

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Overall survival after breast-conserving surgery (BCS) and adjuvant breast irradiation is equivalent to that after mastectomy for stage I or II breast cancer (12). However, the probability of local recurrence is higher in patients treated with BCS compared with those undergoing radical mastectomy (2). A positive resection margin at the time of BCS is associated with a substantially higher local recurrence rate (345). A positive resection margin is defined by the presence of invasive carcinoma or ductal carcinoma in situ (DCIS) at the inked margin of the resected specimen (46). In previous studies, several factors such as younger age, larger tumor size, positive lymph nodes, multifocal tumors, lobular histology, and the percentage of in situ components were associated with a positive resection margin (789101112).
Breast magnetic resonance imaging (MRI) has been widely used for the preoperative evaluation of tumor extent in patients with confirmed breast cancer. Previous studies reported that preoperative breast MRI altered the surgical management in approximately 20–30% of patients with breast cancer, leading to a decrease in reoperation rates and an increase in radical mastectomy rates (1314). The high sensitivity of breast MRI for cancer detection is presumed to improve the selection of patients for BCS and decrease the rates of a positive resection margin at the first BCS attempt (15). However, there is increasing concern that false-positive findings on preoperative MRI may lead to overtreatment in patients switching from BCS to radical mastectomy, without a clear survival benefit.
Therefore, it is important to determine the preoperative MRI findings and clinicopathological features associated with a positive resection margin during BCS. The purpose of our study was to determine the factors that are associated with a positive resection margin at the time of BCS in patients with breast cancer, with an emphasis on preoperative breast MRI findings.
Go to : 
MATERIALS AND METHODS
Patients
This retrospective study was approved by our Institution (Gangnam Severance Hospital) Review Board for clinical studies, and the need for obtaining individual consent from the subjects was waived. Between January 2015 and December 2015, we identified 153 consecutive women who had undergone BCS due to breast cancer, invasive cancer, or DCIS, and screened with preoperative MRI. Women receiving chemotherapy prior to surgery (n = 2), those who underwent local excisional biopsy before preoperative MRI (n = 24), and those lacking medical records associated with human epidermal growth factor receptor 2 (HER2) status (n = 7) were excluded. Finally, a total of 120 patients who had undergone BCS (mean age, 53.3 years; age range, 27–79 years) were included in our study.
Histopathologic and Immunohistochemical Analysis
Final histopathological results of the surgical specimens were reviewed to determine the tumor size of both the invasive component alone, and the invasive and in situ components, the presence or absence of lobular histology, lymphovascular invasion (LVI), and immunohistochemical status. If the final diagnosis was DCIS, the size of the invasive component was recorded as zero. Estrogen receptor (ER) and progesterone receptor (PR) expression was recorded (negative or positive). HER2/neu (HER2) staging was scored as 0 (negative; no staining), 1+ (negative; faint/barely perceptible incomplete membrane staining), 2+ (equivocal; weak-to-moderate complete membrane staining in > 10% of the tumor cells or strong complete membrane staining in < 30% of the tumor cells), or 3+ (positive; strong complete membrane staining in > 30% of the tumor cells) according to the guidelines of the American Society of Clinical Oncology/College of American Pathologists (16). Tumors scoring 2+ required further examination using silver-enhanced in situ hybridization (SISH) to measure HER2 amplification. A HER2/chromosome 17 ratio greater than 2.2 by SISH indicated HER2 positive status.
TNM staging was also conducted based on the seventh American Joint Committee on Cancer guidelines (17). Sentinel node biopsies or axillary nodal dissections were performed, and the N stage was recorded.
Lesion Localization and Evaluation of Resection Margin
Preoperative tumor localization for nonpalpable lesions was performed by two radiologists (with 5 years and 9 years of experience in breast imaging, respectively) with either mammographically or ultrasound-guided wire placement into the tumor. In cases of non-palpable tumors with microcalcifications, specimen mammography was performed to confirm adequate resection. Intraoperative margin excision and frozen section analysis were performed to evaluate intraoperative margins in all patients. A positive surgical margin was defined as the presence of tumor cells at the inked surface of the resected specimen. The margin was considered negative, in the absence of cancer cells on the inked surface of the resected specimen. We classified the following cases as a positive resection margin: 1) re-excision for positive frozen section analysis during BCS, 2) conversion from attempted BCS to mastectomy, and 3) requirement for further surgical excision.
