

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Malignant hilar biliary obstruction (MHBO) is reported in a variety of cancers, including cholangiocarcinoma, gallbladder cancer, pancreatic cancer, and stomach cancer. There are several complications related to biliary obstruction, such as jaundice and cholangitis. Proper management of these complications is important to improving the prognosis of patients with MHBO. Endoscopic biliary drainage with metallic stents has been performed for managing those complications, due to its minimal invasiveness and long-term patency, compared to drainage with plastic stents.1 Recently, bilateral biliary decompression with self-expandable metallic stents (SEMSs) has been considered a favorable palliative procedure for unresectable MHBO.23
Bilateral stent-in-stent (SIS) SEMS placement is physiologic and currently favored by endoscopists despite its technical difficulty. Bilateral drainage also offers advantages in preserving functional volume of the liver and prolonging stent patency.4567 SIS placement involves contralateral placement of a second SEMS through the mesh of the first deployed stent to achieve a physiological Y configuration.8 In terms of SIS method for endoscopic bilateral metallic stenting in MHBO, previous studies have reported various stent patency durations (median patency duration, 140–240 days).69101112131415 However, endoscopists have frequently reported experiencing occlusion of Y-shaped metal stents in patients receiving metal stents via the SIS method for high-grade MHBO.10111617
A few studies have delved into risk factors related to stent occlusion in patients using the SIS method; however, these studies only analyzed a small number of patients with biliary obstruction. Accordingly, we reviewed MHBO patients from two large-volume centers to investigate stent patency duration with SIS method, as well as risk factors associated with stent patency.
MATERIALS AND METHODS
Patients
We analyzed patients with MHBO who underwent bilateral SIS placement with SEMSs between 2009 and 2016 at two tertiary hospitals in South Korea (Severance Hospital and Seoul National University Hospital). We included 16 patients from Severance Hospital and 54 patients from Seoul National University Hospital with unresectable MHBO using Bismuth classifications of II, III, and IV. Unresectability was judged according to advanced cancer extension or intolerable condition of patients based on computed tomography (CT), or magnetic resonance imaging (MRI), cholangiography, and positron emission tomography. We excluded patients who 1) were aged <20 years or >90 years and 2) had a history of biliary tract operation. This study was performed in accordance with ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Institutional Review Boards of Severance Hospital (IRB no. 4-2015-1072) and Seoul National University (IRB no. H-1303-105-475).
Technique
In this study, endoscopic retrograde cholangiopancreatography (ERCP) procedures were performed by eight experienced endoscopists with at least 5 years of experience and each having performed >1000 ERCP procedures. ERCPs were performed under conscious sedation with propofol and pethidine, while being monitored by either an anesthesiologist or endoscopist at the same time. All ERCPs were conducted according to fluoroscopic guidance to diagnose and manage obstruction using a large (4.2 mm) accessory channel duodenoscope (TJF-240; Olympus Optical Co., Ltd., Tokyo, Japan). Cannulation of the common bile duct was attempted with a conventional cannula (Contour ERCP cannula; Boston Scientific, Natick, MA, USA) with or without a guidewire or with a pull-type sphincterotome [Clever-cut (Olympus Optical) or Autotome RX 44 (Boston Scientific)]. A precut papillotomy was attempted upon trial failures of wire-guided cannulation using a pull-type sphincterotome.
After biliary cannulation and completion of cholangiography, two 0.035-inch-diameter guidewires were passed through the stricture and inserted into the left and right hepatic ducts. Location and length of the stricture were evaluated by cholangiogram. After identifying location and extent of malignant bile duct stricture, endoscopists decided which stents [Niti-S large cell D-type stent® (Taewoong Medical, Gimpo, Korea), Wallstent® (Boston Scientific Co.), or Hanarostent® (M.I.Tech, Pyeongtaek, Korea)] to apply. Two SEMSs were inserted via SIS placement. Endoscopic bilateral SIS placement using SEMSs was performed as follows: The first stent was inserted and slowly deployed into the left intrahepatic duct over the guidewire. The second stent was deployed through the mesh of the first stent, such that the two stents overlapped in the common hepatic duct and branched into hepatic ducts, forming a Y-shape (Fig. 1). The lengths of SEMSs were chosen on the basis of the maximum size necessary to span the stenotic area; the diameter of SEMSs was 10 mm.

