical activity and clinical features in SLE patients. The main objective of this study was to clarify an association between physical activity assessed by the IPAQ scores and disease activity/organ damage in SLE patients. We observed that physical activity was not associated with SLE-specific measures like SLEDAI and SDI. However, patients with LN were shown to perform less vigorous physical activity, compared to those without LN.
There is evidence of a close relationship between physical inactivity and high disease activity or specific organ involvement in patients with SLE. Several clinical studies have revealed that exercise or regular physical activity, without the interference of disease activity, improves quality of life, fatigue, and other SLE-related symptoms.524 Eriksson, et al.7 demonstrated less low to moderate intensity physical activity in SLE patients with SDI ≥2, compared to matched controls. In contrast, they did not find a significant difference in physical activity between patients with high disease activity (SLEDAI>5) or low disease activity (SLEDAI≤5) and controls. Two different 12-week randomized trials in small populations with SLE demonstrated no significant changes in disease activity after an exercise training program.2526 Although there was a marked difference in cutoffs for SLEDAI and SDI scores compared to a former study,7 this study failed to confirm the difference of physical activity based on IPAQ scores. The beneficial role of exercise and physical activity in SLE-related disease activity or organ damage should be confirmed in a larger study population.
Physical activity is an independent risk factor for CVD in the general population. Regular physical activity has beneficial health effects and also contributes to decreased mortality risk and development of morbidity.27 The data from the Framingham Heart Study indicate that moderate to high physical activity leads to increased total and CVD-free life expectancy, compared to low physical activity.28 Premature CVD is attributed as the most common cause of mortality in SLE patients affected by the disease for over 5 years.29 Earlier studies on physical activity have primarily focused on the risk of CVD in SLE patients.630 A multicenter inception cohort study found low physical activity level (score<28) to be a potent risk factor for coronary artery disease in 278 SLE patients who were followed for 3 years (71.6% increased risk from enrollment).6 Volkmann, et al.30 demonstrated that physical activity, assessed from self-reports by calculating METS per week, was negatively correlated with carotid intima-media thickness and number of carotid plaques, thus implicating the harmful effect of low physical activity on subclinical atherosclerosis in SLE. Subsequently, they recommended increased exercise to reduce the risk of atherosclerosis in SLE patients. These findings might be compatible with a sedentary lifestyle as a traditional risk factor for CVD in general.31 SLE-induced cognitive impairment has been known to be caused by multiple complex factors, such as inflammation and lower energy expenditure. Physical inactivity coupled with obesity was associated with an increased risk of cognitive dysfunction in female patients with SLE.2 We found no association between physical activity and the risk of CVD disease in this study. Based on these results, future studies identifying the role of physical activity and other lifestyles in the risk of CVD are warranted.
LN is the most debilitating manifestation of SLE and is associated with increased morbidity and mortality.1 The pathogenesis of LN is well understood: formation of glomerular immune complexes, B cell activation with autoantibodies, and inflammatory mediators.32 Although the precise mechanism for the favorable effect of physical activity has not been clearly determined, there is evidence that physical inactivity could induce an increased inflammatory response. Prolonged murine restraint stress induced changes in inflammatory cytokine profiles, increasing IL-6 and reducing IL-10, indicating an enhanced inflammatory cascade.33 In contrast, daily moderate exercise attenuated systemic inflammation in response to lipopolysaccharide injection in mice.34 Recently, Aqel, et al.35 demonstrated that daily moderate exercise improves the inflammatory response of LN in NZM2410/J mice through blocking the expression of inflammatory mediators IL-6, tumor necrosis factor-α, CXCL1, and anti-dsDNA antibodies. Their findings also implicated the possibility of adjunct therapeutic strategy for LN. Compatible with these observation, we found that patients with LN performed less vigorous physical activity.
There are several limitations that should be considered to understand this result. First, this study used only self-reported IPAQ estimates to assess levels of physical activity. Because our study contained a large number of patients, we could not perform objective measurements with an accelerometer. The IPAQ estimate has some advantages in studies that enroll many patients and also for acquisition of discriminable data related with the types of each physical activity, whereas estimation using an accelerometer is not cost-effective. Overall, moderate correlation between self-reported and objectively measured physical activity was confirmed through a cross-sectional study that included 129 patients with SLE.12 Second, healthy and disease control groups were not included in this analysis. Approximately 56% of patients were classified into the low category in the assessment of physical activity in our registry, which is consistent with earlier evidence showing less physical activity in patients with SLE.910 Control groups with inactive, healthy subjects are needed to compare the levels of physical activity in patients with SLE. Third, our results were acquired through cross-sectional analysis. Therefore, we could not identify whether enforcement of physical activity hinders disease activity and lessens organ damage measured through SLEDAI and SDI. Some debate over the effect of therapeutic intervention through a regular exercise program or physical activity on SLE-related symptoms and disease activity remains.5242526 The possibility for exercise and physical activity as therapeutic modalities should be assessed in a prospective study. Considering 90 patients were excluded with missing data for physical activity, the study population may lack representativeness. Patients with a high disease activity or severe disease impairment may be less willing to participate in the questionnaire for physical activity. Excluding such patients who do not complete the questionnaire introduces a high likelihood of selective bias. In addition, physical activity according to disease activity or severity may be underestimated as a result of this study.
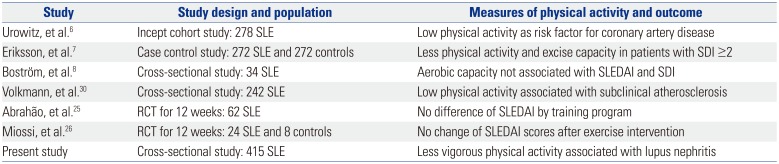
There is still debate over the effect of physical activity in the clinical status of patients with SLE (Table 4). Using the self-reported questionnaire IPAQ, this study was performed to identify the associations between physical activity and disease activity and organ damage in a population of patients with SLE. We found that patients with LN showed no difference in walking and moderate physical activity, compared to patients without LN. Patients with LN also tended to be reluctant to conduct vigorous physical activity. Efforts to strengthen the intensity of physical activity should be encouraged to avoid incremental exposure to SLE-related morbidity and mortality.
 XML Download
XML Download