MR Technique
Breast MRI was performed using a 3T system (Achieva, Philips Medical System, Best, the Netherlands; Discovery MR 750, GE Healthcare, Waukesha, WI, USA) with a dedicated, sensitivity encoding (SENSE), four-channel breast coil. All images were acquired with bilateral axial views in the prone position. The protocol included turbo spin-echo T1- and T2-weighted images and T2-weighted fat suppressed spin-echo series. Dynamic contrast-enhanced MRI was performed with one pre-contrast and five post-contrast dynamic series using a fat-suppressed T1-weighted gradient echo sequence (TR/TE: 4.9/2.4; matrix, 340 x 340; flip angle, 12°; field of view, 34 x 34 cm; slice thickness, 1.5 mm). The acquisition time of each post-contrast series was 74 seconds after a bolus injection of 0.1 mmol gadobutrol (Gadovist, Bayer Healthcare, Berlin, Germany) per kilogram of body weight via an automated injector (Nemoto, Nemoto Kyorindo, Tokyo, Japan), at a rate of 2 mL/s, followed by a 20-mL saline flush. After the examination, subtraction images were obtained by subtracting the unenhanced images from all contrast-enhanced images.
MRI Analysis
Two radiologists (with 5 years and 20 years of experience in breast MRI interpretation, respectively) reviewed the breast MR images in consensus according to the American College of Radiology breast imaging reporting and data system (ACR BIRADS) MRI lexicon (18). The largest diameters of enhancing lesions were measured in the axial plane of early post-contrast fat-suppressed T1-weighted images and subtraction images. Multifocal cancer was defined as the presence of two or more cancer lesions in the same quadrant, which were separated by normal breast parenchyma. In cases of multifocal lesions, the maximal diameter was not the sum of their diameters, but rather the single largest diameter measured. According to the ACR BIRADS MRI lexicon, enhancing lesions were divided into 2 categories: a mass including foci and non-mass enhancement (NME). We categorized the 120 cases into 2 groups based on the patterns of enhancing lesions on breast MRI. These groups included: 1) mass without NME, 2) NME with or without mass. In patients with a mass, we additionally categorized the shape, margin, and internal enhancement of the mass according to the following criteria: 1) shape (oval, round, or irregular), 2) margin (circumscribed, irregular, or spiculated), and 3) internal enhancement (homogeneous, heterogeneous, rim enhancement, or dark internal septations). In patients with NME, we analyzed the distribution and internal enhancement patterns of the NME according to the following criteria: 1) distribution (focal, linear, segmental, or regional) and 2) internal enhancement patterns (homogeneous, heterogeneous, clumped, or clustered ring). We also assessed breast parenchymal enhancement (BPE) using post-contrast fat-suppressed T1-weighted images and subtraction images. BPE was categorized as minimal, mild, moderate, or marked, and dichotomized into weak (minimal or mild) or strong (moderate or marked) enhancement for statistical analysis.
Statistical Analysis
The chi-squared test or Fisher's exact test was used to identify the association between each of the preoperative breast MRI findings or clinicopathological factors and the rate of positive resection margins. An independent two-sample t test was used for continuous normally distributed variables. Multivariate analysis was performed using logistic regression analysis of statistically significant variables (p < 0.100) via univariate analysis, and the odds ratios (ORs) were estimated. We considered p values less than 0.05 as statistically significant. SAS software (version 9.2, SAS Institute Inc., Cary, NC, USA) was used to perform the statistical analyses.
Go to :
RESULTS
The final histopathological results of the surgical specimens revealed invasive ductal carcinoma in 88 cases, DCIS in 8, invasive cribriform carcinoma in 6, mucinous carcinoma in 5, invasive lobular carcinoma in 3, medullary carcinoma in 3, apocrine carcinoma in 2, microinvasive ductal carcinoma with lobular carcinoma in 1, invasive solid papillary carcinoma in 1, high-grade sarcoma in 1, glycogen-rich clear cell carcinoma in 1, and metaplastic carcinoma in 1 case.