Follow-up and definition
Enrollment was defined as the date of first bilateral stent placement. Before the procedure and during follow up at 2 weeks and 4 weeks after the procedure, all patients underwent laboratory testing, including complete blood count and blood biochemistry. Radiological examinations, including abdominal ultrasonography, CT, or MRI, were performed at fixed intervals (1 or 2 months) or when stent dysfunction was suspected, such as elevated total bilirubin or clinical features suggestive of cholangitis (e.g., fever with signs of jaundice and right upper quadrant pain).
The primary outcome was stent patency duration. Stent patency duration was defined as the time interval between SEMSs insertion and stent occlusion or death. The secondary outcomes were technical success, functional success, complications, risk factors related to stent occlusion, and overall survival. Technical success was defined as appropriate stent positioning at the stricture site and immediate biliary decompression. Functional success was defined as a decrease in bilirubin level to less than 75% of the pretreatment value within the first month. Immediate and early complications, such as cholangitis, pancreatitis, and bleeding, were defined as procedure-related complications occurring within 72 h and after 72 h, but within 30 days of stent placement, respectively. Moreover, late complications were defined as procedure-related complications occurring after 30 days of stent placement. Stent occlusion was suspected in patients with abnormal laboratory parameters, such as serum bilirubin, liver transaminase, and/or alkaline phosphatase (ALP), and symptoms, such as jaundice, fever, and/or abdominal pain. Stent occlusion was diagnosed if patients had jaundice with evidence of elevated bilirubin levels and biliary dilation on imaging studies. Tumor ingrowth, tumor overgrowth, hemobilia, and occlusion secondary to sludge or food impaction were evaluated as reasons for stent occlusion. If a stent was occluded, repeat ERCP was performed to confirm the stent patency and manage the occlusion. Stent malfunction was defined when re-intervention was needed in cases of complications, such cholangitis and/or jaundice, elevated liver enzyme levels, and bile duct dilation. In cases of stent malfunction, a repeat endoscopic procedure for biliary drainage was performed using SEMSs or plastic stents. Percutaneous transhepatic biliary drainage was performed instead of endoscopic procedures only in cases of severe cholangitis that precluded endoscopy or failed bilateral stent placement. Overall survival was calculated from the day of SEMSs insertion to the day of last follow-up or death.
Statistical analysis
All data, including stent patency and survival, are expressed as a median (±standard deviation) or n (%), as appropriate. Mann-Whitney U-test was used for comparison of continuous variables, and chi-square test with Fisher's exact test was used for categorical variables. Cumulative stent patency and survival time were estimated using Kaplan-Meier analysis, and curves were compared with the log-rank test. To identify independent risk factors for stent occlusion and survival, univariate and subsequent multivariable Cox regression analyses were performed. All statistical analyses were performed using standard software (SPSS v23.0; IBM Corp., Armonk, NY, USA), with p<0.05 considered as statistically significant.
RESULTS
Patient characteristics
Seventy patients with MHBO underwent bilateral SIS placement between November 2009 and July 2016. The clinical characteristics of the patients are summarized in Table 1. Their median age was 68 years, and 38 patients (53.5%) were men. Median values of pre-stenting total bilirubin and pre-stenting ALP were 6.1±11.1 mg/dL and 450±355 IU/dL, respectively. Among study participants, histopathology was confirmed in 54 (76.1%) patients, and cancer types were as follows: cholangiocarcinoma (n=37, 52.9%), gallbladder cancer (n=22, 31.4%), and other cancers (n=11, 15.7%) including pancreatic and advanced gastric cancers. Bismuth classifications were as follows: type II (n=13, 18.6%), type III (n=17, 24.3%), and type IV (n=40, 57.1%). Among the participants, 35 (50.0%) underwent chemotherapy and three (6.4%) underwent radiotherapy after bilateral biliary stenting. Twenty-six patients underwent previous plastic stenting as a temporary placement. One patient underwent bilateral biliary stenting after removal of a previously inserted metal stent.