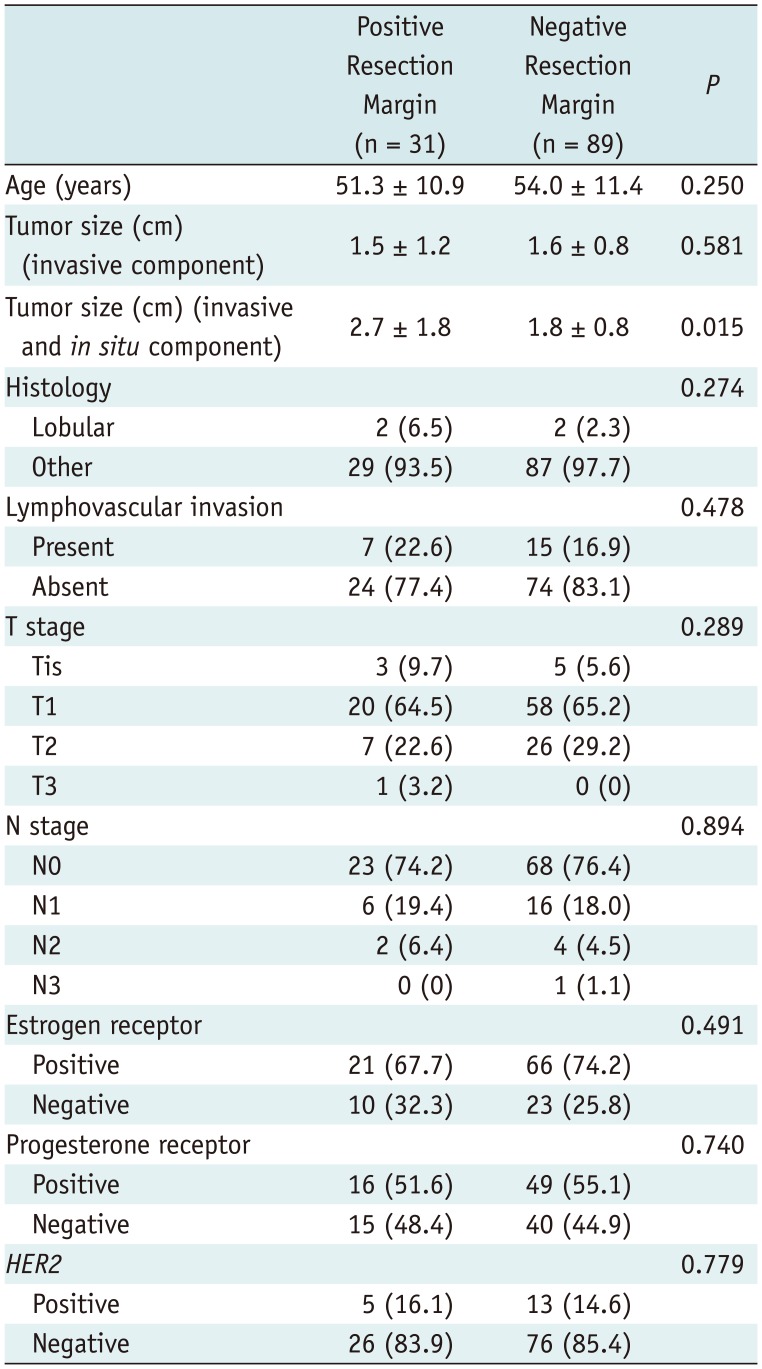
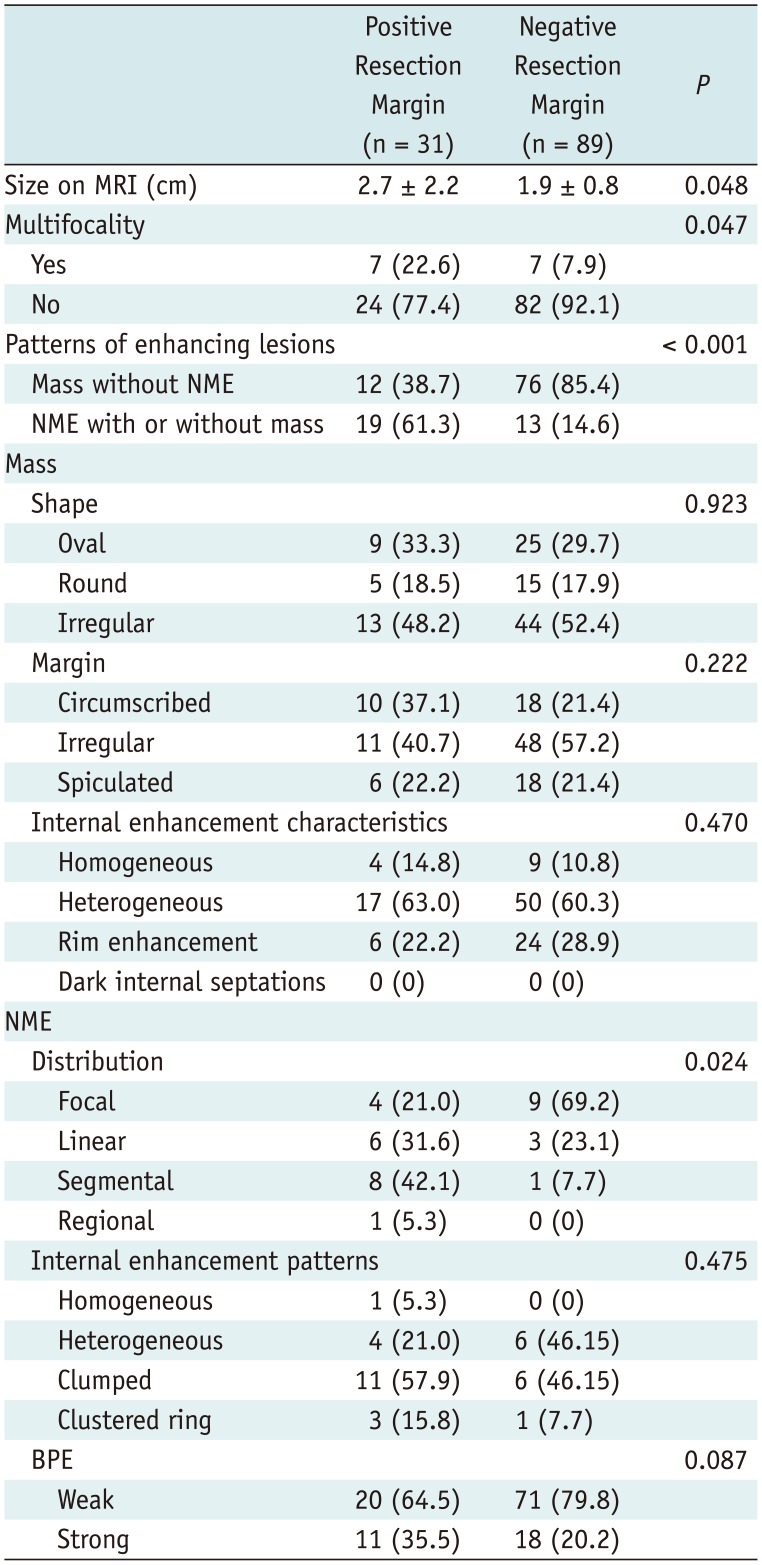
Among the 120 patients, 31 (25.8%) showed a positive resection margin, and 89 (74.2%) had a negative resection margin. Among the 31 cases with a positive resection margin, 17 (54.8%) underwent re-excision for positive frozen section analysis during BCS, 8 (25.8%) received additional local excision, and 6 (19.4%) underwent converted total mastectomy from attempted BCS. The mean tumor size of invasive and in situ component was significantly larger in the positive resection margin group compared with the negative resection margin group (2.7 cm vs. 1.8 cm; p = 0.015). Age, size of the invasive component of breast cancer, lobular histology, LVI, T stage, N stage, ER, PR, and HER2 status were not associated with positive resection margins (Table 1). The mean tumor size and multifocality of the tumor on MRI were associated with a positive resection margin (p = 0.048, p = 0.047, respectively). Patterns of enhancing lesions were also significantly associated with a positive resection margin (p < 0.001). Patients with a positive resection margin manifested a higher rate of NME with or without mass on preoperative breast MRI (61.3%) (Fig. 1). However, patients with a negative resection margin had a lower rate of NME with or without mass (14.6%). In cases with NME, the distribution was significantly associated with a positive resection margin (p = 0.024). Strong BPE was associated with a positive resection margin (p = 0.087) (Table 2).
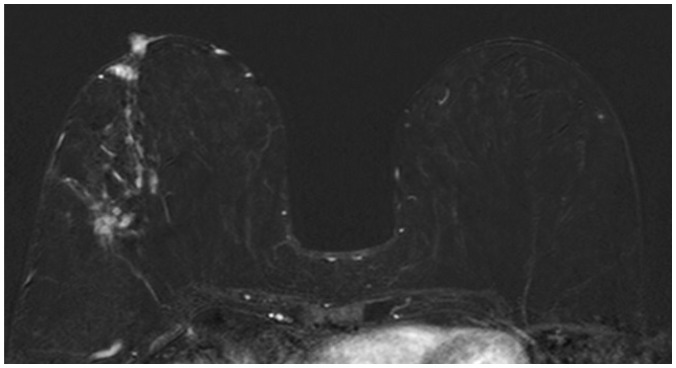 | Fig. 169-year-old woman with invasive solid papillary carcinoma.Preoperative contrast-enhanced T1-weighted subtraction images show segmental clustered ring non-mass enhancement in outer portion of right breast. Patient underwent total mastectomy, which was converted from attempted breast-conserving surgery since positive resection margin was obtained from frozen section analysis. Size of invasive and in situ component of tumor was approximately 3.7 cm. Patient tested positive for estrogen receptor, progesterone receptor and human epidermal growth factor receptor 2.
|
Table 1
Analysis of Associations between Clinicopathologic Factors and Positive Resection Margin
![]()
Table 2
Analysis of Associations between MRI Findings and Positive Resection Margin
![]()
Univariate logistic regression analysis of clinicopathological features revealed that the size of the invasive as well as in situ component of the tumor was associated with a positive resection margin (OR = 1.97; p = 0.004) (Table 3).