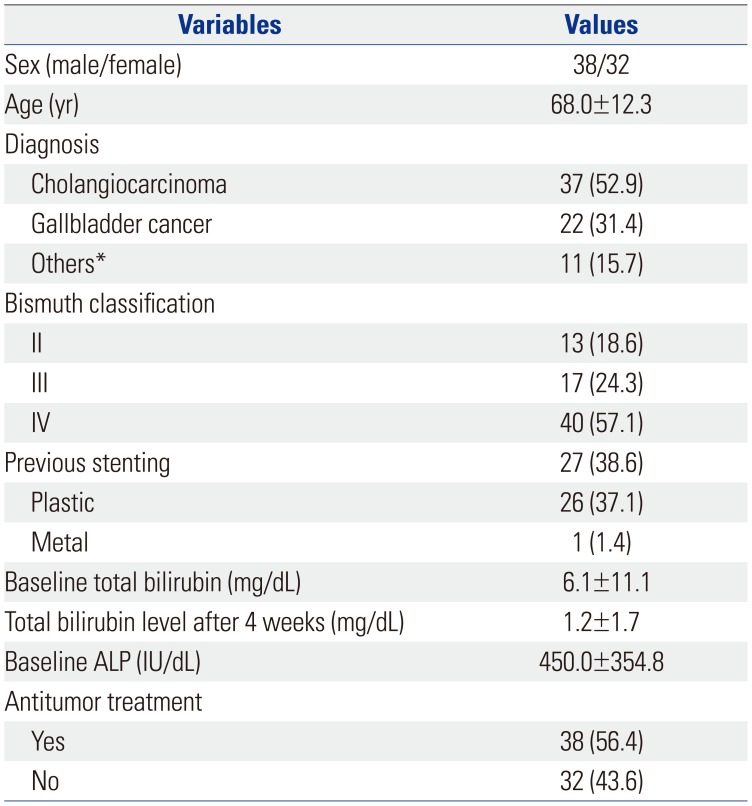
Table 1
Baseline Clinical Characteristics of Patients (n=70)
![]()
Outcomes
Outcomes for patients with bilateral metal stenting are shown in Table 2. The technical success rate was 98% (69/70), and the functional success rate was 85.5% (59/70). The cause of technical failure was stent deployment failure. Immediate complications occurred in nine (12.6%) patients. Four (5.6%) patients developed cholangitis, and five (5.6%) patients developed pancreatitis within 72 h of stent placement. Early complications occurred in eight (11.2%) patients, all of whom developed cholangitis within 30 days after of stent placement. Late complications did not occur in any patient. Cholangitis occurred in four patients as an immediate complication and in eight patients as an early complication. Ten cases were non-occlusion cholangitis and two cases were occlusion cholangitis. Ten patients underwent intervention, including temporary drainage or balloon sweeping, to resolve cholangitis. In two patients, cholangitis resolved spontaneously without any intervention. Patients with cholangitis and stent occlusion were documented simultaneously in number. During a median follow-up period of 140 days, stent occlusion occurred in 35 (50.0%) patients due to sludge (n=1), tumor ingrowth (n=29), tumor overgrowth (n=2), and unknown reasons (n=3). Seven patients received ERCP with sweeping using a basket and balloon, and 13 patients received stent reinsertion inside of the previously inserted metal stent (plastic stent in four patients and metal stent in nine patients). Nineteen patients underwent percutaneous transhepatic biliary drainage with or without stent insertion. During the observation period, no patient (0%) developed stent malfunction within 72 h of stent insertion, while three (3.2%) patients developed stent malfunction within 30 days after of stent placement. Fifteen (21%) patients developed stent malfunction after 30 days, requiring re-intervention.