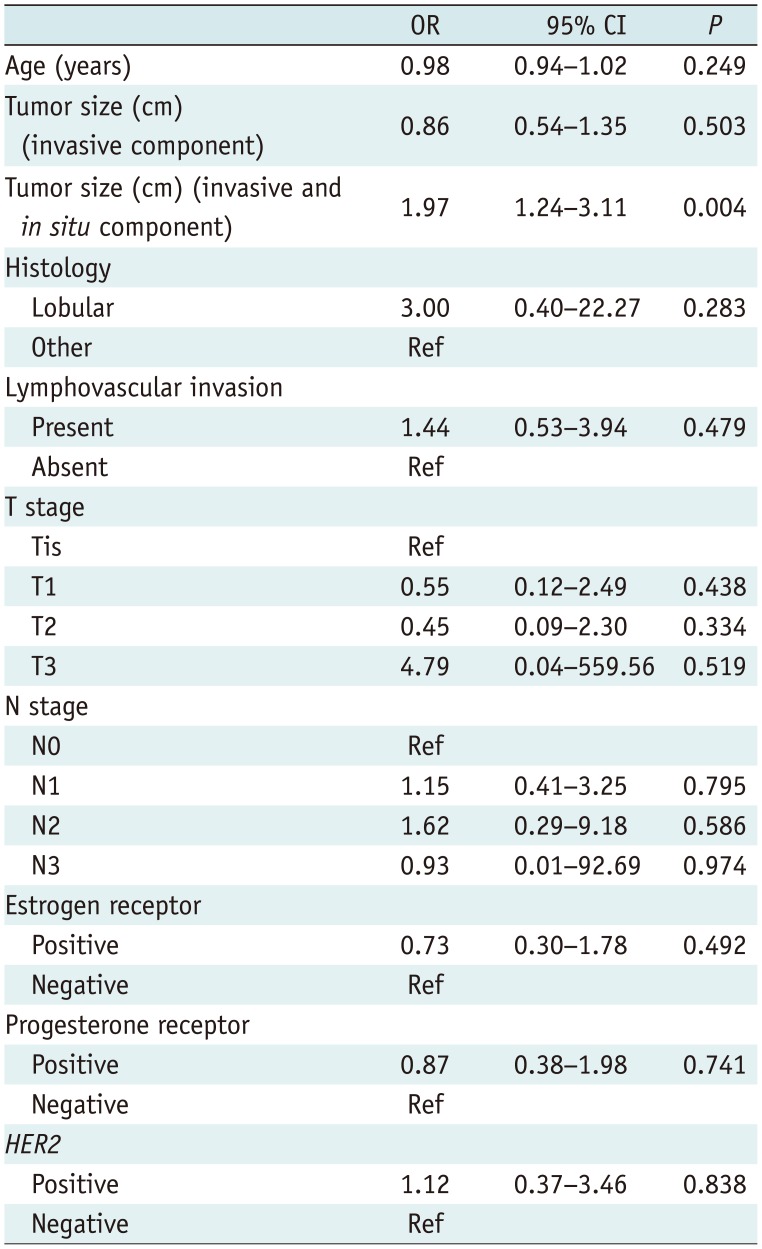
Table 3
Univariate Logistic Regression Analysis of Clinicopathologic Factors for Predicting Positive Resection Margin
![]()
Table 4 summarizes the results of univariate logistic regression analysis of MRI findings. Tumor size, multifocality, and NME with or without mass were associated with positive resection margins (OR = 1.63; p = 0.015, OR = 3.42; p = 0.035, OR = 9.26; p < 0.001, respectively). In particular, NME with segmental distribution was strongly associated with a positive resection margin (OR = 11.96, p = 0.025).
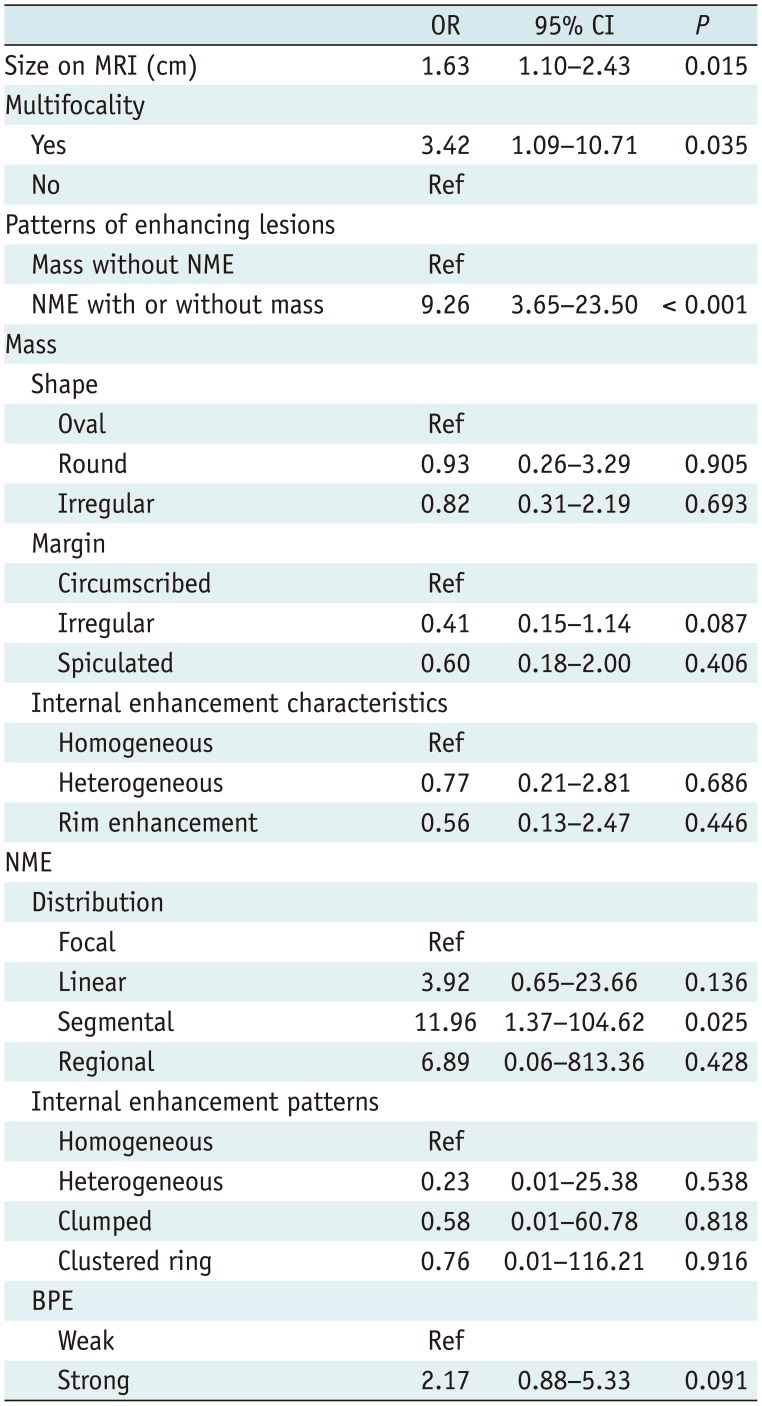
Table 4
Univariate Logistic Regression Analysis of MRI Findings for Predicting Positive Resection Margin
![]()
Patterns of enhancing lesions were significantly associated with a positive resection margin. In terms of patterns of enhancing lesions, NME with or without mass was independently predictive of a positive resection margin (OR = 7.00; p < 0.001). Strong BPE was also a weak predictor of positive resection margin (OR = 2.59; p = 0.076) (Table 5).