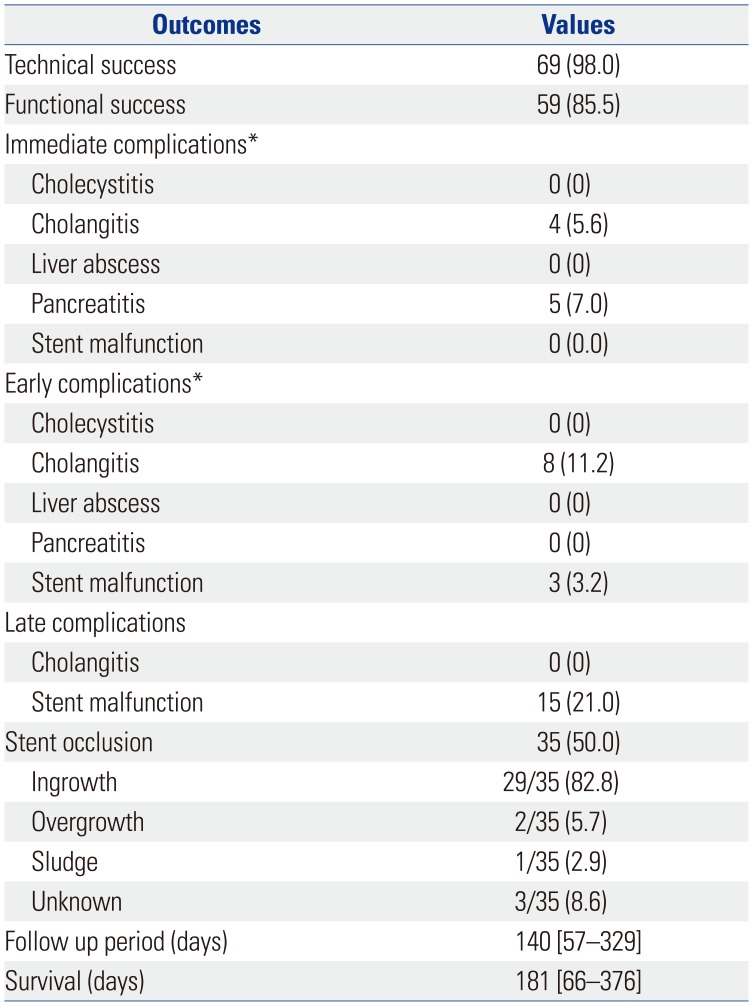
Table 2
Clinical Outcomes of Bilateral Metal Stents (n=70)
Variables are expressed as median [interquartile range] or n (%).
Stent malfunction was defined when re-intervention was needed in cases of complications, such cholangitis and/or jaundice, elevated liver enzyme levels, and bile duct dilation compared with previous CT images.
*Immediate complication, within 72 h of stent placement; early complication, after 72 h but within 30 days of stent placement.
![]()
Stent patency
Cumulative stent patency analyzed by the Kaplan-Meier method is depicted in Fig. 2, and median stent patency was 108 days. Univariate analysis showed Bismuth type IV (vs. II, III), immediate complication, and baseline bilirubin (>6.1 mg/dL) to be predictors of stent occlusion (all p<0.1). To avoid potential multicollinearity and to consider the possibility of immediate complication as procedure-related complication, immediate complication and bismuth type were separately incorporated into multivariate analyses. After adjusting for other variables, high bilirubin level (>6.1 mg/dL) was identified as an independent predictor of stent obstruction (Table 3). In this study, although results indicated immediate complication as an independent risk factor related to stent patency, it could be considered as a confounding factor in some respect. In addition, we reanalyzed the results after excluding patients with immediate complication, as shown in Supplementary Tables 1 and 2 and Supplementary Figs. 1 and 2 (only online). In the present study, we selected the median value (6.1 mg/dL) of pre-stenting total bilirubin as a cut-off level for predicting stent occlusion and overall survival. No statistically significant difference in stent patency was observed between the two centers (p=0.114). For comparison, median stent patency rates reported by previous studies are shown in Supplementary Table 3 (only online).
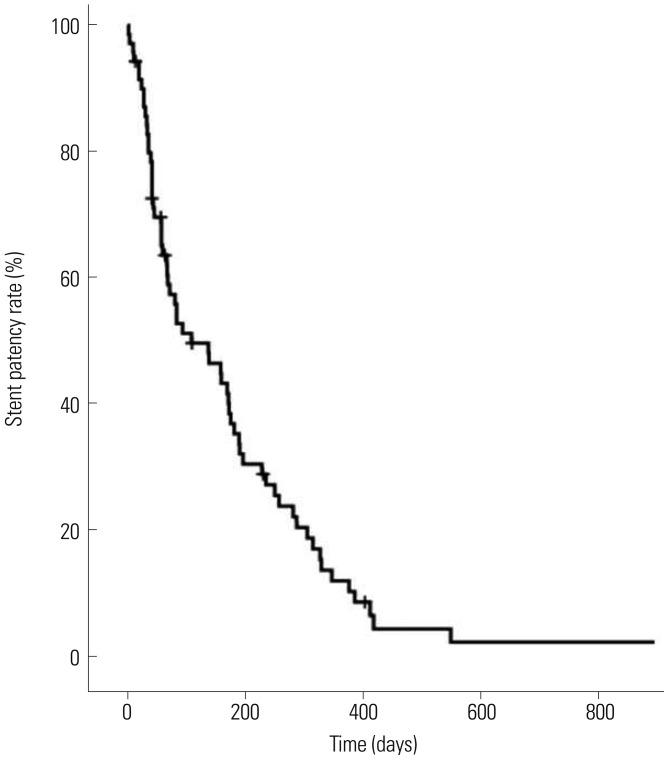
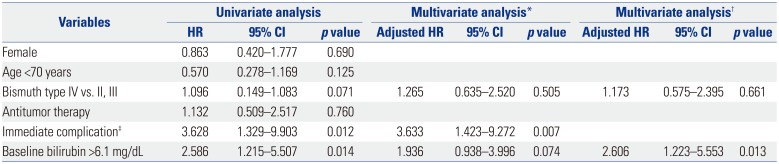
Fig. 2
Cumulative stent patency of bilateral hilar metal stent as analyzed by Kaplan-Meier curves. Median survival time analyzed by the Kaplan-Meier method was 108 days.
![]()
Table 3
Independent Factors Associated with Stent Patency of Bilateral Hilar Metal Stents in Cox Regression Analysis
![]()
Overall survival
Cumulative survival analyzed by the Kaplan-Meier method is shown in Fig. 3, and median survival time was 181 days. Cumulative survival was significantly better in patients with antitumor therapy than in those without, according to univariable Cox proportional hazards analysis [hazard ratio (HR) 0.56, 95% confidence interval (CI) 0.320–0.981; p=0.043]. In addition, patients with a pre-stenting bilirubin level of >6.1 mg/dL had worse survival than those with values <6.1 mg/dL in univariable Cox proportional hazard analysis (HR 2.15, 95% CI 1.181–3.914; p=0.012). However, neither antitumor therapy nor bilirubin level was a statistically significant prognostic factor in multivariate analysis (Table 4).
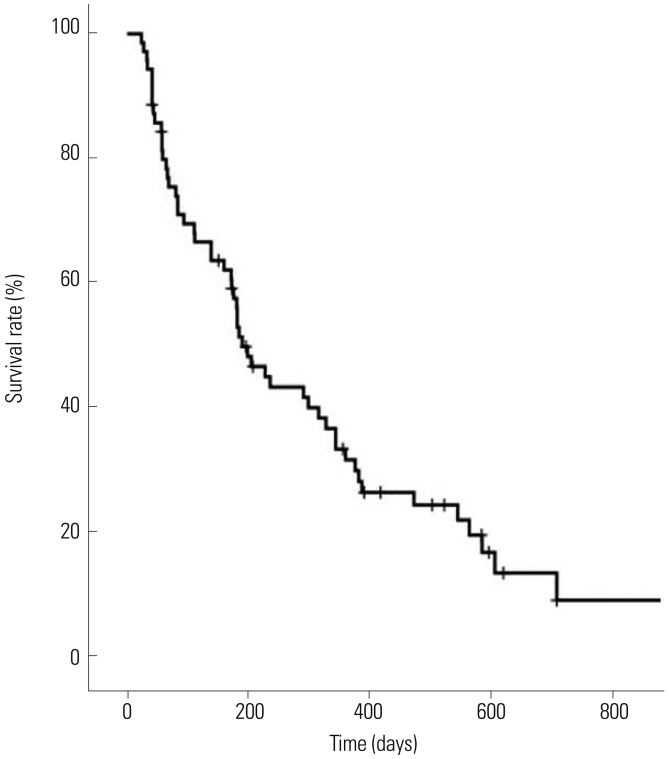

Fig. 3
Kaplan-Meier curve of patient overall survival after placement of bilateral metal stent. Median survival time analyzed by Kaplan-Meier method was 181 days.