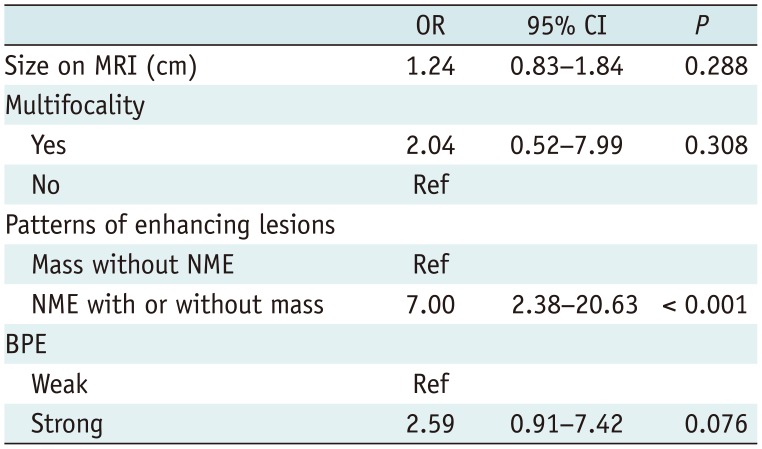
Table 5
Multivariate Analysis of MRI Findings for Predicting Positive Resection Margin
![]()
Go to :
DISCUSSION
Currently, BCS is the standard treatment for breast cancer in its early stages. However, a positive resection margin at the time of BCS is associated with a considerably higher risk of local tumor recurrence (34). The rate of positive resection margin in our study was 25.8% (31/120) which was within the reported range of 20–70% in the literature (319). Larger tumor size, lobular histology, presence of in situ components, younger age, multifocal lesions, and LVI are associated with a positive margin (789101112). Consistent with previous reports, the size of the invasive as well as in situ tumor component was associated significantly with a positive resection margin in our study (OR = 1.97; p = 0.004). However, younger age and lobular histology (only 4 cases out of 120) were not associated with positive resection margin in our study, probably due to the small number of cases.
The role of preoperative MRI in reducing the rate of positive resection margin in patients with breast cancer treated with BCS is disputed. Turnbull et al. (20), in a recent randomized controlled trial, reported that addition of preoperative breast MRI was not significantly associated with reduced reoperation rate. Houssami et al. (21), in a meta-analysis of 9 studies, reported that exposure to preoperative breast MRI increased the overall mastectomy rate (25.5% vs. 18.2%; OR, 1.54 [p < 0.001]; adjusted OR, 1.51 [p < 0.001]) and failed to reduce the rate of re-excision surgery in patients with initial breast conservation (11.6% vs. 11.4%; OR, 1.02 [p = 0.87]; adjusted OR, 0.95 [p = 0.71]). On the other hand, Pengel et al. (22) reported that preoperative MRI was significantly associated with a lower rate of incomplete excision in patients with invasive ductal carcinoma. Mann et al. (23) found that preoperative breast MRI reduced the rate of re-excision without increasing the mastectomy rate in patients with invasive lobular carcinoma.
With regard to the MRI features associated with resection margin positivity after BCS, according to Kim et al. (24), the single NME group showed the highest re-excision rate after BCS (22.2%, p = 0.02). Jang et al. (25) found that a tumor size exceeding 5 cm (OR = 3.81), NME (OR = 2.96), and multifocal lesions (OR = 2.54) on preoperative MRI were positively associated with re-excision. For NME lesions, the segmental distribution pattern predicted re-excision (OR = 10.53) (25). Similar to a previous study, NME with or without mass was an independent predictor of a positive resection margin compared with mass without NME (OR = 7.00, p < 0.001). Notably, the segmental distribution of NME was strongly associated with a positive resection margin (OR = 11.96, p = 0.025). The association between NME and resection margin positivity might be explained by the presence of a DCIS component manifesting as NME. DCIS more commonly presented as NME than mass and many DCIS lesions exhibit segmental or ductal distribution and a clustered ring or clumped internal enhancement (262728). Furthermore, many studies have reported that the presence of a DCIS component was significantly associated with a positive resection margin (2529303132). Thus, radiologists should be aware that NME on preoperative breast MRI increases the possibility of subsequent positive resection margin status.
In this study, multifocal cancer on MRI was correlated with positive resection margin in univariate analysis, but not in multivariate analysis, which might be explained by the routine use of multiple wire localization for multifocal, nonpalpable lesions in our hospital.
Additionally, a strong BPE was associated with a positive resection margin with borderline significance (OR = 2.59, p = 0.76) in our study, similar to a previous study in which strong BPE was a significant independent factor for positive resection margin (OR = 2.39) (33). BPE varies in degree and distribution in different patients as well as in the same patient over time. Moderate or marked BPE may yield false-positive or false-negative results, and has been associated with abnormal interpretation compared with minimal or mild BPE, especially in the presence of focal, regional, or asymmetric BPE (3435). Small additional masses or NME around the index cancer may be masked by adjacent enhancing breast tissue leading to a false-negative interpretation (3536).
There are several limitations to this study. First, because of its retrospective design, patient selection bias might have occurred. We identified 153 consecutive patients with breast cancer who had undergone preoperative MRI and BCS. The patients whose initial surgical plan was switched from BCS to mastectomy due to unfavorable preoperative MRI findings were excluded. Furthermore, 33 (21.6%) of the 153 patients were excluded because they underwent chemotherapy prior to surgery, had a local excisional biopsy, or lacked medical records showing HER2 status. Second, we did not correlate the MRI findings with the pathologic findings comprehensively. Further studies correlating MRI and pathological findings are needed.
In conclusion, this study found that NME with or without mass detected on preoperative breast MRI was an independent predictive factor for a positive resection margin. More specifically, NME with segmental distribution was strongly correlated with a positive resection margin. In addition, strong BPE was associated with a positive resection margin with borderline significance. Among clinicopathologic factors, the size of the invasive and in situ component of the tumor was significantly associated with a positive resection margin. These factors facilitate patient selection and determination of the extent of resection during BCS.
Go to :
 XML Download
XML Download