![]()
Table 4
Independent Factors Associated with Survival after Placement of Bilateral Hilar Metal Stents in Cox Regression Analysis
![]()
DISCUSSION
Endoscopic biliary drainage is a major strategy for MHBO as it is a less invasive, more convenient, and a more physiological procedure, compared to a percutaneous approach or surgical bypass.1819 Previous studies have reported median stent patency rates ranging from 134 to 238 days (Supplementary Table 3, only online). In the present study, stent patency duration and median overall survival rate were shorter than those reported in previous studies (108 days and 181 days, respectively). The results could be explained by a difference in the proportion of high-grade hilar biliary obstructions in the present study (Bismuth type IV, 57.1%), as patients with high-grade biliary obstruction are at high risk for recurrent biliary drainage.20
It is important to know the risk factors associated with short stent patency in SIS method. In the present study, a pre-stenting higher total bilirubin level and the presence of immediate complications were independent risk factors related to stent patency duration in patients with MHBO. To evaluate the variable factors that influence stent patency, Naitoh, et al.12 reported that antitumor therapy was associated with a significantly longer stent patency in multivariable analysis, even if the difference was not statistically significant in the present study. Miura, et al.2021 reported that baseline bilirubin and cholangitis before SEMS placement were risk factors for recurrent biliary obstruction after SEMS placement in patients with MHBO. Higher total bilirubin reflects progression of tumor, and advanced tumor is likely to occlude inside of metal stent. Furthermore, patients with immediate complications eventually presented with cholangitis with occlusion. Only 56.4% of patients received chemotherapy, which could have an effect on patient survival. In univariate analysis, antitumor treatment was an independent factor related to survival; however, multivariable analysis did not confirm the result. In patients who are diagnosed with cholangiocarcinoma, the most common cause of death is infectious complication related to bile duct obstruction, such as biliary sepsis.2223 Therefore, after adjusting for bile duct obstruction related factors, antitumor treatment might not be an independent prognostic factor.
A previous study showed that one of the problems of the SIS method, compared to side-by-side (SBS) method, may be short stent patency. However, in regards to stent patency of the SIS method, comparison to the SBS method is still controversial.1213 To date, there are no randomized controlled trials comparing SBS and SIS. Regarding SIS method, previous studies showed discrepancy in the duration of stent patency.691011121314152425 A major problem of these previous retrospective studies was a difference in the mechanical properties of SEMSs, with various high axial and radial forces.262728 Also, there were differences in the definitions of stent occlusion, such as biliary obstruction or patient death, for those without biliary obstruction. If obstruction was not evident during a patient's life, patency period was equal to survival period, but with censored data. In contrast, some studies have shown the median duration of biliary obstruction after stent insertion.
This study had several limitations. First, this study was a non-randomized, retrospective study with a small sample size. However, since tumors of the biliary tract are relatively uncommon, 70 patients is a decent sample size for this particular population, and 70 patients with malignant hilar obstruction is quite a large sample size. Therefore, the present study does hold clinical relevance. Secondly, this study was not a comparative study between groups. However, the present study was performed in two large-volume centers, where biliary drainage was mostly done, using the SIS method in unresectable MHBO. Therefore, this study could minimize selection bias between SIS and SBS methods.
In conclusion, higher baseline bilirubin (>6.1 mg/dL) was found to be an independent risk factor related to stent patency. The SIS method still remains a controversial option with short stent patency for high-grade MHBO. Further studies are required to improve stent patency using new methods or newly designed stents in patients with high-grade biliary obstruction with severe jaundice.
 XML Download
XML Download